










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.108 n.11 Pretoria Nov. 2018
http://dx.doi.org/10.7196/samj.2018.v108i11.13227
RESEARCH
Twenty-four-hour oesophageal pH studies in rural Eastern Cape Province, South Africa
E J NdebiaI; A M SammonII
IPhD; Department of Human Biology, Faculty of Health Sciences, Walter Sisulu University, Mthatha, South Africa
IIMD, PRCS; Department of Human Biology, Faculty of Health Sciences, Walter Sisulu University, Mthatha, South Africa
ABSTRACT
BACKGROUND. Recent studies in rural Eastern Cape Province, South Africa, have shown an increased number of non-acid gastro-oesophageal reflux events, an increase in baseline gastric pH compared with other published series, and evidence suggestive of duodenogastric reflux. There are no published data on oesophageal pH in this community or in Africa.
OBJECTIVES. To ascertain whether oesophageal pH in this rural community is within normal limits.
METHODS. We carried out 24-hour oesophageal pH/impedance studies on 91 participants. Analysis was carried out using computer software to determine 24-hour percentage times of oesophageal pH above 4, 5, 6, 7 and 8. Oesophageal pH during each episode of non-acid reflux was also recorded.
RESULTS. Participants were from Canzibe in rural Eastern Cape. Of the studies, 72 were satisfactory and showed 24-hour percentage times with an oesophageal pH >6 of 69.3/35.12/51.16 (upright/supine/total); percentage times with a pH >7 were 12.66/3.44/8.86 and those with a pH >8 were 0.48/0.21/0.37. These results are within the range of other published series. Of episodes of non-acid reflux, 90.2% were associated with an oesophageal pH of 4 - 7.
CONCLUSIONS. Baseline oesophageal pH is not significantly affected by the increased numbers of non-acid gastro-oesophageal reflux events reported in this community. If there is a pathogenic effect of non-acid reflux in the Eastern Cape, it does not appear to be mediated through raised oesophageal pH.
The Eastern Cape Province of South Africa (SA) has a very high incidence of squamous cell cancer of the oesophagus. Recent studies of oesophageal pH/impedance in the Eastern Cape have shown significant differences from other world series: episodes of total reflux and of non-acid reflux are increased, intragastric pH is elevated, and there is evidence supportive of duodenogastric reflux.
Objectives
To investigate 24-hour oesophageal pH in individuals from this high-risk area.
Methods
Ethical clearance was obtained from the Research Committee of Walter Sisulu University (ref. no. 00011A-04). Healthy adult volunteers aged 18-65 years were recruited from the villages around Canzibe Hospital, near the town of Mthatha in the rural Eastern Cape. Participants were chosen using a self-exclusion questionnaire and not on the basis of diet, education or income. Volunteers with upper gastrointestinal (GI) symptoms were not admitted to the study No GI endoscopic information was available. All the volunteers gave informed consent.
We used a pressure transducer to identify the upper and lower oesophageal sphincters. After calibration we inserted a pH/MMl catheter (K6011-E1-0782; Unisensor, Switzerland) transnasally, positioning the lower pH electrode 10 cm below the lower oesophageal sphincter (LOS) and the upper pH electrode 5 cm above the LOS. Participants went home with the catheter secured in place with tape and attached to an ambulatory pH/impedance recorder (Ohmega; MMS, Netherlands). They were requested to continue their normal activities, and to record episodes of sleep and mealtimes. pH and impedance values were sampled 50 times per second. At the end of a 24-hour recording time the catheter was removed and all the stored data were downloaded to a computer for analysis using the software provided by the manufacturers of the system (MMS Software, version 8.19).
The software package was used to provide percentage times for each participant for pH measured at the electrode placed 5 cm above the LOS. Each individual record was analysed by the computer programme and examined by two observers independently.
Acid reflux was defined as a reflux episode where the oesophageal pH decreases to <4, or that occurs when the oesophageal pH is <4.P Reflux episodes in which the pH was >4 were classified as non-acid reflux (NAR).
Results
Ninety-one participants were recruited. Nineteen records were found to be unsatisfactory because of failure of the participant to record meals or sleep pattern, recording of <23 hours, technical failure of the equipment, displacement of the catheter, or a minimum recorded pH of >4. Of the final 72 participants whose records were found to be satisfactory, 29 were male. The age range was 22 - 67 years (median 42). All were black Africans.
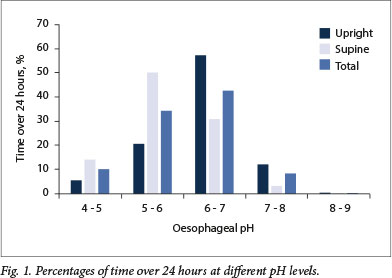
Twenty-four-hour percentage times with an oesophageal pH >6 were 69.3/35.12/51.16 (upright/supine/total). Times with a pH >7 were 12.66/3.44/8.86, and times with a pH >8 were 0.48/0.21/0.37.
Over 24 hours, oesophageal pH was found to be within the range 5 - 7 for 77.1% of the time. The pH was >7 for 8.86% of the time and >8 for 0.37% (Fig. 1).
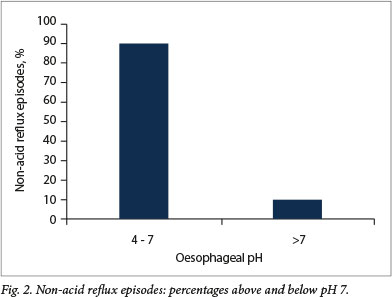
Of NAR episodes, 90.2% were between pH4 and pH7 (Fig. 2) The nadir recorded individual pH range was 0 - 3.4 (mean 1.24). Of the episodes, 26.7% were liquid only and 73.3% mixed liquid and gas. Gas-only refluxes were not included in the calculations. NARs ranged from 0.2 to 219 seconds in duration (mean 17.7).
Mean oesophageal pHs were upright 6.46 and supine 5.46.
Discussion
Despite the previously reported increased ambient gastric pH and increased NAR in this community,[1,2] the results of our study of oesophageal pH compare well with those of other published studies, and can be taken as normal.
The pH/impedance catheter system is established as reliable in providing accurate results over 24 hours. The frequency of recording ensures that all episodes of reflux and the full extent of high and low pHs are recorded. There was a high rate of success despite use of the equipment in an uncontrolled rural environment.
The results offer information about upper GI function in an area with a high incidence of squamous cell cancer of the oesophagus. We have shown previously that the number of NAR episodes in this group of volunteers was higher than reported in other published series. [1] A potential result of increased NAR is an increased mean oesophageal pH. Our results do not show an increase: the mean upright pH was 6.46, which compares with the upright pH of 6.6 in the study by Tutuian et al.[4]
Of NAR episodes in the present study, 90% occurred at a pH that is within the normal range of 5 - 7 for the oesophagus. The time scale of NAR episodes is very short, so episodes of pH higher than the normal upper limit of 7 are few and of short duration, and make little contribution to the mean oesophageal pH. The pH of the oesophagus when an individual is upright is normally determined by saliva.[5] Oesophageal pH is lower when supine, normally 5 - 6 at night, when the flow of saliva ceases. This is reflected in our results.
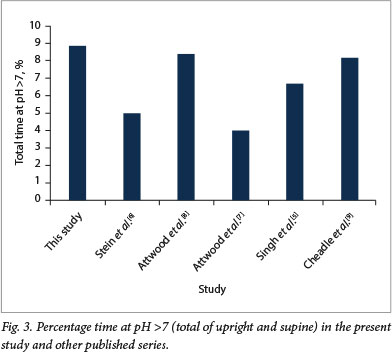
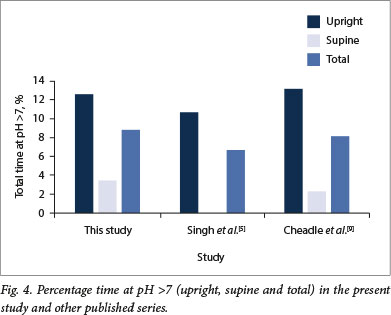
Total time at pH >7 in our series (8.86%) is at the upper end of normal, as shown in other published studies[5-8] (Fig. 3). For studies with a breakdown into upright/supine/total percentage time at pH >7, our results at 12.66/3.44/8.86 were similar to those of Cheadle et al [9] (13.2/2.3/8.16) and Singh et al.[5] (10.7/0.0/6.7) (Fig. 4).
On its own, pH is not generally accepted as a good predictor of duodenogastric reflux; however, in the present study there were some episodes of pH levels >8 that might be regarded as evidence of reflux of alkaline upper GI content.[7]
Iijima et al.[10]showed an association of raised intragastric pH with squamous cell cancer of the oesophagus, and believed it to be aetiologically significant. Uno et al[11] in Japan and Kgomo et in Pretoria, SA, have both shown an association of NAR with squamous cell cancer of the oesophagus, and believe it to be aetiologically significant. The pH of NAR episodes may affect the biological activity of the refluxate content. Alternatively, the raised pH of NAR may reflect the origin of the refluxate from the more alkaline duodenum/ jejunum.
Proposed aetiological factors for squamous cell cancer of the oesophagus in rural Eastern Cape are many, and have included alcohol, tobacco, wild vegetables, environmental carcinogens, contaminants of maize, stored maize meal and dietary deficiencies. [13] The identification of NAR as a mechanism associated with carcinogenic change may be a significant step forward.
Study limitations
In this population study we did not attempt to identify factors such as smoking and alcohol consumption, which may affect reflux. The self-exclusion method includes the possibility of unintentional selection bias. The moderate number of subjects whose records were unsatisfactory due to volunteer failures of recording may have created a sampling bias.
Conclusions
Twenty-four-hour oesophageal pH in the community studied is normal. If an association between NAR and squamous cell cancer of the oesophagus is present in the Eastern Cape, this study demonstrates that the association is not mediated by a raised oesophageal pH. Further research on the content of refluxate in this community may provide answers.
Declaration. None.
Acknowledgements. None.
Author contributions. EJN took part in the design of the study carried out the study took part in analysing the results and was involved in preparation and finalising of the article. AMS took part in the design of the study took part in analysing the results, wrote the first draft of the article and was involved in the finalising and submission of the article.
Funding. This work is based on research supported wholly by the National Research Foundation of South Africa (UID: 107436, ref.: TTK160507164324) and the South African Medical Research Council through its Self-Initiated Research Grant awarded to EJN.
Conflicts of interest. None.
References
1. Ndebia EJ, Sammon AM, Umapathy E, Iputo JE. Normal values of 24-hour ambulatory esophageal impedance-pH monitoring In a rural South African cohort of healthy participants. Dls Esophagus 2015,4(11).385-391. https://doi.org/10.1111/dote.l2333 [ Links ]
2. Sammon AM, Ndebia EJ, Umapathy E, Iputo JE. 24 hour measurement of gastric pH in rural South Africa Gastroenterol Res Pract 2015,2015, article ID 658106. https://doi.org/10.1155/2015/65810e [ Links ]
3. Sifrim D, Castell, D, Dent J, Kahrilas PJ. Gastro-oesophageal reflux monitoring Review and consensus report on detection and definitions of acid, non-acid, and gas reflux. Gut 2004,53(7).1024-1031. https://doi.org/10.1136/gut.2003.033290 [ Links ]
4. Tutulan R, Katz PO, Bohenek W, Castell DO. Dose-dependent control of IntragastricpH by pantoprazole, 10, 20 or 40mg, In healthy volunteers. Aliment Pharmacol Ther 2002,16(4):829-836. https://doi.org/101046/j.1365-2036.2002.01232.x [ Links ]
5. Singh S, Bradley LA, Richter JE. Determinants of oesophageal "alkaline' pH environment in controls and patients with gastro-oesophageal reflux disease. Gut 1993,34(3).309-316. https://doi.org/10.1136/gut.34.3.309 [ Links ]
6. Stein H, Feussner H, Kauer W, DeMeester TR, Siewert JR Alkaline gastroesophageal reflux Assessment by ambulatory aspiration and pH monitoring Am J Surg 1994,167(1).163-168. https://doi.org/10.1016/0002-9610(94)90068 [ Links ]
7. Attwood SEA, DeMeester TR Bremner CG, Barlow AP, Hinder RA. Alkaline gastroesophageal reflux Implications in the development of complications in Barrett's columnar-lined lower esophagus. Surgery 1989,106(4);764-770. [ Links ]
8. Attwood SEA, Ball CS, Barlow AP, Jenkinson L, Norris TL, Watson A. Role of intragastric and intraoesophageal alkalinisation in the genesis of complications in Barrett's columnar lined lower oesophagus. Gut 1993,34(5).11-15. https://doi.org/10.1016/0002-9610(94)90068 [ Links ]
9. Cheadle WG, Vitale GC, Sadek SA, Cuschieri A. Computerised ambulatory esophageal pH monitoring in 50 asymptomatic volunteer subjects. Am J Surg 1988,155(3).503-508. https://doi.org/10.1016/s0002-9610(88)80123-5 [ Links ]
10. Iijima K, Koike T, Abe Y, et al. Gastric hyposecretton in esophageal squamous-cell carcinomas. Dig Dis Sci 2010;55(5) 1349-1355. https://doi.org/10.1007/s10620-009-0853-x [ Links ]
11. Uno K, Iijima K, Hatta W, et al Direct measurement of gastroesophageal reflux episodes in patients with squamous cell cancer by 24-h pH-lmpedance monitoring Am J Gastroenterol 2011,106(11).1923-1929. https://doi.org/10.1038/ajg2011.282 [ Links ]
12. Kgomo M, Mokoena Tr" Ker JA. Non-acid gastro-oesophageal reflux is associated with squamous cell carcinoma of the oesophagus. BMJ Open Gastroenterol 2017,4x000180. https://doi.org/10.1136/bmjgast-2017-000180 [ Links ]
13. Sammon AM. Squamous cancer of the oesophagus in Africa. 2009. scoafrica.org (accessed 27 September 2018). [ Links ]
 Correspondence:
Correspondence:
A M Sammon
alastair.sammon@gmail.com
Accepted 7 May 2018

