










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.109 n.10 Pretoria Oct. 2019
http://dx.doi.org/10.7196/samj.2019.v109i10.13707
RESEARCH
Projecting the fiscal impact of South Africa's contraceptive needs: Scaling up family planning post 2020
L CholaI; K MacQuilkanII; A WinchIII; R RapitiII; I EdokaIV; C Kohli-LynchII; K HofmanV
IPhD; School of Public Health, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IIMSc; SAMRC/Wits Centre for Health Economics and Decision Science, PRICELESS SA, School of Public Health, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IIIMSc; Global Health and Development, Imperial College, London, UK
IVPhD; SAMRC/Wits Centre for Health Economics and Decision Science, PRICELESS SA, School of Public Health, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
VMB BCh, FAAP;AMRC/Wits Centre for Health Economics and Decision Science, PRICELESS SA, School of Public Health, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
ABSTRACT
BACKGROUND. Evidence-informed priority setting is vital to improved investment in public health interventions. This is particularly important as South Africa (SA) makes the shift to universal health coverage and institution of National Health Insurance.
OBJECTIVES. To measure the financial impact of increasing the demand for modern contraceptive methods in the SA public health sector. We estimated the total cost of providing contraceptives, and specifically the budgetary impact of premature removals of long-acting reversible contraceptives.
METHODS. We created a deterministic model in Microsoft Excel to estimate the costs of contraception provision over a 5-year time horizon (2018 - 2023) from a healthcare provider perspective. Only direct costs of service provision were considered, including drugs, supplies and personnel time. Costs were not discounted owing to the short time horizon. Scenario analyses were conducted to test uncertainty.
RESULTS. The base-case cost of current contraceptive use in 2018 was estimated to be ZAR1.64 billion (ZAR29 per capita). Injectable contraceptives accounted for ~47% of total costs. To meet the total demand for family planning, SA would have to spend ~30% more than the estimate for current contraceptive use. In the year 2023, the 'current use' of modern contraceptives would increase to ZAR2.2 billion, and fulfilling the total demand for family planning would require ZAR2.9 billion. The base-case cost of implantable contraceptives was estimated at ZAR54 million. Assuming a normal removal rate, the use of implants is projected to increase by 20% during the 5-year period between 2019 and 2023, with an estimated 46% increase in costs. The cost of early removal of Implanon NXT is estimated at ZAR75 million, with total contraception costs estimated at ZAR102 million in 2019, compared with ZAR56 million when a normal removal rate is applied.
CONCLUSIONS. The costs of scaling up modern contraceptives in SA are substantial. Early and premature removals of implantable contraceptives are costly to the nation and must be minimised. The government should consider conducting appropriate health technology assessments to inform the introduction of new public health interventions as SA makes the shift to universal health coverage by means of National Health Insurance.
Contraception is one of the most important tools for development in any country, as it has a profound impact on individual, family and societal wellbeing.[1] Increasing contraception can lead to a reduction in maternal and child mortality and HIV/AIDS.[2] It contributes to economic growth by increasing universal education, promotion of gender equality and environmental sustainability, and ultimately reduces poverty and hunger.[3,4]
Improving sexual and reproductive health therefore remains a key development goal for the South African (SA) government, which has committed to making modern contraceptives more accessible to women by 2020[5] and ensuring universal access to sexual and reproductive healthcare by 2030.[6] In the SA public sector, contraceptives are provided without charge to women who need them. Nationally, contraceptive choice is enhanced by the availability of a wide range of options, which was boosted by the introduction of the subdermal implant (Implanon and Jadelle) in 2014.[7] The implant was introduced in an effort to increase access to long-acting reversible contraceptives (LARCs), which have been shown to be very effective family planning options, reducing the need for user adherence and relieving pressure on health facilities, as contacts with health workers are fewer.[8] However, there have been challenges with the roll-out of LARCs in SA.[9] Approximately 1% of sexually active women use intrauterine devices, and although the use of implants has increased to ~4% in recent years, there has been a sharp decline in their uptake.[10] Early and premature removals of implants are also on the increase, mainly as a result of intolerable side-effects.[9,11,12]
With the SA government seeking to expand contraceptive coverage to all women in need,'5,61 it is important that the economic and financial implications of scaling up family planning are fully understood. Previous estimates of the costs of scaling up family planning in SA have not taken into consideration the inherent system challenges that could ultimately make cost-effective interventions such as LARCs unaffordable.[13,14]
Objectives
To measure the financial impact of increasing the demand for modern contraceptive methods in the SA public health sector over a 5-year time horizon. Focus was placed on the roll-out of the implant to show the financial impact of premature and early removals. To the best of our knowledge, such analyses were not done prior to the roll-out of any contraceptive methods in SA, and we aim to show the importance of financial considerations in the implementation of health interventions, particularly as the nation strives to attain universal health coverage.
Methods
A deterministic model was developed in Excel 2013 (Microsoft, USA) to estimate the financial impact of contraceptive provision in the public sector, from a provider perspective. The analysis only considered modern contraceptive methods and was undertaken on the population of sexually active women aged 15 - 49 years (we combined the proportions of currently married and sexually active unmarried women). Baseline data on family planning, including the contraceptive prevalence rate, unmet need for family planning, demand for family planning and modern contraceptive use, were obtained from the 2016 South Africa Demographic and Health Survey.[10] Population estimates were from the Statistics South Africa mid-year population projections.[15]
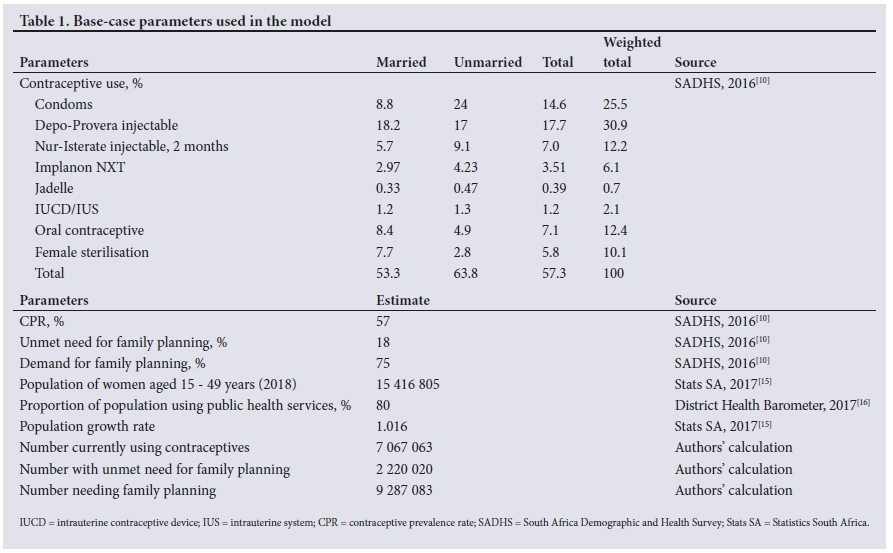
Table 1 shows the parameters used in the analysis. We used a contraceptive prevalence rate (CPR) of 57% for all sexually active women. The Depo-Provera injectable was the most commonly used contraceptive (18%), and Jadelle was the least common at 0.4%. The unmet need for family planning was 18%. The combined demand for family planning, which is the sum of the unmet need and the CPR, was therefore 75%. In the analysis, the weighted total contraceptive use among married and unmarried sexually active women was used to estimate total costs.
With the population in the first year of analysis (2018) estimated at 12.3 million for the public sector, the total number of women using contraceptives was 7.1 million, and the number with an unmet need for family planning was 2.2 million.
The annual cost of providing each contraceptive method is shown in Table 2. Included in the calculation were costs of drugs and supplies and personnel time. Drug costs were obtained from the National Department of Health Master Procurement Catalogue of February 2018.[17] Personnel costs were based on the SA public sector salary structure for medical personnel.[18] The assumptions on materials used and personnel time to administer each contraceptive method were based on similar analyses in the OneHealth tool[19] and WHO-CHOICE.[20]

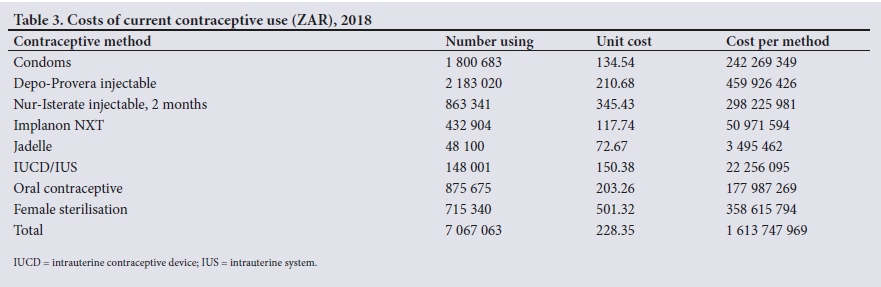
An average cost for provision of modern contraception was calculated by applying the weighted totals from Table 1 for each contraceptive method to the associated annual cost, giving a figure of ZAR228.35 (Table 2). The total cost of current contraceptive use was calculated as the product of the number currently using contraceptives (Table 1) and the weighted total cost (ZAR228, Table 2). The cost of fulfilling the current need (met and unmet) for family planning was estimated by multiplying the average cost by the current demand for family planning.
The financial impact of LARCs considered the impact of implantable contraceptives (Jadelle and Implanon) under two scenarios: normal removal and premature removal. Normal removal means that Implanon is removed and replaced every 3 years and Jadelle every 5 years. Premature removal is when the implants are removed before the prescribed period. A conservative estimate of 50%[21] was applied for early removal, and costs were calculated for the combination of early removals and normal removals. The removal rate was assumed to be the same for Implanon and Jadelle. It was further assumed that a patient whose implant had been removed would transfer to another modern contraceptive method, so the average cost for all contraceptives was added to the average cost for Implanon and Jadelle, resulting in an average cost for early removal of ZAR314.85 and ZAR117.74, respectively.
Contraceptive prevalence was assumed to increase at a rate of 0.03% per year.'101 An annual rate of 1.6% was used to project the growth in the population over time.'151 Costs were not discounted, given the short time horizon, and all base case costs are presented in 2018 prices. An annual inflation increment of 5% was assumed over the 3-year time horizon.
Results
Base-case costs of family planning
The total cost for all current contraceptive use in the public sector (for the year 2018) was estimated to be ZAR1.61 billion, a product of the average cost and the total number currently using contraceptives (Table 3). The model projected that injectables, Depo-Provera (ZAR460 million) and Nur-Isterate (ZAR298 million) would be the most costly, together accounting for ~47% of total costs. Condoms would cost ZAR242 million, and the Jadelle implant would cost the least at ZAR3.5 million. If the total demand for family planning was met (not shown in Table 3), total annual costs would rise to ZAR2.1 billion (~30% of current use costs).
Future changes in demand and costs of family planning
From an estimated 12.3 million in 2018, the number of women aged 15 - 49 years was projected to increase to 13.4 million in 2023 (Table 4). Of these women, 7.9 million would be using modern contraceptives, with the CPR estimated at 58.8%. Maintaining the demand for family planning at 75%, the total demand for family planning would be ~10.1 million in 2023. The total cost associated with contraceptive use in that year would be ZAR2.29 billion (met need), and the total cost of fulfilling the demand (met and unmet) for family planning would be ZAR2.93 billion.
The budget impact of LARCs
In the base-case scenario (2018), we estimated that 433 000 women were using Implanon and 48 000 were using Jadelle (not included in Table 4). The total demand for Implanon was estimated to be 567 000 and that for Jadelle 63 000. The projected total cost of 'current use' of Implanon was ZAR81.69 million and the total cost of fulfilling the demand for family planning was ZAR184.67 million. Jadelle was projected to have a much smaller impact owing to lower utilisation numbers and lower average cost; ZAR5.6 million for 'current use' and ZAR6.4 million for fulfilling the total demand.
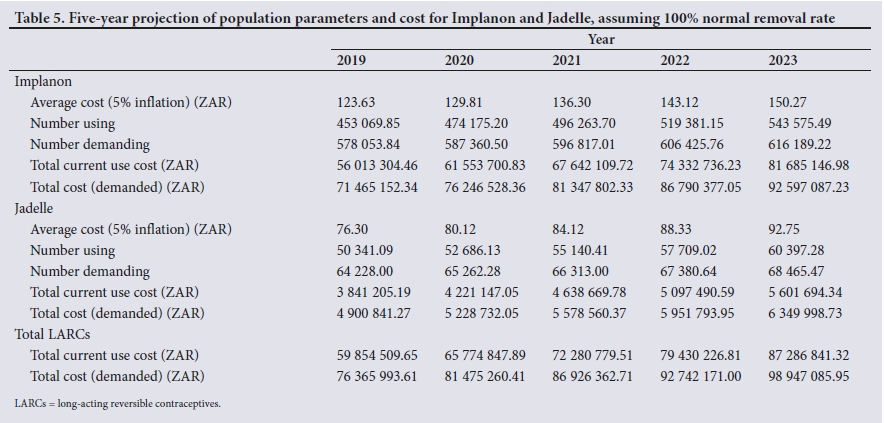
Assuming that all LARCs were removed at a normal rate between 2019 and 2023, the number using implantable contraceptives is projected to increase by 20% (from 453 000 to 543 000 for Implanon and from 50 000 to 60 000 for Jadelle), while the total demand for all contraceptives would increase by about 7% (Table 5). At this usage rate, the total cost of providing the implants (both Implanon and Jadelle) is estimated to be ZAR59 million in 2019 and ZAR87 million in 2023 (a 46% increase).
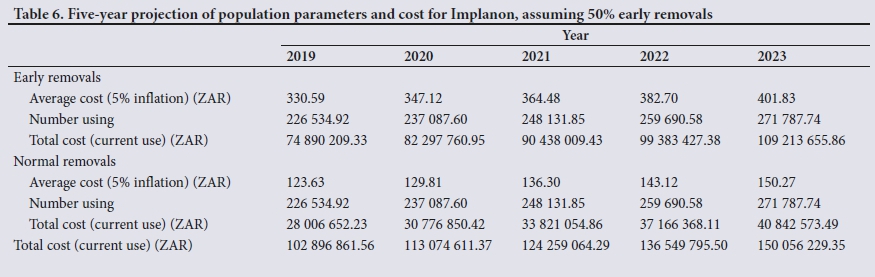
Table 6 shows the impact of early removals on the cost of Implanon. Assuming a 50% premature removal rate, the number of users decreases by 50%, e.g. in 2019 to 226 534 (from 453 069 as given in Table 5). The cost of early removal is estimated to be ZAR74.9 million in 2019. Added to the cost of normal removal, the total cost of Implanon in 2019 is ZAR102.9 million. This is 1.8 times more than the cost without premature removals estimated in Table 5.
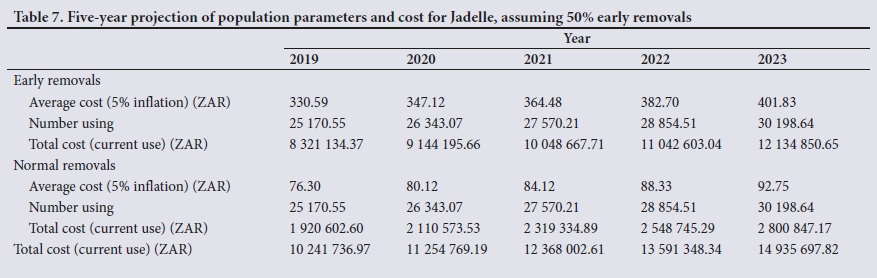
Similarly, the total cost for Jadelle when premature removals are taken into consideration almost triples, from ZAR3.8 million to ZAR10.2 million (Table 7).
Discussion
This article considers the financial impact of scaling up modern contraceptives in SA. Owing to the challenges that SA has experienced with rolling out LARCs,[9,11,12] the current and future impact on the national budget of continued premature removals of implantable contraceptives was analysed.
The results show that the total spend on contraception in SA is substantial, with base-case costs of current contraceptive use in 2018 estimated to be ZAR1.64 billion. This is ~1% of the national health budget, and about ZAR29 per capita at current population estimates. Injectable contraceptives account for ~47% of the total costs. To meet the total demand for family planning, SA would have to spend ~30% more than the estimate for current contraceptive use. By the year 2023, the 'current use' of modern contraceptives would increase to ZAR2.2 billion, and fulfilling the total demand for family planning would require ZAR2.9 billion.
The use of implantable contraception is currently about 3%,[10] and the current spend is estimated at ZAR54 million (2018). Assuming a normal removal rate, the use of implants is projected to increase by 20% during the 5-year period between 2019 and 2023, with an estimated 46% increase in costs. Premature removals affect both the demand for and cost of contraception. The demand decreases, but the total cost increases. For example, the cost of early removal of Implanon is estimated at ZAR75 million, with total contraception costs estimated at ZAR102 million in 2019, compared with ZAR56 million when a normal removal rate is applied.
Most studies that project the costs of family planning do not take into account the challenges of scaling up modern contraceptives.[13,14,22] The challenges are many, and include issues on both the demand and supply sides, such as concerns over side-effects, opposition from partners, inadequate logistics and insufficiently trained health workers.[23-25] The costs of addressing these challenges are likely to be substantial. In this current analysis, we only considered the cost of premature removals for implantable contraceptives. Other costs related to side-effects associated with this contraceptive method,[26] for example, are not taken into account. What we provide in this analysis is probably an underestimate of the full costs of contraceptive use.
The analysis in this article, however, is useful in that it provides costing and budgeting perspectives and makes the case for conducting assessments of new health technology interventions before they are introduced.[27] Appropriate economic evaluations should also probably include assessments of costs related to training, sensitisation and deployment. Technologies should also be targeted at population subgroups. In the case of implantable contraception, these devices should be provided to women who intend and are likely to use them for the entire prescribed period. While it is not easy to predict the biological and physiological reactions to contraception, users must be given full information on the possible consequences of the various contraceptive alternatives, to enable them to make better choices about family planning methods. These investments in sensitisation and education may initially be substantial, but they could be cost-saving in the long term.
Contraception is widely accepted to be beneficial and to have a positive effect on economic development. However, family planning should not be provided 'at all costs', and caution must be exercised when scaling up 'beneficial' interventions. In a country like SA, the opportunity cost of resource use is high, necessitating the need for evidence-based priority setting. Policymakers must move away from allocation of resources based on clinical effectiveness and safety alone. In this article, we show the importance of cost considerations in the planning process. While the analysis has its limitations, and even in instances where data challenges abound, useful and robust budget assessments can be provided to inform decision-making. More health systems research is need to establish the determinants of early contraceptive removal and its economic impact.
Declaration. None.
Acknowledgements. None.
Author contributions. LC, KM and AW conceptualised the analysis and designed the model, CKL, RR and IE suggested adjustments to the model, KM and AW collected the data, KH and LC conceptualised the basis of the manuscript, LC drafted the manuscript, and all authors read and revised the manuscript.
Funding. This research was supported by the SA MRC Grant D1305910-03, the SA MRC Grant D1305910-01 and the BMGF (grant OPP1087363) through iDSI.
Conflicts of interest. None.
References
1. Habumuremyi PD, Zenawi M. Making family planning a national development priority. Lancet 2012;380(9837):78-80. https://doi.org/10.1016/S0140-6736(12)60904-0 [ Links ]
2. Wilcher R, Cates W, Gregson S. Editorial: Family planning and HIV: Strange bedfellows no longer. AIDS 2009;23(Suppl 1):S1-S6. https://doi.org/10.1097/01.aids.0000363772.45635.35 [ Links ]
3. Canning D, Schultz TP. The economic consequences of reproductive health and family planning Lancet 2012;380(9837):165-171. https://doi.org/10.1016/S0140-6736(12)60827-7 [ Links ]
4. Longwe A, Smits J. The impact of family planning on primary school enrolment in sub-national areas within 25 African countries. Afr J Reprod Health 2013;17(2):23-38. https://www.jstor.org/stable/23485918 (accessed 15 April 2018). [ Links ]
5. FP2020. Accelerating progress: Strategy for 2016 - 2020. 2015. http://progress.familyplanning2020.org/ (accessed 15 April 2018). [ Links ]
6. United Nations. Sustainable Development Goals. 2015. https://sustainabledevelopment.un.org/?menu=1300 (accessed 15 April 2018). [ Links ]
7. Rees H, Pillay Y, Mullick S, Chersich MF. Strengthening implant provision and acceptance in South Africa with the 'Any woman, any place, any time' approach: An essential step towards reducing unintended pregnancies. S Afr Med J 2017;107(11):939-944. https://doi.org/10.7196/SAMJ.2017.v107i11.12903 [ Links ]
8. Winner B, Peipert JF, Zhao Q, et al Effectiveness oflong-acting reversible contraception. N Engl J Med 2012;366(21):1998-2007. https://doi.org/10.1056/NEJMoa1110855 [ Links ]
9. Adeagbo OA, Mullick S, Pillay D, et al. Uptake and early removals of Implanon NXT in South Africa: Perceptions and attitudes of healthcare workers. S Afr Med J 2017;107(10):822-826. https://doi.org/10.7196/SAMJ.2017.v107i10.12821 [ Links ]
10. Statistics South Africa. South Africa Demographic and Health Survey. Pretoria: Stats SA, 2016. https://dhsprogram.com/publications/publication-fr337-dhs-ffnal-reports.cfm (accessed 15 April 2018). [ Links ]
11. Pillay D, Chersich MF, Morroni C, et al. User perspectives on Implanon NXT in South Africa: A survey of 12 public-sector facilities. S Afr Med J 2017;107(10):815-821. https://doi.org/10.7196/SAMJ.2017.v107i10.12833 [ Links ]
12. Flore M, Chen X, Bonney A, et al. Patients' perspectives about why they have their contraceptive Implanon NXT device removed early. Aust Fam Physician 2016;45(10):740-744. https://www.racgp.org.au/afp/2016/october/patients%E2%80%99-perspectives-about-why-they-have-their-contraceptive-implanon-nxt-device-removed-early/ (accessed 5 September 2019). [ Links ]
13. McGee SA, Chola L, Tugendhaft A, et al. Strategic planning for saving the lives of mothers, newborns and children and preventing stillbirths in KwaZulu-Natal province South Africa: Modelling using the Lives Saved Tool (LiST). BMC Public Health 2016;16(49). https://doi.org/10.1186/s12889-015-2661-x [ Links ]
14. Chola L, McGee S, Tugendhaft A, Buchmann E, Hofman K. Scaling up family planning to reduce maternal and child mortality: The potential costs and benefits of modern contraceptive use in South Africa. PLoS One 2015;10(6):e0130077. https://doi.org/10.1371/journalpone.0130077 [ Links ]
15. Statistics South Africa. Mid-year Population Estimates. Pretoria: Stats SA, 2018. http://www.statssa.gov.za/?s=mid-year+population+estimates&sitem=publicatic (accessed 15 April 2018). [ Links ]
16. Massyn N, Padarath A, Peer N, Day C, eds. District Health Barometer 2016/17. Durban: Health Systems Trust, 2017. [ Links ]
17. National Department of Health, South Africa. Medicine Procurement List: Master Procurement Catalogue 2018. http://www.health.gov.za/index.php/component/phocadownload/category/196 (accessed 15 April 2018). [ Links ]
18. Department: Public Service and Administration, South Africa. Remuneration policy documents. 2018. http://www.dpsa.gov.za/dpsa2g/r_documents.asp (accessed 15 April 2018). [ Links ]
19. Stover J, McKinnon R, Winfrey B. Spectrum: A model platform for linking maternal and child survival interventions with AIDS, family planning and demographic projections. Int J Epidemiol 2010;39(Suppl 1):i7-i10. https://doi.org/10.1093/ije/dyq016 [ Links ]
20. Stenberg K, Lauer JA, Gkountouras G, Fitzpatrick C, Stanciole A. Econometric estimation of WHO-CHOICE country-specific costs for inpatient and outpatient health service delivery. Cost Eff Resour Alloc 2018;16:11. https://doi.org/10.1186/s12962-018-0095-x [ Links ]
21. Jacobstein R, Polis CB. Progestin-only contraception: Injectables and implants. Best Pract Res Clin Obstet Gynaecol 2014;28(6):795-806. https://doi.org/10.1016/j.bpobgyn.2014.05.003 [ Links ]
22. Halperin DT, Stover J, Reynolds HW. Benefits and costs of expanding access to family planning programs to women living with HIV. AIDS 2009;23(Suppl 1):S123-S130. https://doi.org/10.1097/01.aids.0000363785.73450.5a [ Links ]
23. Haider TL, Sharma M. Barriers to family planning and contraception uptake in sub-Saharan Africa: A systematic review. Int Q Community Health Educ 2013;33(4):403-413. https://doi.org/10.2190/IQ.33.4.g [ Links ]
24. Dansereau E, Schaefer A, Hernandez B, et al. Perceptions of and barriers to family planning services in the poorest regions of Chiapas, Mexico: A qualitative study of men, women, and adolescents. Reprod Health 2017;14(129). https://doi.org/10.1186/s12978-017-0392-4 [ Links ]
25. Eltomy EM, Saboula NE, Hussein AA. Barriers affecting utilization of family planning services among rural Egyptian women. East Mediterr Health J 2013;19(5):400-408. https://doi.org/10.26719/2013.19.5.400 [ Links ]
26. Bitzer J, Tschudin S, Alder J. Acceptability and side-effects of Implanon in Switzerland: A restrospective study by the Implanon Swiss Study Group. Eur J Contracept Reprod Health Care 2004;9(4):278-284. https://doi.org/10.1080/13625180400017503 [ Links ]
27. Battista RN, Lafortune L. Health technology assessment and public health: A time for convergence. Eur J Public Health 2009;19(3):227. https://doi.org/10.1093/eurpub/ckp054 [ Links ]
 Correspondence:
Correspondence:
K Hofman
karen.hofman@wits.ac.za
Accepted 1 August 2019


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}