










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSAMJ: South African Medical Journal
versão On-line ISSN 2078-5135
versão impressa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.109 no.2 Pretoria Fev. 2019
http://dx.doi.org/10.7196/samj.2019.v109i2.13347
RESEARCH
A retrospective review on benzodiazepine use: A case study from a chronic dispensary unit
I SinghI; F OosthuizenII
IBPharm, MPharm; Discipline of Pharmaceutical Sciences, School of Health Sciences, University of KwaZulu-Natal, Durban, South Africa
IIBPharm, MSc, PhD; Discipline of Pharmaceutical Sciences, School of Health Sciences, University of KwaZulu-Natal, Durban, South Africa
ABSTRACT
BACKGROUND: Benzodiazepines (BZDs) are highly effective hypnotic and anxiolytic agents and among the most frequently used drugs in the world, but there are significant disadvantages associated with their use. Identifying possible irrational BZD prescribing is important to ensure safe and effective use of these agents. No studies have been conducted in other African countries, and this is the only study in the Western Cape (WC) Province of South Africa (SA), highlighting the paucity of local research
OBJECTIVES: To identify the most commonly prescribed BZDs at a chronic dispensary unit (CDU) in the WC and describe the indications, co-prescribing patterns and patient factors in different areas of the WC
METHODS: A retrospective, quantitative study was carried out using prescription data from a CDU in the Western Cape Department of Health, SA. Data for January 2017 were analysed. Associations between BZD therapeutic indications and co-prescribing patterns were assessed, together with demographic data. Data were coded and descriptive and inferential analysis was done using Stata version 14
RESULTS: A total of 1 396 prescriptions met the inclusion criteria and were analysed. Overall, clonazepam was the most frequently prescribed BZD (n=691 prescriptions, 49.5%), followed by diazepam (n=298, 21.4%), lorazepam (n=222, 15.9%) and oxazepam (n=185, 13.3%). The most common therapeutic indication for BZDs was epilepsy (n=294, 21.1%), followed by depression (n=166, 11.9%) and depression with concomitant anxiety (n=79, 5.7%). The most common concomitant drug class associated with BZD use was antiepileptics (n=1 581), followed by other BZDs (n=706) and analgesics and antipyretics (n=665). Female patients were more likely than males to be prescribed BZDs (p<0.001), and the mean (standard deviation) age of BZD users was 51.3 (19.5) years
CONCLUSIONS: BZDs were most commonly prescribed to female patients and middle-aged adults. Clonazepam was the most frequently prescribed BZD, indicating a preference for long-acting BZDs. Epilepsy was the most common therapeutic indication and antiepileptics were the most common concomitant drug class prescribed, implying that BZDs have a primary role in the management of epileptic conditions in the public healthcare sector. Future studies should include the private sector, as regulations in the public sector greatly influence the patterns of BZD use
Benzodiazepines (BZDs) are a class of psychotropic drugs that function as positive allosteric modulators on the gamma-aminobutyric acid-A (GABAA) receptors in the brain.[1] Binding results in the opening of chloride ion channels, resulting in the neuron becoming negatively charged and resistant to excitation.[1] This process potentiates the inhibitory actions of GABA, resulting in a range of clinical effects including hypnosis, anxiolysis, and anticonvulsant, myorelaxation and amnesic actions.[2] These varying actions have contributed to the widespread use of BZDs.[2] BZDs are most commonly used in the field of psychiatry, but are also frequently prescribed in epilepsy and conditions associated with muscle spasticity.[2] These drugs remain popular because they are highly efficacious and fast acting with minimal toxicity, and it is not surprising that they are among the most frequently prescribed medications globally.[2,3]
Although BZDs have many clinical benefits, there are risks and significant disadvantages associated with their use.[2] Adverse effects of BZDs include psychomotor retardation, memory impairment, paradoxical excitement, emotional blunting and depression.[2,4] The main dangers associated with BZD prescription are the risk of abuse and physiological and psychological dependence.[2] Tolerance may develop with repeated administration and result in dose escalation to reach the previous clinical effect.[2] Additionally, abrupt discontinuation of BZD use can result in a withdrawal syndrome characterised by sleep disturbances, anxiety and irritability.[2] Groups at risk include individuals with a history of substance abuse and the elderly.[4] Individuals with substance abuse may abuse BZDs in combination with other substances that enhance their toxic effects and can result in death.[4] Elderly people have decreased drug metabolism and increased susceptibility to psychomotor and cognitive impairment, which can lead to falls and fractures.[2] The above facts raise concern regarding the safe use of BZDs, so clear guidelines are recommended for their appropriate prescribing.[5] Internationally, many countries have released guidelines on BZD prescribing. In South Africa (SA) the standard treatment guidelines (STGs) and Western Cape (WC) Provincial Code List recommend short-term and limited use.[6,7]
There has been an increase in research on BZD utilisation in most countries, with most information coming from developed countries. A study in the USA found that BZD prescriptions increased by 67% from 1996 to 2013.[8] Another US study found that long-term use of BZDs increased with age from 14.7% in patients aged 18 - 35 years to 31.4% in those aged 65 - 80 years.[9] There are very limited studies on BZD use in developing countries, but the existing research is consistent with international data indicating increased use. No studies have been conducted in other African countries, and there are only a few studies on BZD use in SA. The most noteworthy study on the prescribing patterns of BZDs demonstrated an increase in prescription claims from 7.3% to 8.0% in two provinces, namely the Northern Cape and Gauteng.[10] Two studies in the WC have important implications for this study. The first of these found that BZDs were the substances most misused by patients attending Cape Town specialist treatment centres from 1998 to 2000, which indicates that the WC may be a particularly important setting for BZD utilisation research.[3] The second study found that the WC had the highest prevalence of mental disorders in SA,[11] highlighting the significance of conducting the present study in the WC to determine the associated use of BZDs.
Objectives
There is a need for more studies on BZD use in SA. The main objectives of the present study were to critically assess prescribing patterns of the BZDs most commonly used in the WC and quantify the co-prescribing patterns associated with BZD use, and to provide insight into prescribing and a platform for remedial action for safer and more effective use of medicines.[5] The latter could help control drug expenditure and promote more rational prescribing patterns.
Methods
Study sample
This was a descriptive, retrospective quantitative study of prescription data from the Western Cape Department of Health (WCDoH). The data were obtained from DSV Healthcare, which is a private distributor of pharmaceutical and healthcare products. This company functions as a dispensary and prepackages patient-ready parcels for chronic, stable patients accessing WCDoH facilities. DSV Healthcare has been contracted by the WCDoH to supply medicines to public health patients.
Only prescriptions received during the month of January 2017 were included in the study. A total of 331 507 scripts were received by DSV Healthcare during this time period. Prescriptions were analysed according to BZD use. Four BZDs were reviewed: clonazepam, diazepam, lorazepam and oxazepam. These are the only BZDs stocked at DSV Healthcare and can be dispensed outside a hospital setting.
The inclusion criteria encompassed prescriptions: (i) received by the CDU; (ii) that contained at least one BZD item; and (iii) dated during January 2017. We excluded prescriptions: (i) that did not contain a BZD; (ii) for patients not accessing WCDoH facilities; (iii) for patients accessing City of Cape Town Health facilities, which are not funded by the National Department of Health; (iv) dated outside January 2017; (v) with stat doses, which are not accepted at DSV Healthcare; and (vi) for inpatients, as inpatient prescriptions are not accepted at DSV Healthcare.
Of the 1 396 prescriptions selected for inclusion, two had missing information on patient gender. These were nevertheless included in the study, as all the other variables were recorded.
Full ethical approval was obtained from the University of KwaZulu-Natal (ref. no. BE246/17) and the WCDoH (ref. no. WC_2016RP40_745), and permission to use data was granted by DSV Healthcare.
Sampling, data collection and analysis
The data set was obtained electronically from DSV Healthcare, which stores the WCDoH prescriptions. The data set contained prescription information in the form of an Excel version 16.19 spreadsheet (Microsoft, USA) called a 'data dump'. The indication for BZDs was added manually to the data set according to the International Classification of Diseases and Related Health Problems, 10th revision (ICD-10).
The completed spreadsheet included BZD type, therapeutic indications, patient factors including age and gender, concomitant drugs prescribed with BZDs, and demographics including district and substructure under each region in the WC. These data were coded and analysed using Stata version 14 (StataCorp, USA).
Results were described using frequencies, percentages and means (with standard deviations (SDs)). The 25th, 50th and 75th percentiles for age were also used. Pearson's χ2 test was used to assess associations between categorical variables, and analysis of variance to compare differences in age between BZD users. A p-value <0.05 was considered to be statistically significant. Data were analysed using Stata version 14.
In addition, concomitant medication use associated with BZD prescribing was identified by grouping medications into drug classes and identifying the most frequent concomitant drug classes prescribed.
Results
Prescribing patterns per district
A total of nine substructures were analysed, each belonging to either the metropolitan district or the rural district. The metropolitan district constituted four substructures: Eastern Khayelitsha, Northern Tygerberg, South Western and Klipfontein/Mitchell's Plain. The rural district constituted five substructures: Cape Winelands, Central Karoo, Eden, Overberg and West Coast.
Of the 1 396 prescriptions analysed, the majority were from the metropolitan district (n= 969, 69.4%) as opposed to the rural district (n=427, 30.6%). The prescribing frequency for BZDs per district is presented in Table 1.
Overall, clonazepam was the most frequently prescribed BZD (n=691, 49.5%), accounting for approximately half of the total number of BZD prescriptions. Diazepam was the second most frequently prescribed (n=298, 21.4%) followed by lorazepam (n=222, 15.9%) and oxazepam (n=185, 13.3%). Clonazepam was the most frequently prescribed BZD in both the metropolitan and rural districts (metropolitan 45.0% and rural 59.7%).
Oxazepam was the BZD with the lowest prescribing frequency in the metropolitan district (11.0%), while lorazepam was the BZD with the lowest prescribing frequency in the rural district (8.2%).
Prescribing patterns per substructure
Benzodiazepine prescribing frequency in the different substructures is presented in Table 2. Northern Tygerberg had the highest number of BZD prescriptions (n=400, 28.7%) while Central Karoo had the lowest (n=19, 1.4%).
Overall, clonazepam was the most frequently prescribed BZD among the substructures, with the exception of Klipfontein/Mitchell's Plain, where diazepam was prescribed more frequently (n=54, 38.0%) than clonazepam (n=51, 35.9%). The least prescribed BZD differed for each substructure, with oxazepam having the lowest prescribing frequency in five out of the nine substructures.
Analysis of benzodiazepine prescribing related to patient demographics
Prescribing patterns associated with gender (Table 3)
There were statistically more females (n=793 prescriptions, 56.9%) receiving BZDs than males (n=601, 43.1%) (p<0.001). Clonazepam was the most frequently prescribed BZD for both females (n=412, 52.0%) and males (n=278, 46.3%).
The least prescribed BZD differed according to gender. Diazepam was the least prescribed BZD in females (n=118, 14.9%), while oxazepam was the least prescribed in males (n=51, 8.4%).
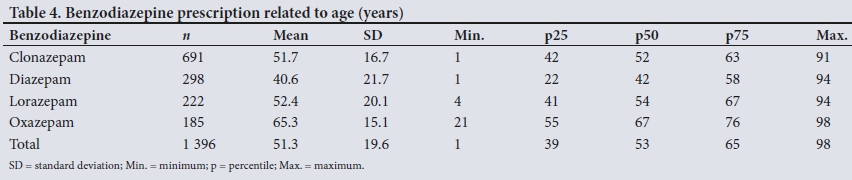
Prescribing patterns associated with age (Table 4)
The ages of patients receiving prescriptions for BZDs ranged from 1 to 98 years, with a mean (SD) of 51.3 (19.6). The mean (SD) ages of patients receiving clonazepam and lorazepam were 51.7 (16.7) years and 52.4 (20.1) years, respectively.
Diazepam tended to be prescribed to younger patients (mean (SD) 40.57 (21.7) years) and oxazepam to older patients (65.3 (15.1) years). Age differed significantly between users of the different BZDs (p<0.0001), with the exception of clonazepam and lorazepam. The 25th, 50th and 75th percentiles were 39, 53 and 65 years, indicating that in the main the ages of the population of BZD users ranged from middle adulthood to elderly (34 - 60 years).
Prescribing patterns associated with benzodiazepine indication
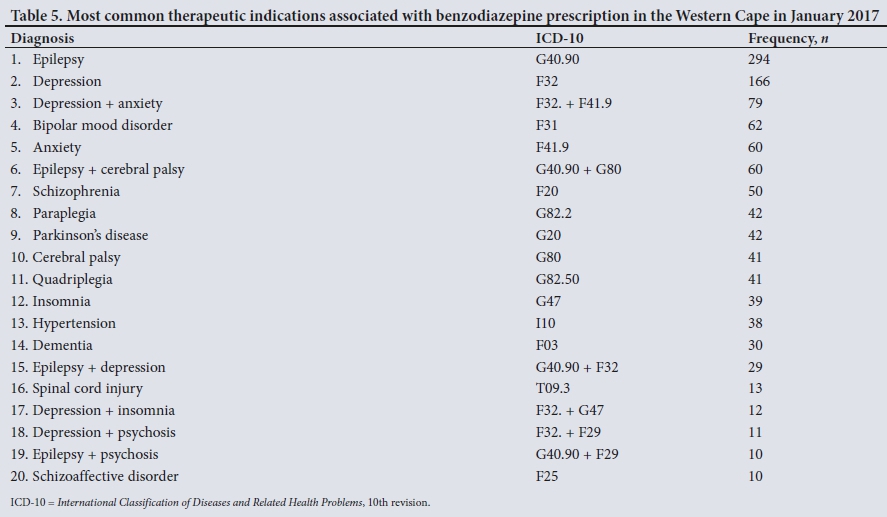
The indications most frequently listed for BZD use in the WC are reported in Table 5. The most common therapeutic indication was epilepsy (n=294 prescriptions, 21.1%) followed by depression (n=166, 11.9%) and depression with concomitant anxiety (n=79, 5.7%).
Concomitant medication prescribing
The data were analysed to identify concomitant medications associated with BZD use (Table 6). This analysis was done by grouping drug classes together.

A total of 9 026 concomitant drugs were found in the 1 396 prescriptions included in this study. The most common concomitant drug class prescribed was antiepileptics (n=1 581 prescriptions), followed by other BZDs (n=706) and analgesics and antipyretics (n=665). Other significant co-prescribed drug classes included selective serotonin reuptake inhibitors (n=379) and tricyclic anti-depressants (n=220).
Discussion
Multiple studies on BZD use have been done in developed countries, but there has been little similar research in SA. This is the first study to report BZD prescribing patterns in the WC public healthcare setting.
The study reviewed 1 396 BZD prescriptions for the month of January 2017 in the WC. The majority were from the metropolitan district, which has a larger populations than the rural district, resulting in more people accessing public healthcare facilities and an increased likelihood of being prescribed a BZD.[12]
We found that of the four BZDs reviewed, clonazepam was the most frequently prescribed in both the metropolitan and rural districts, followed by diazepam, lorazepam and oxazepam. Prescription of BZDs is heavily regulated in the WC.[7] According to the Provincial Code List, prescription of a BZD should not exceed 14 days except in the case of specialist referral under certain conditions including epilepsy and cerebral palsy and severe muscle spasms in children. [7]
The high prescription rate for clonazepam is probably due to less strict restrictions for clonazepam that permit its longer-term use in epilepsy[7] and may result in repeat prescriptions and chronic use of this agent.
Additionally, clonazepam is classified as a long-acting BZD. Some prescribers prefer long-acting BZDs due to an increase in dosing intervals, which contribute to its popularity among prescribers and patients.[2] A study from a mental healthcare facility in the USA in patients with depression found long-acting (half-life >24 hours) clonazepam to be the most frequently prescribed BZD.[13] Similarly, a study in Brazil's public healthcare sector assessing dependence and anxiety in BZD users also found clonazepam to be the most widely used BZD.[13,14] There are no studies on BZD utilisation from African countries other than SA. Notably, two of the four studies from SA also demonstrated that long-acting BZDs are most commonly used. [15,16] A 2007 study by Kairuz and Truter[15] in the private sector in SA found that diazepam, a BZD with a half-life similar to clonazepam, was the most frequently prescribed BZD. Earlier, in 1990, Summers et al.[16] demonstrated that the majority of BZDs prescribed in a public hospital in SA fell into the long-acting and intermediate-acting categories, showing that this bias exists across the healthcare sector. The frequent prescribing of clonazepam in our study can therefore probably be ascribed to both a convenient dosing interval and high rates of the chronic conditions that this drug is used for.
In the present study, diazepam was the second most commonly prescribed BZD overall. Like the more often prescribed clonazepam, diazepam also has less strict restrictions in the WC that allow its use in children with cerebral palsy and severe muscle spasms[7] and may be a contributory factor in its high rate of use. In the available literature, short-acting BZDs are prescribed more frequently than their longer-acting counterparts.[9,17] A meta-analysis from a longitudinal prescription database that included ~60% of all retail pharmacies in the USA demonstrated that only one-quarter of individuals receiving BZDs used long-acting agents.[9]
Lorazepam and oxazepam had lower prescription rates overall than the other BZDs, probably because they are recommended for restricted and short-term use in clinical indications that are less prevalent than conditions other BZDs are used for. A study in Pakistan investigating BZD use in outpatient clinics found that alprazolam, a short-acting BZD, was most commonly used in patients with cardiovascular problems.[18] A cross-sectional Lebanese study assessing BZD prescription patterns also found that short-acting BZDs were frequently prescribed.[19] These results highlight the fact that while long-acting BZDs are most commonly prescribed in many countries, short-acting ones are still preferred in others. Short-acting BZDs may be prescribed more frequently because of their usefulness in certain populations. The Beers Criteria, for example, recommend the use of short-acting BZDs rather than longer-acting agents in geriatric patients.[20] The Beers Criteria suggest that short-acting BZDs are safer than long-acting ones in patients aged >65 years because the latter can cause prolonged sedation, increasing the risk of falls and fractures in the elderly.[20]
A study in the USA on BZD use from January 2008 to December 2008 found a general increase in the use of these agents with age, with the highest increase of 8.7% in individuals aged 65 - 80 years.[9] A study in Norway evaluating a prescription database from 2004 to 2009 found that the mean age of BZD users was 62 years, almost 10 years older than the mean age in our study.[21] Patients in older age groups tend to have an increased disease burden, especially with regard to neurocognitive and neuropsychiatric conditions and chronic pain syndrome, which may explain the increased use of BZDs in the elderly.[9] A study in Brazil assessing dependence and anxiety in BZD users found that those with the highest rate of use were between 61 and 70 years of age, again indicating an older age group compared with our study. In the current study, the majority of the patients prescribed BZDs were adults aged 34 - 60 years.[14]
Interestingly, a study in Pakistan reviewing BZD use in outpatient clinics found the average age of BZD users to be 45 years, which is much younger than in our study.[18] Similarly, an SA study in 2004 reviewing BZD prescriptions from private healthcare patients found the mean age to be 43.17 years.[15] Another study conducted in the private healthcare sector of SA in Gauteng and Northern Cape provinces found that patients aged 40 - 65 years had the highest rate of BZD prescriptions.[10] It is important to note that use of BZDs is not recommended in elderly patients, as the half-lives of BZDs are increased in the elderly, leading to toxicity and an increase in the likelihood of falls and fractures.[4] Guidelines such as the Beers Criteria therefore suggest that the elderly should use short-acting agents in the short term only.[20]
The present study found that significantly more females than males were prescribed BZDs. This is consistent with other reports highlighting a higher prevalence of BZD prescriptions in females. [9,13,14] Three of the four studies that reviewed BZD use in SA found it to be higher in females (the fourth study did not analyse gender differences).[10,15-17] Epidemiological data suggest that females tend to have a higher prevalence of depression and anxiety than males, which are common therapeutic indications for BZDs.[2,22] This correlates with our finding that depression and depression and anxiety were the therapeutic conditions most often treated with a regimen that included a BZD. Additionally, studies suggest that females are more inclined to use medication and access health services than males, resulting in a greater likelihood of BZD use.[14]
The most common therapeutic indication for prescription of a BZD in our study was epilepsy (n=294 prescriptions, 21.1%). This finding is not surprising, as the WC approves the use of clonazepam in epilepsy.[7] The STGs indicate that epileptic conditions such as generalised tonic-clonic seizures and partial seizures should be treated with anticonvulsant medications such as carbamazepine, lamotrigine, phenytoin or valproate.[6] However, the STGs recommend that absence seizures and myoclonic seizures should be referred for specialist consultation.[6] A specialist can approve the prescription of clonazepam as adjuvant therapy in absence seizures and myoclonic seizures in this setting. Guidelines from the National Institute for Health and Care Excellence (NICE) indicate that BZDs can be used as alternative agents in the treatment of atypical absence seizures, myoclonic seizures and idiopathic generalised epilepsy, which is in line with the STGs.[23]
The most frequent concomitant drug class prescribed with BZDs was antiepileptic drugs. Benzodiazepines can be used in the management of epileptic conditions, as they act by decreasing the duration and spread of seizures.[24] They are still frequently prescribed as an adjunct to other antiepileptics in the management of epilepsy when monotherapy is ineffective, as they produce pharmacological synergism.[25] Additionally, BZDs have been proven to be valuable in the emergency management of status epilepticus, where they are first-line agents in most management protocols.[2]
The second most common therapeutic indication for BZD prescribing was depression. Studies in the USA have found depression to be the most common therapeutic indication for BZD prescription upon discharge,[13,221 while in developing countries such as Thailand and Lebanon depression has been identified as the third most common therapeutic indication.[19,261 These findings demonstrate the worldwide prevalence of BZD use in depression.
The third most common therapeutic indication for BZD prescribing was depression with concomitant anxiety. Anxiety and depression are very common comorbid disease states that present with similar symptoms[27] and are therefore grouped together. A study in the USA on BZD use in older patients in a primary care setting found that anxiety was a common indication for BZD use.[28] Additionally, studies in Thailand and Lebanon have identified anxiety as the main indication for BZD prescription, which indicates that these comorbid states are commonly treated with BZDs.[19,26] The high prevalence of anxiety as a therapeutic indication combined with a high prevalence of depression means that BZDs are commonly used in these comorbid states.
The second most frequent concomitant drug class prescribed with a BZD was a second BZD. There is no therapeutic basis for the use of more than one BZD in the same patient, because BZDs all have the same mechanism of therapeutic action, differing only with regard to pharmacokinetic properties.[29] A study on co-prescription of BZDs in Norway found the practice of using more than one BZD concomitantly to be widespread, and often initiated by the same prescriber.[29]
Study limitations
This study was restricted to prescriptions sent to a WCDoH CDU, so there is no way of knowing the true number of patients prescribed BZDs in the WC, as some pharmacies may choose to manage patients at facility level. Prescriptions from City of Cape Town facilities were excluded, and this study on BZD prescription in the WC therefore has incomplete data.
This study only reviewed prescriptions in the public healthcare sector, which is highly regulated in terms of the Essential Drugs List (EDL). The EDL provides a subset of drugs available for prescription that is limited to specialist doctors. This provides a unique platform for drug use patterns that cannot be transposed onto the private healthcare sector, which has a wider variety of drugs and spectrum of use. Additionally, any clinician can prescribe BZDs, which creates further disparity between research conducted in the private and public healthcare sectors.
The fact that only prescriptions dispensed in the month of January 2017 were reviewed also means that information on BZD prescription patterns is limited.
Conclusions
The present study confirmed the findings of other researchers that female patients and patients in older age groups are most likely to be prescribed BZDs. We found clonazepam to be the most frequently prescribed BZD, which is in keeping with other studies showing a preference for long-acting BZDs.
The study found the use of BZDs to be rational, taking into account the therapeutic indications and types of BZDs prescribed, as well as the use of concomitant drug therapy.
Future research reviewing BZD use should include the private healthcare sector, to provide greater insight and create greater generalisability on BZD prescribing patterns. Additionally, using a longer time frame and including City of Cape Town prescriptions would give a fuller understanding of BZD prescription patterns in the WC.
Declaration. This publication forms part of the work emanating from IS's Master of Pharmacy degree.
Acknowledgements. We thank MsYusentha Balakrishna for her valuable statistical input.
Author contributions. IS: conceptualisation, data analysis, drafting of manuscript; FO: conceptualisation, contribution to writing of manuscript, review of manuscript.
Conflicts of interest. None.
References
1. Griffin CE III, Kaye AM, Bueno FR, Kaye AD. Benzodiazepine pharmacology and central nervous system-mediated effects. Ochsner J 2013;13(2):214-223. [ Links ]
2. Ashton H. The diagnosis and management of benzodiazepine dependence. Curr Opin Psychiatry 2005;18(3):249-255. https://doi.org/10.1097/01.yco.0000165594.60434.84 [ Links ]
3. Myers B, Siegfried N, Parry CD. Over-the-counter and prescription medicine misuse in Cape Town -findings from specialist treatment centres. S Afr Med J 2003;93(5):367-370. [ Links ]
4. Longo LP, Johnson B. Addiction: Part I. Benzodiazepines - side effects, abuse risk and alternatives. Am Fam Physician 2000;61(7):2121-2128. [ Links ]
5. Academy of Managed Care Pharmacy. Drug Utilization Review. 2009. http://www.amcp.org/WorkArea/DownloadAsset.aspx?id=9296 (accessed 20 December 2018). [ Links ]
6. National Department of Health, South Africa. Essential Drugs Programme. Primary Healthcare Standard Treatment Guidelines and Essential Medicines List. 5th ed. Pretoria: NDoH, 2014:16.9-16.10. [ Links ]
7. Western Cape Department of Health. Provincial Code List: Catalogue of approved pharmaceuticals for use in the Department of Health. 2017. https://www.westerncape.gov.za/assets/departments/health/pharmacy_code_list_june_2013.pdf (accessed 20 December 2017). [ Links ]
8. Bachhuber MA, Hennessy S, Cunningham CO, Starrels JL. Increasing benzodiazepine prescriptions and overdose mortality in the United States, 1996 - 2013. Am J Public Health 2016;106(4):686-688. https://doi.org/10.2105/AJPH.2016.303061 [ Links ]
9. Olfson M, King M, Schoenbaum M. Benzodiazepine use in the United States. JAMA Psychiatry 2015;72(2):136-142. https://doi.org/10.1001/jamapsychiatry.2014.1763 [ Links ]
10. Visser CD. Prescribing patterns of benzodiazepines: A comparative study between two provinces in South Africa. MPharm (Pharmacy Practice) thesis. Potchefstroom: North-West University, 2011. [ Links ]
11. Herman AA, Stein DJ, Seedat S, Heeringa SG, Moomal H, Williams DR. The South African Stress and Health (SASH) study: 12-month and lifetime prevalence of common mental disorders. S Afr Med J 2009;99(5):339-344. [ Links ]
12. Statistics South Africa. Mid-year population estimates 2016. Statistical release P0302. Pretoria: Stats SA, 2017. https://www.statssa.gov.za/publications/P0302/P03022016.pdf (accessed 20 December 2018). [ Links ]
13. Valenstein M, Taylor KK, Austin K, Kales HC, McCarthy JF, Blow FC. Benzodiazepine use among depressed patients treated in mental health settings. Am J Psychiatry 2004;161(4):654-661. https://doi.org/10.1176/appi.ajp.161.4.654 [ Links ]
14. Schallemberger JB, Colet CD. Assessment of dependence and anxiety among benzodiazepine users in a provincial municipality in Rio Grande do Sul, Brazil. Trends Psychiatry Psychother 2016;38(2):63-70. https://doi.org/10.1590/2237-6089-2015-0041 [ Links ]
15. Kairuz TE, Truter I. A descriptive study of anxiolytic and hypnotic prescribing according to age and sex. Int J Pharmacy Pract 2007;15(4):301-306. https://doi.org/10.1211/ijpp.15.4.0008 [ Links ]
16. Summers RS, Schutte AD, Summers BE. Benzodiazepine use in a small community hospital: Appropriate prescribing or not? S Afr Med J 1990;78(12):721-725. [ Links ]
17. Kairuz T, Truter I, Rossato L, Pudmenzky A. Dispensing patterns of anxiolytics and sedative-hypnotics: A feasibility study comparing datasets from a developed and a developing country (Australia and South Africa). Curr Drug Saf 2017;12(1):57-61. https://doi.org/10.2174/1574886312666170109115741 [ Links ]
18. Patel MJ, Ahmer S, Khan F, Qureshi AW, Shehzad MF, Muzaffar S. Benzodiazepine use in medical outpatient clinics: A study from a developing country. J Pak Med Assoc 2013;63(6):717-720. https://www.ncbi.nlm.nih.gov/pubmed/23901671 [ Links ]
19. Ramadan WH, El Khoury GM, Deeb ME, Sheikh-Taha M. Prescription patterns of benzodiazepines in the Lebanese adult population: A cross-sectional study. Neuropsychiatr Dis Treat 2016;6(12):2299-2305. https://doi.org/10.2147/NDT.S113078 [ Links ]
20. Fick DM, Cooper JW, Wade WE, Waller JL, Maclean JR, Beers MH. Updating the Beers criteria for potentially inappropriate medication use in older adults: Results of a US consensus panel of experts. Arch Intern Med 2003;163(22):2716-2724. https://doi.org/10.1001/archinte.163.22.2716 [ Links ]
21. Bramness JG, Sexton JA. The basic pharmacoepidemiology of benzodiazepine use in Norway 2004-9. Nor Epidemiol 2011;21(1):35-41. https://doi.org/10.5324/nje.v21i1.1423 [ Links ]
22. Peters SM, Knauf KQ, Derbidge CM, Kimmel R, Vannoy S. Demographic and clinical factors associated with benzodiazepine prescription at discharge from psychiatric inpatient treatment. Gen Hosp Psychiatry 2015;37(6):595-600. https://doi.org/10.1016/j.genhosppsych.2015.06.004 [ Links ]
23. Appleton RE, Freeman A, Cross JH. Diagnosis and management of the epilepsies in children: A summary of the partial update of the 2012 NICE epilepsy guideline. Arch Dis Child 2012;97(12):1073-1076. https://doi.org/10.1136/archdischild-2012-302822 [ Links ]
24. Henriksen O. An overview of benzodiazepines in seizure management. Epilepsia 1998;39(1):2-6. http://onlinelibrary.wiley.com/doi/10.1111/j.1528-1157.1998.tb05110.x/pdf (accessed 20 December 2018). [ Links ]
25. George J, Jose J, Kulkarni DA, Hanamantappa RR, Shalavadi CV. Evaluation of drug utilization and analysis of anti-epileptic drugs at tertiary care teaching hospital. Indian J Pharmacy Pract 2016;9(3):189-194. https://doi.org/10.5530/ijopp.9.3.10 [ Links ]
26. Srisurapanont M, Garner P, Critchley J, Wongpakaran N. Benzodiazepine prescribing behaviour and attitudes: A survey among general practitioners practicing in northern Thailand. BMC Fam Pract 2005;6(1):27. https://doi.org/10.1186/1471-2296-6-27 [ Links ]
27. Dunlop BW, Davis PG. Combination treatment with benzodiazepines and SSRIs for comorbid anxiety and depression: A review. Prim Care Companion J Clin Psychiatry 2008;10(3):222-228. [ Links ]
28. Simon GE, Ludman EJ. Outcome of new benzodiazepine prescriptions to older adults in primary care. General Hosp Psychiatry 2006;28(5):374-378. https://doi.org/10.1016/j.genhosppsych.2006.05.008 [ Links ]
29. Handal M, Skurtveit S, M0rland JG. Co-medication with benzodiazepines. Tidsskr Nor Laegeforen 2012;132(5):526-530. https://doi.org/10.4045/tidsskr.11.0321 [ Links ]
 Correspondence:
Correspondence:
F Oosthuizen
oosthuizenf@ukzn.ac.za
Accepted 16 July 2018


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}