










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.109 n.1 Pretoria Jan. 2019
http://dx.doi.org/10.7196/samj.2019.v109i1.13696
CORRESPONDENCE
Genomic characterisation of Klebsiella michiganensis co-producing OXA-181 and NDM-1 carbapenemases isolated from a cancer patient in uMgungundlovu District, KwaZulu-Natal Province, South Africa
To the Editor: The emergence and spread of carbapenem-resistant Enterobacteriaceae (CRE) is a serious public health concern worldwide, especially for hospitalised patients.[1-3] Klebsiella spp. are recognised as significant pathogens responsible for serious difficult-to-treat nosocomial infections.[1,4] Several reports have identified Klebsiella spp. co-producing New Delhi metallo-beta-lactamase (NDM) and other carbapenemases worldwide.[1,4-7] Although NDM-1-producing K. michiganensis was reported in clinical samples from the private sector in KwaZulu-Natal Province, South Africa (SA),[8] this is the first detection of blaNDM-1 and blaOXA-181in a carriage isolate of K. michiganensis A202R3B6 (accession no. QKWV00000000). A 59-year-old cancer patient was screened at admission and discharge in a surgical ward in a district hospital in SA. The patient received cloxacillin 250 mg twice daily for 5 days until discharge. Faecal culture was negative at admission but revealed carriage of carbapenemase-producing K. michiganensis ST 29 (A202R3B6) at discharge.
This isolate was initially identified as K. oxytoca, but genomic identification confirmed it to be K. michiganensis. K. michiganensis formed part of a bigger study investigating antibiotic-resistant bacteria in clinical and carriage samples from patients admitted to a district and tertiary hospital in uMgungundlovu District, KwaZulu-Natal, SA. The isolate was identified using biochemical tests (Rosco Diagnostica, Denmark). Antimicrobial susceptibility testing was performed by broth microdilution, and results were interpreted according to the European Committee on Antimicrobial Susceptibility Testing (EUCAST). Escherichia coli ATCC 25922, K. pneumoniae ATCC 700603 and K. pneumoniae ATCC 51503 were used as controls.
Whole-genome sequencing (WGS) analysis was performed on a MiSeq platform (Illumina, USA) with 100x coverage. The bacterial analysis pipeline of GoSeqIt tools was used to annotate and identify known acquired antibiotic-resistant genes via ResFinder,[9] virulence factors using VirulenceFinder[10] and mobile genetic elements through PlasmidFinder.[11] The multi-locus sequence type was determined from WGS data.
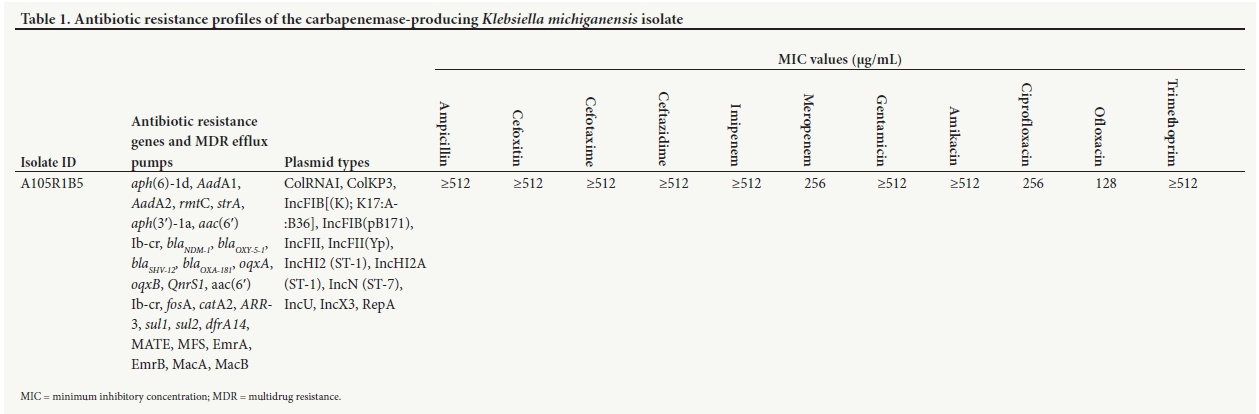
The final assembly of K. michiganensis ST 29 A202R3B6 contained 6 499 557 base pairs with 60.87% G+C content. Analysis of WGS data revealed that the K. michiganensis harboured several antibiotic resistance genes and multidrug resistance efflux pumps (Table 1). PlasmidFinder revealed that the genome of K. michiganenesis ST 29 (A202R3B6) harboured 12 plasmids, and genomic analysis revealed that the IncX3 plasmid harboured blaNDM-1 (Table 1).
To the best of our knowledge, the detection of these carbapenemases along with several resistance genes in a carriage sample is the first reported from SA and suggests that the intestinal tract serves as reservoir of resistant bacteria. blaOXA-181and blaNDM-1 are commonly detected in E. coli and K. pneumoniae worldwide,[4,7] and as such, the concomitant presence of these carbapenemase genes in K. michiganensis ST 29 suggests that horizontal gene transfer occurs within and between bacterial species. In addition, this isolate was not detected on screening at admission but only at discharge, suggesting a lack of infection prevention and control (IPC) measures at the hospital. Our findings therefore underline the importance of routine screening for extended-spectrum beta-lactamases and/or carbapenemase bacteria upon admission and the need for IPC to be strictly implemented to reduce the dissemination of CRE in SA.
Author contributions. RCF co-conceptualised the study, undertook sample collection and microbiological laboratory and data analyses, prepared tables, interpreted results, contributed to bioinformatics analysis, and drafted the manuscript. LLF undertook sample collection and microbiological laboratory analyses, contributed to bioinformatics analysis and vetted the results. MA undertook bioinformatics analysis. AI performed whole-genome sequencing analysis. SYE co-conceptualised the study and undertook critical revision of the manuscript. All authors read and approved the final manuscript.
Funding. This work was supported by the Antimicrobial Research Unit and College of Health Sciences of the University of KwaZulu-Natal. The National Research Foundation (NRF) funded this study through the NRF Incentive Funding for Rated Researchers (grant no. 85595), the NRF Competitive Grant for Rated Researchers (grant no. 106063) and the DST/NRF South African Research Chair in Antibiotic Resistance and One Health (grant no. 98342) awarded to SYE. The South African Medical Research Council also funded the WGS aspect of study through the Self-Initiated Research Grant. Any opinions, findings and conclusions or recommendations expressed in this letter are those of the authors and do not necessarily reflect the views of the organisations or agencies that provided support for the project. The funders had no role in the study design or the decision to submit the work for publication.
Conflicts of interest. SYE is a member of the Global Respiratory Infection Partnership sponsored by an unrestricted educational grant from Reckitt Benckiser, UK.
Raspail Carrel Founou
Antimicrobial Research Unit, College of Health Sciences, University of KwaZulu-Natal, Durban, South Africa; and Department of Clinical Microbiology, Centre of Expertise and Biological Diagnostic of Cameroon, Yaoundé, Cameroon. czangue@yahoo.fr
Luria Leslie Founou
Antimicrobial Research Unit, College of Health Sciences, University of KwaZulu-Natal, Durban, South Africa; and Department of Food Safety and Environmental Microbiology, Centre of Expertise and Biological Diagnostic of Cameroon, Yaoundé, Cameroon
Mushal Allam, Arshad Ismail
Sequencing Core Facility, National Health Laboratory Service, Johannesburg, South Africa
Sabiha Yusuf Essack
Antimicrobial Research Unit, College of Health Sciences, University of KwaZulu-Natal, Durban, South Africa
References
1. Liapis E, Pantel A, Robert J, Nicolas-Chanoine M, Cavalié L, Mee-Marquet O. Molecular epidemiology of OXA-48-producing Klebsiella pneumoniae in France. Clin Microbiol Infect 2014;20(12):O1121-O1123 https://doi.org/10.1111/1469-0691.12727 [ Links ]
2. Mediavilla JR, Patrawalla A, Chen L, et al. Colistin- and carbapenem-resistant Escherichia coliharboring mcr-1 and blaNDM-5, causing a complicated urinary tract infection in a patient from the United States. MBio 2016;7(4):e01191-16. https://doi.org/10.1128/mBio.01191-16 [ Links ]
3. Tokajian S, Eisen JA, Jospin G, Farra A, Coil DA. Whole genome sequencing of extended-spectrum ß-lactamase producing Klebsiella pneumoniae isolated from a patient in Lebanon. Front Cell Infect Microbiol 2015;8 April. https://doi.org/10.3389/fcimb.2015.00032 [ Links ]
4. Dortet L, Poirel L, Yaqoubi FA, Nordmann P. NDM-1, OXA-48 and OXA-181 carbapenemase-producing Enterobacteriaceae in Sultanate of Oman. Clin Microbiol Infect 2012;18(5):E144-E148. https://doi.org/10.1111/j.1469-0691.2012.03796.x [ Links ]
5. Founou L, Founou R, Essack S. Antibiotic resistance in the food chain: A developing country-perspective. Front Microbiol 2016; 7:1881. https://doi.org/10.3389/fmicb.2016.01881 [ Links ]
6. Iwase T, Ogura Y, Hayashi T, Mizunoe Y. Complete genome sequence of Klebsiella oxytoca strain JKo3. Genome Announc 2016;4(6):e01221-16. https://doi.org/10.1128/genomeA.01221-16 [ Links ]
7. Mei YF, Liu PP, Wan LG, Liu Y, Wang LH, Wei D. Virulence and genomic feature of a virulent Klebsiella pneumoniae sequence type 14 strain of serotype K2 harboring blaNDM-5 in China. Front Microbiol 2017;8(335). https://doi.org/10.3389/fmicb.2017.00335 [ Links ]
8. Pedersen T, Sekyere JO, Govinder U, et al. Spread of plasmid-encoded NDM-1 and GES-5 carbapenemases among extensively drug-resistant and pandrug-resistant clinical enterobacteriaceae in Durban, South Africa. Antimicrob Agents Chemother 2018;62(5):e02178-17. https://doi.org/10.1128/AAC.02178-17 [ Links ]
9. Zankari E, Hasman H, Cosentino S, et al. Identification of acquired antimicrobial resistance genes. J Antimicrob Chemother 2012;67(11):2640-2644. https://doi.org/10.1093/jac/dks261 [ Links ]
10. Joensen KG, Scheutz F, Lund O, et al. Real-time whole-genome sequencing for routine typing, surveillance, and outbreak detection ofverotoxigenic Escherichia coli. J Clin Microbiol 2014;52(5):1501-1510. https://doi.org/10.1128/JCM.03617-13 [ Links ]
11. Carattoli A, Zankari E, García-Fernández A, et al. In silico detection and typing of plasmids using PlasmidFinder and plasmid multilocus sequence typing. Antimicrob Agents Chemother 2014;58(7):3895-3903. https://doi.org/10.1128/AAC.02412-14 [ Links ]


{kind=link}