










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.108 n.12 Pretoria Dec. 2018
http://dx.doi.org/10.7196/samj.2018.v108i12.13134
RESEARCH
Another piece to the epidemiological puzzle of traumatic spinal cord injury in Cape Town, South Africa: A population-based study
J PhillipsI; J BraafII; C JosephIII, IV
IPhD; Department of Physiotherapy, Faculty of Community and Health Sciences, University of the Western Cape, Cape Town, South Africa
IIBSc; Yad-Marpe Physiotherapy Practice, Cape Town, South Africa
IIIPhD; Department of Physiotherapy, Faculty of Community and Health Sciences, University of the Western Cape, Cape Town, South Africa
IVPhD; Division of Physiotherapy, Department of Neurobiology, Care Sciences and Society, Karolinksa Institutet, Flemingsberg, Sweden
ABSTRACT
BACKGROUND. The epidemiology of traumatic spinal cord injury (TSCI) is poorly understood in developing countries. In South Africa (SA) specifically, two healthcare systems (private v. government funded) exist, and it is therefore important to assess patient characteristics in order to plan appropriately.
OBJECTIVES. To determine epidemiological characteristics of TSCI in the private healthcare system in Cape Town, SA, and compare findings with previously published data from the government sector.
METHODS. A regional, population-based design was used, including all private and government-funded hospitals in the catchment area (Cape Town Metropolitan Municipality). All eligible survivors of TSCI in the private sector were retrospectively identified from admission records for a 1-year period. The International Spinal Cord Injury Core Data Set was systematically completed using patient medical records. Epidemiological data from the government cohort were secondarily analysed; however, socioeconomic variables were primarily analysed in this study. Inferential statistics were used to assess differences between the two healthcare systems.
RESULTS. The annual crude incidence of 20.0 per million in the private sector was significantly lower than the 75.6 per million in the government sector (p<0.001). In addition, the two cohorts differed significantly with regard to age at injury, pre-injury employment and aetiology, highlighting that individuals in the private sector were older than those in the government sector, that most were employed prior to the injury, and that their injuries were chiefly transport related, as opposed to assault in the government sector.
CONCLUSIONS. Two cohorts with TSCI from the sampling population differed with regard to incidence, aetiology and sociodemographic characteristics. The findings suggest the need for more than one high-priority primary prevention programme, stratified by healthcare system. These programmes should inclusively emphasise road safety and the consequences of interpersonal violence among men.
Traumatic spinal cord injury (TSCI) is one of the most devastating conditions known to humanity. Depending on the level and completeness of the injury, it causes considerable morbidity as a result of changes in sensory, motor and autonomic functions.[1,2] The morbidity associated with a TSCI affects more than just the individual, exerting demands on the family (often responsible for providing assistance to survivors) and the healthcare system.[3-5]
Within the global scientific community, prevention of TSCI and its negative consequences has become a central part of the agenda, and a global project aiming to inform stakeholders of the development and co-ordination of prevention strategies has been initiated and implemented.[6] The first step of this mapping project was to provide knowledge pertaining to the epidemiology of spinal cord injuries (both traumatic and non-traumatic). However, considerable knowledge gaps have been identified, especially in the developing world (Asia, Africa, the Caribbean, etc.).[6-8]
A recent epidemiological study on TSCI in Cape Town, South Africa (SA), revealed a high incidence rate of 75.6 per million among the population utilising government-funded healthcare. The study also reported interpersonal violence to be the main cause of injury.[9] However, it remained unclear whether the results pertaining to the incidence, aetiology and injury characteristics could be applied to survivors of TSCI with private healthcare insurance in the same catchment area. Furthermore, little is known about the socioeconomic profile of survivors of TSCI with private insurance in respect of its influence on incidence rate and aetiology.
Objectives
Given these knowledge gaps, the objectives of this study were to: (i) determine the incidence, aetiology and injury characteristics of TSCI in individuals with private healthcare insurance in Cape Town, SA, compared with previously published data on those with government-funded healthcare; and (ii) compare the socioeconomic standing of individuals with private insurance v. those with government-funded healthcare.
Methods
Research design and setting
This population-based cohort design identified patients with TSCI admitted to acute/rehabilitation privately funded hospitals in Cape Town, SA, from 15 September 2013 to 14 September 2014. The dates of (retrospective) registration of TSCI cases coincided with the study period of the prospective data collection in the government-funded cohort, thus aiding comparison.
The Cape Town population was estimated at 3.86 million (mid-2014), of whom 25% were covered by private healthcare insurance.[10] This study context is very diverse in terms of ethnicity and socioeconomic class/status. A 2014 public provincial document reported that 49.7% of the population of employable age (15 - 64 years) was employed. The care provision for persons with TSCI in the private healthcare context is not centralised; survivors are typically managed at a range of acute-care hospitals, but initial acute rehabilitation is mainly offered at one private centre. Heads of neurology and orthopaedic departments were contacted to ascertain admittance of individuals with TSCI during the data collection period. Three private hospitals admitted such patients, with most recruited from a private academic hospital that also provides inpatient rehabilitation.
Data collection and procedure
Three private hospitals managed patients with TSCI during the data collection period. Other than that survivors had to be admitted to a private facility, the inclusion criteria were similar to the previous study:[9] (i) confirmed acute traumatic spinal cord or cauda equina lesion; (ii) age >18 years at the time of injury; (iii) admittance to a private acute-care hospital; (iv) survival for at least 7 days post trauma and maintaining TSCI as the primary diagnosis; and (v) survivors who were resident in the country and the catchment region.
The International Spinal Cord Injury Core Data Set was used to collect data to determine the incidence, aetiology, extent of the injury (vertebral injuries, associated injury, need for spinal surgery and ventilatory support, and neurological classification) and length of hospital stay.[11,12] Diagnosis of TSCI was based on evaluation of the magnetic resonance imaging results, and neurological severity was assessed by specialist neurologists according to the International Standards for Neurological Classification of Spinal Cord Injury.[13]
One of the authors (JB) reviewed medical records of patients meeting the criteria for inclusion and systematically completed the International Core Data Set for Spinal Cord Injury. Ethical approval for research conducted in the government setting was granted by the Research Ethics Committee of the University of the Western Cape (ref. no. BM/13/4/27) and permission was granted by the heads of departments of the respective private hospitals. All ethical principles pertaining to research conducted on human volunteers were adhered to.
Secondary analysis of the government-funded healthcare sector
This study used selected data variables from an article[9] that investigated epidemiological characteristics of patients with acute TSCI in the government-funded healthcare sector in Cape Town. The variables were incidence rate, gender, age, aetiology, presence of spinal fractures and associated injuries, number of patients who underwent spinal surgery, neurological level of injury (according to the American Spinal Injury Association Impairment Scale (AIS)) and length of hospital stay. In addition, previously unpublished data, specifically ethnicity, pre-injury employment and type of work (classified as blue and white collar), were analysed in the present study.
Data analysis
The annual crude incidence was first calculated for the private sector and then combined with the previously estimated incidence rate for the government-funded sector, with the aim of providing an estimate for the entire population at risk. Individuals at risk (defined as persons with private healthcare insurance) numbered 961 187 including all ages and 651 685 including only those aged ≥18 years. Descriptive statistics were used to describe the profile of the two cohorts in terms of sociodemographic and injury characteristics, extent of the injury and duration of hospital stay. Results, depending on the normality of the data, were expressed as counts with percentages, means with standard deviations, or medians with ranges. Differences between cohorts were computed using the Mann-Whitney (7-test for continuous variables (age and duration of hospital stay) owing to non-normal data. For categorical variables, Fisher's exact test was used owing to assumptions not being fulfilled for the x2 test.
Results
Incidence
The annual crude incidence of TSCI in the private sector population was 20 per million (95% confidence interval (CI) 11.6 - 34.4), which was significantly lower than that observed in the government-funded healthcare sector (p<0.0001). Taking both sectors together, the incidence rate was estimated at 61.1 per million (95% CI 52.4 - 71.4) (Table 1).
Sociodemographic, aetiology and injury characteristics
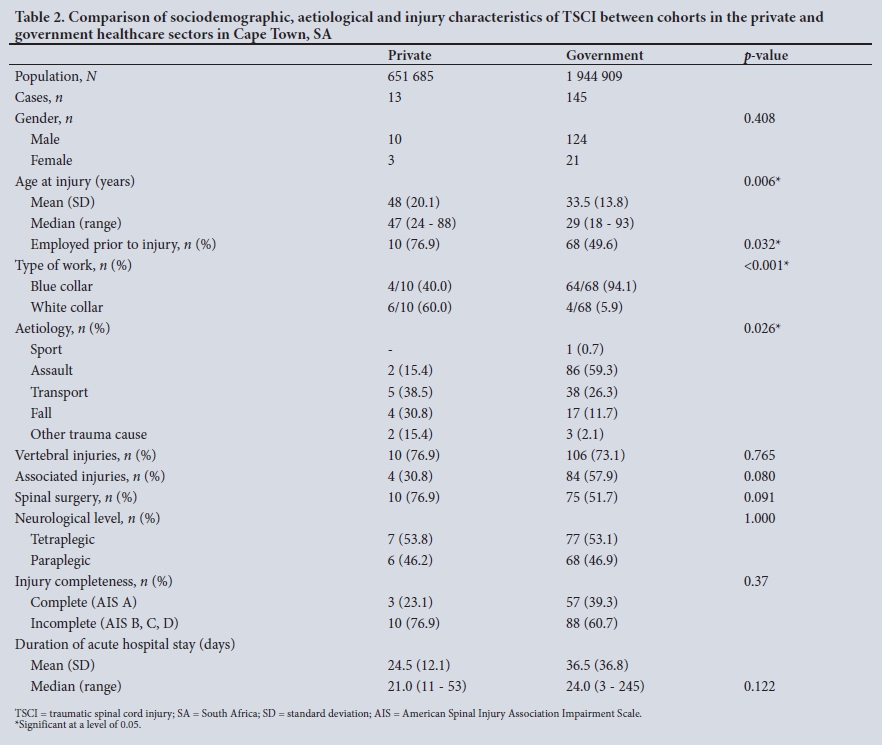
The private sector cohort differed significantly from their counterparts in the government-funded sector with regard to age and employment at the time of injury. The median age at injury in the private sector cohort was 47 years, as opposed to 29 years in the government-funded group (p=0.006). Both cohorts consisted of more males than females. The main cause of injury in the private sector cohort was transport-related, as opposed to assault in the government-funded group. This difference was significant (p=0.026). Fewer survivors in the private sector than in the government sector presented with associated injuries. No significant differences between the cohorts were noted concerning subclassification (neurological level) of spinal cord injury (SCI), completeness of injury (AIS A v. AIS B, C, D) and duration of acute hospital stay (Table 2).
Age differences across aetiologies in the two healthcare sectors
Age at injury was found to differ significantly between the cohorts. The median age in the government cohort was lowest for the assault category (26 years) and highest for falls (48 years). In the private sector, age was also lowest in the assault category, but the median was higher (38 years) than in the government cohort. The median ages for transport-related and falls injuries in the private sector were 42 and 70 years, respectively. Furthermore, no statistical difference was found in the median age of survivors in the private sector across the aetiological categories. These median ages per stratified cause of injury were significantly different from those in the government sector (p<0.001).
Discussion
The main objective of this study was to investigate the incidence, aetiology and injury characteristics of TSCI in the Cape Town population with private healthcare insurance, and compare their epidemiological characteristics with findings in the government sector. The results suggest not only that the annual incidence rate is lower than that for the population with government-funded healthcare, but that the cohorts differ with regard to age at injury, socioeconomic status and main cause of injury.
In this population-based study, 13 individuals with acute TSCI in the private sector were identified for the 1-year period. The annual incidence rate was significantly lower in this population than in the government-funded sector. This finding was surprising given that this sample came from the same catchment area for which an incidence of 75.6 per million was reported for the population with government-funded healthcare. One explanation could be the low occurrence of assault-related TSCI in the private cohort, while assault was the main cause of TSCI in the government cohort. The reason for fewer assault-related injuries among individuals with private healthcare could be their higher socioeconomic position, with less exposure to violent crimes.[14,15]
Significant differences between the cohorts were found for age at injury and main cause of injury. The mean and median age differences between the cohorts were ~15 and 18 years, respectively, with transport-related accidents the main cause of injury in the private sector v. assault in the government cohort. The age difference could be attributed to fewer injuries that were caused by assault in the private cohort, since the median age of 26 years in the assault category in the government sector was significantly lower than for other aetiologies. These results suggested that younger survivors of TSCI in the government cohort were more likely to be exposed to interpersonal violence. More studies are warranted to specifically investigate the influence of socioeconomic status on exposure to violent crimes and resultant injuries.
The findings with regard to socioeconomic status were not surprising, in that most individuals with private healthcare insurance were employed, with higher-income jobs than those in the government sector. We have discussed the differences in incidence and causes of injury between the cohorts based on socioeconomic disparity. However, the likelihood of engaging in violence or being a victim of a violent crime and the perceived importance of road safety are highly influenced by the environment in which an individual lives. Societal problems that could contribute to the risk of TSCI in SA are diverse, and a socioecological approach to prevention could highlight underlying processes leading to an increased susceptibility to TSCI.[16,17]
We found a significant difference in the incidence of TSCI between populations with private and government-funded healthcare, highlighting the need to assess whether resources are adequate to meet demands in the public sector. This investigation is necessary, since we noted that patients with government-funded care had more associated injuries, probably owing to the difference in causes of injury, and received spinal surgery less frequently. These observations led to the development of a multicentre study to assess the impact of processes of care on mortality following TSCI in the public sector. This information could therefore be used to strengthen systems of care and improve health policy specific to SCI in SA. In addition, future epidemiological studies should have a longer surveillance period, include the whole of SA, and investigate TSCI across all age groups, including children and adolescents, in order to understand the full burden of this devastating condition.
Study strengths and limitations
The main strength of this study was the use of a similar population-based design in both the sectors. In addition, the international SCI basic core data set was used, as recommended, with the aim of facilitating meaningful comparison between two cohorts. The study also had some limitations. First, the sample size of the private cohort was small, probably because the observation period was 1 year only and the rate of TSCI in this group was low. Secondly, the care of SCI is not centralised in the private healthcare system as it is in the government system, so the possibility of missing isolated cases of individuals seeking private care outside the study setting could not be dismissed.
Conclusions
This was the first population-based study to describe the epidemiological characteristics of TSCI in both the private and government healthcare sectors, thereby addressing the entire population at risk. Survivors of TSCI in the private sector differed from those with government-funded healthcare with regard to incidence rate, age, aetiology and socioeconomic status. We learnt that more than one main preventive strategy should apply to one catchment area.
Declaration. None.
Acknowledgements. We thank all the study participants and participating hospitals.
Author contributions. JP: contributed to study conception and design, assisted with manuscript drafting and review, and procured funds for this study; JB: assisted with data collection and review of the manuscript; CJ: conceived the study aim and design, managed data collection and data analysis, drafted the first version of the manuscript and addressed authors' comments.
Funding. This work was supported by the National Research Foundation of South Africa. The funding agency had no role in the design of the study, the analyses or the writing of the article.
Conflicts of interest. None.
References
1. Divanoglou A, Westgren N, Bjelak S, Levi R. Medical conditions and outcomes at 1 year after acute traumatic spinal cord injury in a Greek and a Swedish region: A prospective, population-based study Spinal Cord 2010;48(6):470-476. https://doi.org/10.1038/sc.2009.147 [ Links ]
2. Joseph C, Nilsson Wikmar L. Prevalence of secondary medical complications and risk factors for pressure ulcers after traumatic spinal cord injury during acute care in South Africa. Spinal Cord 2015;54(7):535-539. https://doi.org/10.1038/sc.2015.189 [ Links ]
3. World Health Organization and International Spinal Cord Society. International perspective on spinal cord injury. 2013. http://www.who.int/mediacentre/factsheets/fs384/en/ (accessed 11 October 2017). [ Links ]
4. Dahlberg A, Kotila M, Kautiaien H, Alaranta H. Functional independence in persons with spinal cord injury in Helsinki. J Rehabil Med 2003;35(5):217-220. https://doi.org/10.1080/16501970306092 [ Links ]
5. Lofvenmark I, Norrbrink C, Nilsson Wikmar L, Lofgren M. 'The moment I leave my home - there will be massive challenges': Experiences of living with a spinal cord injury in Botswana. Disabil Rehabil 2015;38(15):1483-1492. https://doi.org/10.3109/09638288.2015.1106596 [ Links ]
6. Cripps RA, Lee BB, Wing P, Weerts E, Mackay J, Brown D. A global map for traumatic spinal cord injury epidemiology: Towards a living data repository for injury prevention. Spinal Cord 2011;49(4):493-501. https://doi.org/10.1038/sc.2010.146 [ Links ]
7. Lee BB, Cripps RA, Fitzharris M, Wing PC. The global map for traumatic spinal cord injury epidemiology: Update 2011, global incidence rate. Spinal Cord 2014;52(2):110-116. https://doi.org/10.1038/sc.2012.158 [ Links ]
8. Rahimi-Movaghar V, Sayyah MK, Akbari H, et al. Epidemiology of traumatic spinal cord injury in developing countries: A systematic review. Neuroepidemiology 2013;41(2):65-85. https://doi.org/10.1159/000350710 [ Links ]
9. Joseph C, Delcarme A, Vlok I, et al. Incidence and aetiology of traumatic spinal cord injury in Cape Town, South Africa: A prospective, population-based study. Spinal Cord 2015;53(9):692-696. https://doi.org/10.1038/sc.2015.51 [ Links ]
10. Statistics South Africa. Census 2011 (Statistical release - P0301.4). Pretoria: Stats SA, 2011. https://www.statssa.gov.za/publications/P03014/P030142011.pdf (accessed 15 October 2017). [ Links ]
11. DeVivo M, Biering-Sorensen F, Charlifue S, et al. International Spinal Cord Injury Core Data Set. Spinal Cord 2006;44(9):535-540. https://doi.org/10.1038/sj.sc.3101958 [ Links ]
12. DeVivo MJ, Biering-Sorensen F, New P, Chen Y. Standardization of data analysis and reporting of results from the International Spinal Cord Injury Core Data Set. Spinal Cord 2011;49(5):596-599. https://doi.org/10.1038/sc.2010.172 [ Links ]
13. Waring WP, Biering-Sorensen F, Burns S, et al. 2009 review and revisions of the International Standards for the Neurological Classification of Spinal Cord Injury. J Spinal Cord Med 2010;33(4):346-352. https://doi.org/10.1080/10790268.2010.11689712 [ Links ]
14. Hsieh C-C, Pugh MD. Poverty, income inequality, and violent crime: A meta-analysis of recent aggregate data studies. Crim Justice Rev 1993;18(2):182-202. https://doi.org/10.1177/073401689301800203 [ Links ]
15. Doolan K, Ehrlich R, Myer L. Experience of violence and socioeconomic position in South Africa: A national study. PLoS One 2007;2(12)e1290. https://doi.org/10.1371/journal.pone.0001290 [ Links ]
16. Hanson DW, Finch CF, Allegrante JP, Sleet D. Closing the gap between injury prevention research and community safety promotion practice: Revisiting the public health model. Public Health Rep 2012;127(2):147-155. https://doi.org/10.1177/003335491212700203 [ Links ]
17. Seedat M, van Niekerk A, Jewkes R, Suffla S, Ratele K. Violence and injuries in South Africa: Prioritising an agenda for prevention. Lancet 2009;374(9694):1011-1022. https://doi.org/10.1016/S0140-6736(09)60948-X [ Links ]
 Correspondence:
Correspondence:
C Joseph
conran.joseph@ki.se
cjoseph@uwc.ac.za
Accepted 15 May 2018


{kind=link}
{kind=link}