










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSAMJ: South African Medical Journal
versão On-line ISSN 2078-5135
versão impressa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.108 no.11 Pretoria Nov. 2018
http://dx.doi.org/10.7196/samj.2018.v108i11.13067
RESEARCH
Hearing outcomes in children with meningitis at Red Cross War Memorial Children's Hospital, Cape Town, South Africa: A silent crisis
S KuschkeI; N GoncalvesII; S PeerIII
IBCommunication Pathology, MCommunication Pathology; Department of Audiology, Red Cross War Memorial Children's Hospital and Faculty of Health Sciences, University of Cape Town, South Africa
IIBSc Hons, MB BCh; Department of Otolaryngology, Red Cross War Memorial Children's Hospital and Faculty of Health Sciences, University of Cape Town, South Africa
IIIMB BCh, MMed Otol, FCORL (SA); Department of Otolaryngology, Red Cross War Memorial Children's Hospital and Faculty of Health Sciences, University of Cape Town, South Africa
ABSTRACT
BACKGROUND. Bacterial meningitis is one of the most common causes of hearing loss. Hearing loss develops within the first few days following the onset of meningitis, highlighting the importance of early audiology referrals. Post-meningitis hearing loss may lead to cochlear ossification, making traditional cochlear implantation impossible.
OBJECTIVES. To determine the duration of time from meningitis diagnosis to audiology referral. A second objective was to determine the prevalence and severity of meningitis-related sensorineural hearing loss (SNHL) at Red Cross War Memorial Children's Hospital (RCWMCH), a paediatric tertiary hospital in Cape Town, South Africa (SA).
METHODS. A retrospective folder review of all children diagnosed with meningitis and referred for audiological evaluation was conducted over an 18-month period between 1 January 2015 and 30 June 2016. Descriptive statistical methods were used for data analysis.
RESULTS. The total number of inpatients diagnosed with unspecified meningitis at RCWMCH between January 2015 and June 2016 was 345. The total number diagnosed with bacterial meningitis was 68. Only 16 children with meningitis (23.5%) were referred to the Department of Audiology at RCWMCH over the 18-month period. Twelve children had confirmed bacterial meningitis. All the children had up-to-date immunisations. The mean (standard deviation) time from diagnosis to audiology referral was 17 weeks (16.9; range 1 - 60). The overall prevalence of hearing loss was 42.8%. Four children (28.5%) were diagnosed with severe to profound SNHL.
CONCLUSIONS. Less than a quarter of all children diagnosed with bacterial meningitis at RCWMCH over the 18-month study period were referred to audiology. Frequent delays in referrals for audiological assessment following meningitis were noted. This may indicate a lack of awareness on the part of doctors. Healthcare practitioners need to be made aware of the need for prompt audiological testing for children with meningitis. In SA, local guidelines for early diagnosis and monitoring of hearing in children who have had meningitis should be developed in order to improve hearing outcomes.
Bacterial meningitis has been identified as one of the most common causes of hearing impairment in both adults and children.[1] Globally, 10% of children with acute bacterial meningitis may acquire some degree of permanent bilateral or unilateral hearing loss, which usually develops within 48 hours of hospital admission.[2] South African (SA) studies have documented bacterial meningitis as a risk factor for hearing loss.[3,4] Furthermore, 6% of all acquired sensorineural hearing loss (SNHL) in the paediatric population can be attributed to bacterial meningitis.[3] A 12-year study examining the risk of neurological abnormalities and central auditory dysfunction following meningitis reported that SNHL may remain stable, or may fluctuate spontaneously.[2]
Permanent and transient hearing loss develops within the first few days after the onset of meningitis,[1] highlighting the importance of early audiology referrals and accurate audiological diagnosis.[5] It has been reported that delayed diagnosis of hearing loss, which results in the lack of sufficient or quality language input during the critical period of speech and language development, may lead to poor language and academic performance.[6] Children who have had meningitis should therefore ideally be referred for sensitive and comprehensive audiological assessments before discharge from hospital. Despite a large body of evidence illustrating the need for post-meningitis audiological evaluation, many affected children are not assessed and are often lost to follow-up. The poor follow-up rate is probably due to lack of referral and may indicate a lack of awareness that hearing assessments following meningitis are necessary.[1,2,5]
Post-meningitis hearing loss may lead to cochlear ossification, an inflammatory process where the inner ear becomes fibrosed and eventually ossified. Cochlear ossification, which results in increased risk of partial insertion of the cochlear implant electrode, may occur as early as 3 - 4 weeks after the onset of meningitis.[7,8] Findings of a retrospective review of 47 cochlear implants done in patients with bilateral profound hearing loss following bacterial meningitis showed that cochlear ossification, diagnosed with magnetic resonance imaging, occurred in almost half (44%) of patients.[9] Ossification typically starts at the round window, proceeding apically.[9] Traditional cochlear implantation methods (round window or cochleostomy insertion) are therefore not possible. Any child with post-meningitis severe to profound hearing loss therefore needs urgent temporal bone imaging for cochlear ossification and subsequent referral for a cochlear implant.
Objectives
To determine the duration of time from meningitis diagnosis to audiology referral. A second objective was to determine the prevalence and degree of severity of meningitis-related SNHL at Red Cross War Memorial Children's Hospital (RCWMCH), a paediatric tertiary hospital in Cape Town, SA.
Methods
Setting
RCWMCH is one of only two dedicated paediatric academic hospitals in sub-Saharan Africa. It serves children from birth to 13 years of age. The Department of Audiology at RCWMCH assesses and treats ~300 children per month.
Ethical approval
The study was approved by the University of Cape Town (UCT) Department of Surgery (ref. no. 2016/075) and the UCT Human Resources Ethics Committee (ref. no. 028/2017).
Procedure
A retrospective folder review of all children diagnosed with meningitis and referred for audiological evaluation was conducted over an 18-month period between 1 January 2015 and 30 June 2016. A large amount of data can be accumulated for patients with a retrospective review; however, some limitations of this design include incomplete data sets, illegible handwriting in patient records, and missing records.[10] Data collected included demographic information, age at diagnosis, sex, and clinical and audiometric information. Audiometric information included time from meningitis diagnosis to audiology referral, as well as type and degree of hearing loss. Clinical information included lumbar puncture (LP) biochemistry and microbiology results, and computed tomography (CT) brain scan results.
The audiological test battery included otoacoustic emissions, tympanometry and auditory brainstem responses (ABRs) where indicated. Behavioural audiometry (pure tone testing) was used where age-appropriate, to determine the degree and configuration of the hearing loss. Hearing outcomes, including the degree of the hearing loss in each ear, were determined. According to the American Speech and Hearing Association, normal peripheral hearing was defined as thresholds <15 decibels of hearing loss (dB HL).[11] Hearing loss was present if thresholds were >15 dB HL across frequencies (250 - 8 000 Hz).
Data were captured on a Microsoft Excel spreadsheet, 2010 version (Microsoft, USA). Descriptive statistical methods were used to analyse patient information and to describe the clinical and audiometric characteristics of the patients.
Results
Demographics
The total number of inpatients diagnosed with unspecified meningitis at RCWMCH between January 2015 and June 2016 was 345. The total number of inpatients diagnosed with bacterial meningitis was 68. A total of 16 children (23.5%) with suspected or confirmed meningitis were referred to the Department of Audiology at RCWMCH over the above 18-month period. Two children were excluded, one with viral encephalitis and the other with neurocysticercosis. Eight were male (57.1%) and 6 were female (42.9%). The mean (standard deviation (SD)) age at diagnosis was 3.1 months (2.3; range 1 - 8).
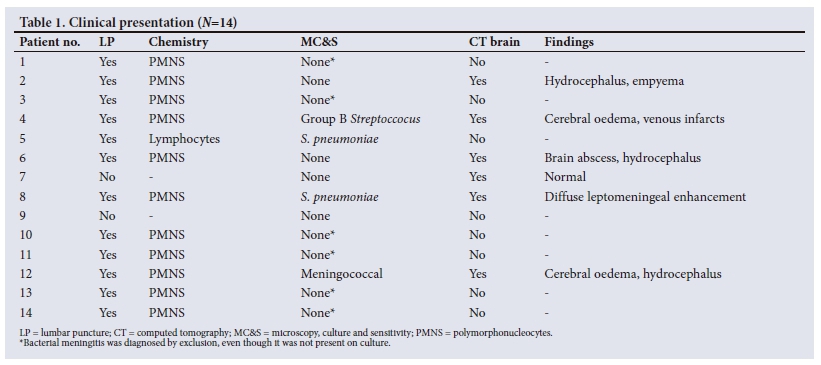
Clinical findings
Twelve children had confirmed bacterial meningitis on LP. The remaining 2 children commenced treatment based on clinical presentation alone. The most common organism cultured was Streptococcus pneumoniae, found in 2/12 children (16.7%). There was one case of meningococcal meningitis. All the children had up-to-date immunisations. Brain CT scans were performed in 6/14 children (42.9%). Features of meningitis were reported in all but one case (5/6, 83.3%). Intracranial complications were reported in 5/14 children (35.7%). No features of middle-ear effusions or opacification of the mastoid air cell system that could be attributed to an otogenic cause were detected in any of the scans. All the children were treated with intravenous antibiotics.
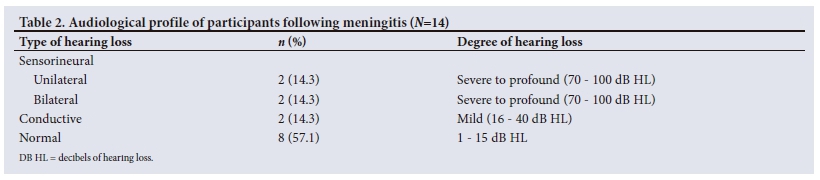
Audiology findings
The mean (SD) time from diagnosis to audiology referral was 17 weeks (16.9; range 1 - 60). One child was referred almost 1 year after having meningitis. The overall prevalence of hearing loss was 42.9%. Table 2 depicts the audiological profile of participants following meningitis.
Discussion
The objective of this study was to determine the hearing outcomes of children with meningitis. Our results showed that nearly one-third of children presented with severe to profound SNHL, a higher incidence of post-meningitis hearing loss than reported in the international literature.[12] The higher incidence could be attributed to the study population being from a tertiary institution, which typically receives a high proportion of critically ill children. Karanja et al.[13] also reported a high prevalence of SNHL (43.4%) following meningitis at a tertiary hospital. The higher prevalence of post-meningitis SNHL in that study may be attributed to their relatively large sample size. High incidences of meningitis have been reported in developing countries, owing to poor access to healthcare and limited-resource environments.[14]
A major finding in the current study was the delay in referral to audiology following meningitis. The average time from meningitis diagnosis to referral was 17 weeks, with one child being referred nearly 1 year after having meningitis. Less than a quarter (23.5%) of all children diagnosed with bacterial meningitis at RCWMCH over the 18-month study period were referred to audiology. The current literature suggests that ~40% of patients who have had bacterial meningitis in SA are not referred for audiological assessment.[1] Compared with developed countries, the referral rate in the current study is substantially lower. In the UK, 7.7 - 27% of children are not referred for audiological assessment following meningitis.[15] Furthermore, with nearly one-third of the children in the current study presenting with severe to profound hearing loss, the delay in referral and subsequent diagnosis may have had a detrimental impact on their eligibility for cochlear implantation.
Any child with bilateral severe to profound hearing loss and CT findings of cochlear ossification should be counselled on an aural rehabilitation approach, such as oral, aural or total communication. However, prompt audiological testing and appropriate referrals to an otolaryngologist and a cochlear implant team are crucial in early detection of children with profound hearing loss, whose families may choose to pursue cochlear implantation as the preferred aural rehabilitation option.
Despite the small sample size in the current study, our results highlight important factors that contribute to hearing outcomes following meningitis in SA. The audiological test battery included tympanometry without measuring acoustic reflexes, so potential objective evidence of hearing loss could have been missed. However, ABRs were done as an objective test where indicated. The participants in the study were confined to inpatients, so data from the outpatient department were not included in the audit, which may have skewed results. However, inclusion of outpatient referrals is a basis for future research.
Conclusions
Post-meningitis hearing outcomes in children at RCWMCH are similar to international findings. An important finding in the current study was the substantial delay in referral to audiology. Lack of awareness on the part of healthcare professionals regarding the need for audiological referrals and the appropriate timing thereof, and poor access to healthcare, could explain the high rate of delayed diagnoses of hearing impairment following meningitis. Recommended solutions in a resource-constrained environment include education of healthcare professionals in order to increase awareness of prompt audiological testing for children diagnosed with meningitis, which will result in early diagnosis and suitable management to improve hearing outcomes.
Update. Since the current study was conducted, the audiology and ENT departments at RCWMCH have embarked on an extensive awareness and education campaign, which resulted in an increased number of appropriate and early referrals.
Declaration. None.
Acknowledgements. We thank Ms Mon-Cheri Baatjes for her valuable contribution to earlier drafts of this article, as well as for her time and hard work in helping with data collection.
Author contributions. SK and SP designed the study, SK and NG contributed to data collection, SK, NG and SP contributed to data analysis, SK drafted the manuscript, and all authors contributed to and approved the final version of the manuscript.
Funding. None.
Conflicts of interest. None.
References
1. Khoza-Shangase K, Emma RR. Paediatric meningitis and hearing loss in a developing country: Exploring the current protocols regarding audiological management following meningitis. Afr J Infect Dis 2010;4(2):51-60. https://doi.org/10.4314/ajid.v4i2.55148 [ Links ]
2. Grimwood K, Nolan TM, Bond L, Anderson VA, Catroppa C, Keir EH. Risk factors for adverse outcomes of bacterial meningitis. J Paediatr Child Health 1996;32(5):457-462. https://doi.org/10.1111/j.1440-1754.1996.tb00949.x [ Links ]
3. Le Roux T, Swanepoel DW, Louw A, Vinck B, Tshifularo M. Profound childhood hearing loss in a South Africa cohort: Risk profile, diagnosis and age of intervention. Int J Pediatr Otorhinolaryngol 2015;79(1):8-14. https://doi.org/10.1016/j.ijporl.2014.09.033 [ Links ]
4. Swanepoel DW, Johl L, Pienaar D. Childhood hearing loss and risk profile in a South African population. Int J Pediatr Otorhinolaryngol 2013;77(3):394-398. https://doi.org/10.1016/j.ijporl.2012.11.034 [ Links ]
5. Smith RJH, Bale JF, White KR. Sensorineural hearing loss in children. Lancet 2005;365(9462):879-890. https://doi.org/10.1016/S0140-6736(05)71047-3 [ Links ]
6. Nicholas JG, Geers AE. Effects of early auditory experience on the spoken language of deaf children at 3 years of age. Ear Hear 2006;27(3):286-298. https://doi.org/10.1097%2F01.aud.0000215973.76912.c6 [ Links ]
7. Philippon D, Bergeron F, Ferron P, Bussières R. Cochlear implantation in postmeningitic deafness. Otol Neurotol 2010;31(1):83-87. https://doi.org/10.1097/MAO.0b013e3181c2a02d [ Links ]
8. Wilson C, Roberts A, Stephens D. Improving hearing assessment of children post-meningitis. Arch Dis Child 2003;88(11):976-977. https://doi.org/10.1136/adc.88.11.976 [ Links ]
9. Caye-Thomasen P, Dam MS, Omlandi SH, Mantoni M. Cochlear ossification in patients with profound hearing loss following bacterial meningitis. Acta Otolaryngol 2012;132(7):720-725. https://doi.org/10.3109/00016489.2012.656323 [ Links ]
10. Sedgwick P. Retrospective cohort studies: Advantages and disadvantages. BMJ 2014;348:1072. https://doi.org/10.1136/bmj.g1072 [ Links ]
11. Clark JG. Uses and abuses of hearing loss classification. ASHA 1981;23(7):493-500. https://www.researchgate.net/publication/16145943 (accessed 11 October 2018). [ Links ]
12. Von Gottberg A. Bacterial meningitis in the era of paediatric vaccination against the encapsulated pathogens: Bacterial meningitis is still prevalent worldwide in spite of effective vaccines. CME 2010;28(6):252-259. [ Links ]
13. Karanja BW, Oburra HO, Masinde P, Wamalwa D. Prevalence of hearing loss in children following bacterial meningitis in a tertiary referral hospital. BMC Res Notes 2014;7:138. https://doi.org/10.1186/1756-0500-7-138 [ Links ]
14. Kutz JW, Simon LM, Chennupati SK, Giannoni CM, Manolidis S. Clinical predictors for hearing loss in children with bacterial meningitis. Arch Otolaryngol Head Neck Surg 2006;132(9):941-945. https://doi.org/10.1001/archotol.132.9.941 [ Links ]
15. Merkus P, Free RH, Mylanus EAM. Dutch cochlear implant group (CI-ON) consensus protocol on postmeningitis hearing evaluation and treatment. Otol Neurotol 2010;31(8):1281-1286. https://doi.org/10.1097/MAO.0b013e3181f1fc58 [ Links ]
 Correspondence:
Correspondence:
S Kuschke
silvakuschke@gmail.com
Accepted 4 May 2018


{kind=link}
{kind=link}