










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSAMJ: South African Medical Journal
versión On-line ISSN 2078-5135
versión impresa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.108 no.11 Pretoria nov. 2018
http://dx.doi.org/10.7196/samj.2018.v108i11.13378
CME
Cardiac disease in pregnancy: When to raise the 'red flag'
P Soma-PillayI; J AnthonyII; S D MandondoIII
IMB ChB, Dip Obstet (SA), FCOG (SA), MMed (O et G), Cert Maternal and Fetal Medicine (SA), PhD; Department of Obstetrics and Gynaecology, Faculty of Health Sciences, Steve Biko Academic Hospital and University of Pretoria, South Africa
IIMB ChB, FCOG (SA), MPhil (Bio-ethics); Department of Obstetrics and Gynaecology, Faculty of Health Sciences, Groote Schuur Hospital and University of Cape Town, South Africa
IIIBSc, MB ChB, FCOG (SA); National Committee for the Confidential Enquiry into Maternal Deaths, East London, South Africa
ABSTRACT
Cardiac disease in pregnancy is an important cause of maternal morbidity and mortality and is the second most common cause of indirect maternal death in South Africa. Although most women with cardiac disease cope well throughout pregnancy, some conditions are associated with an increased risk. Appropriate management of cardiac disease in pregnancy requires expert assessment, risk categorisation and ongoing care. The objective of this article is to assist clinicians to identify and modify risk factors associated with cardiac disease in pregnancy and thus reduce avoidable morbidity and mortality.
Cardiac disease is a cause of maternal mortality in developed and developing countries globally. In the UK, the Confidential Enquiry into Maternal and Child Health (CEMACH) showed that the overall rate of mortality from cardiac disease rose from 7.3/1 000 000 births in 1982 - 1984 to 22.7/1 000 000 births in 2009 - 2011.[1,2] The institutional maternal mortality rate (iMMR) for cardiac disease was 2/100 000 during 2012 - 2014.[2] The major part of this increase is attributable to acquired heart disease.[1]
In South Africa (SA), according to the Saving Mothers 2011 - 2013: Sixth Report on Confidential Enquiries into Maternal Deaths,[3] there has been a steady increase in the iMMR for cardiac disease over the last 4 triennia. The iMMR for cardiac disease in 2005 - 2007 was 3.73, which has increased to 5.64 during 2008 - 2010 and to 6.00/100 000 live births in 2011 - 2013.[3] Cardiac disease is, therefore, after non-pregnancy-related infections, the second most common cause of indirect maternal death. In 2011 - 2013, the number of deaths due to peripartum cardiomyopathy was more than double that of complications related to rheumatic heart disease and formed 34% of the total number of cardiac deaths.
According to the Saving Mothers 2014 - 2016 report,[4] 35% of deaths in the medical and surgical disorders category were cardiac deaths (35.3%; n=165). The majority of deaths from cardiac disease are in the under-30-year age group (58%; n=95). HIV was not a significant risk factor, as 63% (n=105) of patients were HIV-negative. Sixty percent of maternal deaths occurred after delivery (n=99), with 56.6% of patients delivered by caesarean section. Thirty-five mothers (85.3%) who died of peripartum cardiomyopathy presented with acute symptoms in the postpartum period. Forty-four (27%) patients were managed at level 1 hospitals. Failure to make a diagnosis, incorrect management and delay in referring patients to the appropriate level of care were important factors that contributed to avoidable cardiac mortality.
As our population changes, more women with corrected congenital heart defects reach adulthood, and older mothers, smokers and obese women with ischaemic heart disease risks and rural clients with rheumatic heart disease become pregnant and require specialist care. Despite the potential for significant maternal morbidity, most patients with cardiac disease can expect a satisfactory outcome with careful prepregnancy, antenatal, intrapartum and postnatal management. This article aims to assist clinicians to identify cardiac clients at risk and reduce avoidable mortality.
Risk assessment: Estimation of maternal risk
Normal physiological pregnancy-related changes may aggravate underlying cardiac disease, leading to associated morbidity and mortality.
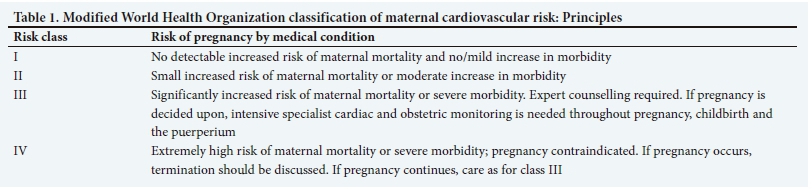
To estimate the risk of maternal cardiovascular complications, several approaches have been employed. Previously, the complications associated with pregnancy in women with heart disease (CARPREG) risk score was widely used, but the Task Force of the European Society of Cardiology recommends that maternal risk assessment should be carried out according to the modified World Health Organization (WHO) risk classification.[5] This classification integrates all known maternal cardiovascular risk factors, including underlying heart disease and any other comorbidities. It includes contraindications for pregnancy that are not incorporated in the CARPREG risk scores/ predictors.
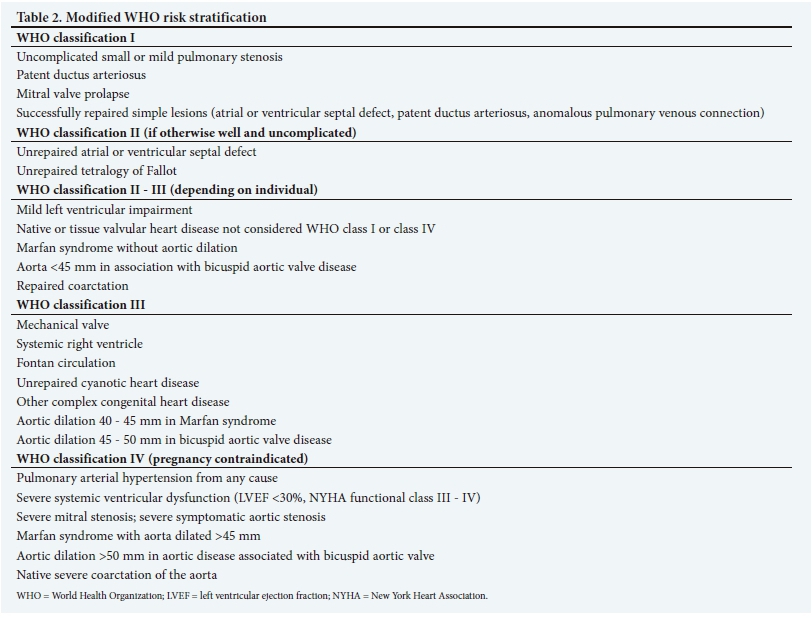
The general principles of this classification are depicted in Table 1, and a practical application is given in Table 2. For women in WHO class I, the risk is very low, and cardiology follow-up during pregnancy may be limited to one or two visits. Those in WHO class II are at low or moderate risk, and follow-up every trimester is recommended. For women in WHO class III, there is a high risk of complications, and frequent (monthly or bimonthly) cardiology and obstetric review during pregnancy is recommended. Women in WHO class IV should be advised against pregnancy but, if they become pregnant and refuse termination, monthly or bimonthly review is needed.[6] In the context of 'red-flag' disorders, patients with WHO class III and class IV conditions need continuous expert care and assessment throughout pregnancy, whereas all other patients with suspected or known cardiac disease in pregnancy require at least one early assessment by a combined obstetric and cardiology team to confirm a known or suspected diagnosis and to assign risk according to the WHO scoring system.
Rheumatic heart disease
Valvular heart lesions secondary to childhood rheumatic fever are important causes of maternal morbidity and mortality in developing countries.[7-9] Although many women with valve disease, especially less severe valve disease, cope well throughout pregnancy, there are some conditions in which the risk of pregnancy is considered prohibitive. A red light status should be conferred to pregnant women with the following conditions:
-
mitral stenosis
-
severe mitral regurgitation
-
severe aortic stenosis
-
baseline New York Heart Association (NYHA) functional class >II
-
valve lesions associated with severe left ventricular (LV) dysfunction or significant pulmonary hypertension
-
valvular disease in women living in low- and middle-income countries (LMICs).
Mitral stenosis
Haemodynamic changes in pregnancy, including increases in heart rate, cardiac output, red cell mass and plasma volume, can lead to increased left atrial pressures and cardiac decompensation. The most common complications in pregnancy are a decline in functional capacity, atrial arrhythmias, such as atrial fibrillation and pulmonary oedema.[10-12] Complications are associated with the severity of the stenosis and baseline NYHA functional class.[10,11,13] The Registry of Pregnancy and Cardiac Disease (ROPAC) found that the risk of heart failure in women with mild, moderate and severe stenosis was 15.8%, 31.8% and 48.1%, respectively.[14] These data are consistent with those in a study of 80 women with rheumatic valve stenosis, which reported pulmonary oedema in mild (24%), moderate (34%) and severe (56%) cases of mitral stenosis during pregnancy.[15] The degree of stenosis, the NYHA class and right ventricular systolic pressure in women with mild or moderate stenosis may help to distinguish between women who are likely to cope with pregnancy and those at risk of complications.[14] The ROPAC study found NYHA class >II to be an independent predictor of maternal cardiac events in pregnancy (odds ratio (OR) 3.77; 95% confidence interval (CI) 1.93 - 7.38).[14] Heart failure (7% v. 49%) and arrhythmic complications (2% v. 21%) are more likely to occur in women with NYHA class III or class IV than in women with NYHA class I or class II.[16]
The high rate of complications may be reduced with surgical intervention and close follow-up during pregnancy and the post-partum period. A percutaneous balloon mitral commissurotomy is effective for selected patients with isolated mitral valve stenosis, resulting in a rapid decrease in left atrial pressure and pulmonary arterial pressure.[17] Echocardiographic follow-up during pregnancy is important to detect early haemodynamic changes that may precede and possibly predict clinical deterioration.[14] In the ROPAC study, 30% of heart failure cases occurred in the first postpartum week. Therefore, during this time, haemodynamic monitoring should include efforts to avoid large fluctuations in pre- and after-load. Treatment of heart failure should be the same as for non-pregnant women.
Severe mitral regurgitation
Decreases in peripheral vascular resistance and blood pressure during pregnancy are believed to physiologically aid women with moderate and even severe regurgitation with normal left ventricular size and systolic function. However, the increased plasma volume and cardiac output may lead to heart failure and arrhythmia in women with severe mitral regurgitation, especially those with significant ventricular dilatation or dysfunction. In the ROPAC study, severe mitral regurgitation was associated with a significant risk of an adverse cardiac event in pregnancy (OR 5.25; 95% CI 1.86 - 14.9).[14]
Severe aortic stenosis
Increased cardiac output in pregnancy in the setting of a restricted fixed outflow obstruction is of major importance. Relief of inferior vena cava obstruction, autotransfusion from the contracting uterus and excessive fluid administration in the postpartum period may also be poorly tolerated. Most women with mild or moderate stenosis tolerate pregnancy well, while complications such as angina, tachyarrhythmias and pulmonary oedema may be seen in women with severe stenosis.[11,18] Complication rates of 10 - 42% have been reported.[11,18] Women who develop symptoms should be admitted to hospital for bedrest, and pulmonary oedema must be treated with diuretics. Aggressive diuresis, however, should be avoided as hypovolaemia may cause decreased placental perfusion. Percutaneous balloon valvuloplasty should be considered for women not responding to medical therapy, provided there is no significant regurgitation.
Valvular disease in women living in low- and middle-income countries
The prevalence of rheumatic heart disease in sub-Saharan Africa is high, with 2 - 3/1 000 among school-aged children who underwent clinical screening and a tenfold higher prevalence if echocardiographic screening was added.[19-21] The ROPAC study recommended percutaneous balloon mitral commissurotomy as a treatment option for young women with moderate or severe mitral stenosis who desire pregnancy, even if they are asymptomatic.[14] Despite the higher prevalence and more severe forms of mitral stenosis in LMICs, valvular interventions are more frequent in countries with advanced economies.[9] The problem of delay in patients seeking help, financial constraints, lack of information about pregnancy risks in women with heart disease and social and cultural drawbacks often preclude any appropriate prevention strategy in developing countries.[22] Consequently, management of patients remains a medical challenge. These factors contribute to the high maternal mortality rates in sub-Saharan Africa.[7,22]
Peripartum cardiomyopathy
Peripartum cardiomyopathy (PPCM) is an idiopathic form of cardiomyopathy presenting with heart failure secondary to LV dysfunction towards the end of pregnancy or in the months following delivery, where no other cause of heart failure is identified.[23] Most women present with severe acute heart failure, but even those presenting with more subtle symptoms can have long-term impaired cardiac function.[24] During 2011 - 2013, PPCM comprised 34% of cardiac maternal deaths in SA.[7] Forty-eight percent of these occurred in the postpartum period and all cases were newly diagnosed, as none of the maternal records documented a previous history of cardiomyopathy. Delayed diagnosis was an important avoidable factor identified by maternal death assessors in this audit.
All women presenting to the labour ward or emergency unit during pregnancy or up to 6 months post partum with symptoms of heart failure or shortness of breath should be red flagged. The National Committee on Confidential Enquiries into Maternal Deaths in SA recommends that clinicians should have a low threshold for investigating women presenting with cardiovascular risk factors, suspected rheumatic heart disease or symptoms such as shortness of breath or chest pain.[25] Appropriate investigations include an electrocardiogram (ECG), chest radiograph, echocardiogram and computed tomography (CT) pulmonary angiography. Evaluation of patients with suspected acute PPCM includes two parts, which should be performed simultaneously to allow timely diagnosis and treatment: evaluation of cardiopulmonary distress and confirmation of the diagnosis. The European Society of Cardiology study group on PPCM recommends that the presence of criteria defining cardiopulmonary distress should lead to intensive cardiac care unit admission: haemodynamic instability (systolic blood pressure <90 mmHg, heart rate >130 bpm or <45 bpm), respiratory distress (respiratory rate >25/minute, peripheral oxygen saturation <90%), or signs of tissue hypoperfusion with abnormal cellular oxygen metabolism (increased blood lactate >2.0 mmol/L; low central venous oxygen saturation <60 %, if available; altered mental state; cold, clammy, mottled skin; oliguria <0.5 mL/kg/h).[26] Echocardiography is used to confirm the diagnosis of suspected PPCM, assess concomitant or pre-existing cardiac disease, exclude complications such as thrombus formation and obtain prognostic information.[26]
Timely diagnosis and treatment are crucial. The management team should include cardiologists, intensivists, obstetricians, neonato-logists and anaesthetists. After initial treatment and stabilisation, the patient should be counselled about future risk, impact of subsequent pregnancies, duration of medical therapy and contraceptive options. The Heart Failure Association PPCM Study Group recommends 6-monthly follow-up until recovery to a LV ejection fraction (LVEF) >50%.[26] In women with LV recovery, who remain stable after tapering of heart failure drug therapy, an annual visit is recommended for up to 10 years. There is no consensus as to whether heart failure medication should be discontinued in women with recovered LV function.
Complications in pregnant women with prosthetic heart valves
Pregnant women with mechanical prosthetic heart valves are automatically classified as WHO risk category III.[5] This classification implies a significantly increased risk of maternal mortality or severe morbidity, necessitating expert counselling regarding the maternal and fetal risks of pregnancy. Intensive care is required for all women with mechanical prosthetic valves who plan to be pregnant despite these risks. Expert care should be a joint venture shared between obstetricians skilled in internal medicine and cardiologists. The occurrence of pregnancy in a woman with a mechanical prosthetic valve should be a red-light event leading to early referral to an appropriate level of expert care. Given the scarcity of trained cardiologists in SA, this usually implies referral to a large metropolitan area with tertiary medical facilities.
In addition to the inherent risk of having a prosthetic valve, pregnancy represents a further threat to the wellbeing of women with mechanical heart valves: firstly, there is an increased probability of valve thrombosis and, secondly, there is an increased risk of infection.
Risk of thrombosis
Pregnancy is a procoagulant state with enhanced clot formation throughout its duration. The need for this adaptation arises mostly in the choriodecidual space, where fibrin deposition is demonstrable. The enhanced clotting profile of pregnancy is based on greater circulating concentrations of clotting factors, an impeded anticlotting mechanism based on activated protein C resistance and inhibition of fibrinolysis as a result of placental production of plasminogen activator inhibitor (PAI-2). These mechanisms also increase the probability of fibrin deposition outside the placental bed, resulting in e.g. deep venous thrombosis becoming more common in pregnant than non-pregnant women. Mechanical heart valves have an inherent risk of thrombosis, which has diminished with the newer generation of valves. However, the procoagulant effects of pregnancy may increase the risk of valve thrombosis and increase the possibility of acute heart failure.
Mechanical valves require anticoagulation regardless of pregnancy. Pregnancy may alter the indications for and dose of anticoagulant drugs used according to the fetal risks arising from their use and the need to allow delivery without an enhanced possibility of iatrogenic obstetric haemorrhage caused by the administration of these drugs. The possibilities require careful counselling of the pregnant woman and her partner before any treatment is changed and careful monitoring of the anticoagulant efficacy of any drugs subsequently used, as well as a careful strategy for managing the parturient needing peripartum anticoagulation. The merits of the different drugs available are summarised below:
-
Unfractionated heparin (UFH). This must be used intravenously according to international guidelines, with studies indicating that the subcutaneous use of the drug is associated with a high failure rate.[27] The heparin should be titrated against the activated partial thromboplastin time, aiming at a ratio of 2.5 - 3.0 compared with controls. UFH does not cross the placenta and there is no possibility of the baby developing embryopathy when the drug is used in the first trimester. UFH is associated with more than double the risk of valve thrombosis compared with warfarin and a consequential increase in the maternal mortality rate.[28] However, the use of UFH obviates any possibility of fetal anomaly attributable to oral anticoagulant drugs, although the combined, sequential use of UFH followed by warfarin may still result in subsequent abortion and fetal wastage.
-
Low-molecular-weight heparin (LMWH). This drug is used subcutaneously, and when used in the first trimester rather than warfarin will avoid the risk of teratogenesis. The dose of LMWH needed to reach a therapeutic threshold is increased during pregnancy because of the physiological changes. Simultaneously, the monitoring of anti-Xa activity is imperative if LMWH is to be used.[29] Using LMWH rather than oral anticoagulants is associated with a significant increased risk of thromboembolic events, which may be as high as 1 in 10.[30]
-
Warfarin. This is the most effective anticoagulant available for the prevention of maternal thromboembolic complications. However, there is an inherent risk of treatment failure and a background maternal mortality risk of 1 in 50. The risk of adverse perinatal outcome is much higher, with perinatal wastage as high as 1 in 3. The embryopathy risk has been characterised as negligible by some guidelines, where the dose of drug used in the first trimester is <5 mg/day. Evidence in case reports indicates that this is not universally true.[31]
The maternal and fetal risk therefore varies according to the selected anticoagulant regimen, and expert counselling together with close monitoring are necessary, regardless of the drugs used. Therefore, all pregnant women with mechanical heart valves should be accorded red-light status when pregnant, with immediate referral to an appropriate level of care to choose and optimise the anticoagulant regimen.
Risk of haemorrhage
Therapeutic anticoagulation implies an increased risk of haemorrhage, especially in obstetric practice, where the possibility of life-threatening haemorrhage can and does arise. Haemorrhage is a leading direct cause for maternal mortality among SA women - a risk that is likely to increase when anticoagulants are used. Data from New Zealand indicate that both antepartum and postpartum haemorrhage are prevalent: between 1 in 5 and 1 in 7 women using LMWH for anticoagulation suffer from a haemorrhagic complication, with approximately two-thirds of these complications being drug-related.[30]
These considerations are the second reason to regard all women with prosthetic mechanical heart valves as deserving of red-light status.
Risk of sepsis
Parturition is associated with an inflammatory cytokine cascade and leucocyte infiltration of the fetal tissues.[32] It is a matter of speculation that this may represent an adaptive response to incipient infection at the time of delivery. However, more apparent is that markers of inflammation increase even further in women who have premature rupture of the membranes and those who go into preterm labour.[33] The risk of sepsis is further underscored by epidemiological studies showing the importance of sepsis, unrelated to HIV infection, as a cause of maternal mortality in SA.
These considerations must be viewed in the context of infective endocarditis that shows a cumulatively increasing incidence over time in individuals who have mechanical valves outside of pregnancy. There is therefore an inherent risk of infection in and around the mechanical valve, which is likely to increase during pregnancy because of the prevalence of bacteraemia associated with (vaginal) childbirth. The approach to preventing endocarditis owing to parturition is well established and is based on the use of routine antibiotic prophylaxis during delivery, which is now universally recommended.[34]
What has gone unrecognised, however, are the risks of endocarditis related to line sepsis. The use of long-term intravenous lines, where UFH is administered intravenously for many days in succession, results in an enhanced risk of sepsis.[35] There is published evidence that intravenous catheters are associated with positive cultures in as many as 1 in 3 cases where staphyloccoci, enterococci, streptococci and Pseudomonas comprise the majority of organisms. Anecdotal experience of those providing services to women with prosthetic valves confirms instances where line sepsis has been the direct cause of endocarditis and has led to maternal mortality.
Modifying red-light status
In patients with mechanical heart valves, their red-light status will never change. However, dealing with the red-light level of risk requires expert and targeted interventions. These include:
-
Prevention of unplanned pregnancy. This responsibility rests with all medical practitioners providing care to women with prosthetic valves. The use of anticoagulants in this group of women is of concern. This is not a barrier to effective contraception and even the combined oral contraceptive pill may be used, providing the level of anticoagulation is being monitored. Counselling regarding family size and offering permanent contraception should always be considered in the management of these women.
-
Baseline evaluation and establishing a programme of shared care between obstetricians and cardiologists are imperative. These patients should be seen frequently and should be able to access care rapidly in the event of any emergency.
-
Choosing an anticoagulant regimen should be deliberately considered with informed choice from the pregnant woman and her partner. Whatever regimen is implemented, there must be facilities for monitoring the efficacy of the drugs used (measuring international normalised ratio (INR), activated partial thromboplastin time (aPTT) or anti-Xa levels).[36,37] Therapeutic levels must be maintained, with the exception of the time spent in labour.
-
In general, warfarin or LMWH is the preferred option because of the risks of line sepsis and social isolation arising from continuous hospitalisation.[36]
-
Peripartum management should include a scheduled de-escalation of long-acting anticoagulant drugs immediately before delivery, with short-term bridging using intravenous UFH.
Obstetric procedures should be limited according to their risk of sepsis, and prophylactic antibiotics are indicated during labour. General measures considered necessary in the intrapartum care of pregnant women with heart disease are applicable and include nursing the parturient in the semi-Fowler's position, limiting the use of intravenous fluids and providing adequate analgesia during labour.
Conclusion
Cardiac disease in pregnancy is prevalent and an important cause of morbidity and mortality. Appropriate management during pregnancy requires expert assessment, risk categorisation and ongoing care, which may need to include regular follow-up in combined obstetric and cardiology clinics.
Pregnancy also opens a window of opportunity, which may allow the identification of undiagnosed subclinical cardiac disease that may then be more appropriately and continuously managed to avoid morbidity and mortality in later life.
Summary
-
All women with suspected or known cardiac disease should be risk assessed early in pregnancy by a combined obstetric and cardiology team.
-
A percutaneous balloon mitral commissurotomy should be considered as a treatment option for young women with moderate or severe mitral stenosis.
-
The diagnosis of cardiac disease should be suspected in women presenting to the labour ward or emergency unit with acute shortness of breath during pregnancy or up to 6 months post partum.
-
All pregnant women with prosthetic heart valves should be managed by a combined team consisting of a cardiologist and an obstetrician skilled in internal medicine.
Declaration. None.
Acknowledgements. None.
Author contributions. PSP: conceptualisation, review, write-up and editing; JA: review, write-up and editing; and SM: review and write-up.
Funding. None.
Conflicts of interest. None.
References
1. Lewis G, ed. Confidential Enquiry into Maternal and Child Health (CEMACH). Saving Mothers' Lives: Reviewing Maternal Deaths to Make Motherhood Safer 2003 - 2005. The Seventh Report on Confidential Enquiries into Maternal Deaths in the United Kingdom. London: CEMACH, 2007. [ Links ]
2. Knight M, Nair M, Tuffnell D, et al. MBRRACE-UK Saving Lives, Improving Mothers' Care -Surveillance of Maternal Death in the UK 2012 - 2014 and Lessons Learned to Inform Maternity Care from the UK and Ireland Confidential Enquiries into Maternal Deaths and Morbidity 2009 - 2014. Oxford: National Epidimiology Unit, University of Oxford, 2016. [ Links ]
3. Department of Health. Saving Mothers 2011 - 2013: Sixth Report on the Confidential Enquiries into Maternal Deaths in South Africa. Pretoria: DoH, 2014. [ Links ]
4. Department of Health. Saving Mothers 2014 - 2016: Seventh Report on the Confidential Enquiries into Maternal Deaths in South Africa. Pretoria: DoH, 2017. [ Links ]
5. Regitz-Zagrosek V, Lundqvist CB, Borghi C, et al. ESC guidelines on the management of cardiovascular disease in pregnancy. Eur Heart J 2011;32(24):3147-3197. https://doi.org/10.1093/eurheartj/ehr218 [ Links ]
6. Thorne S, MacGregor A, Nelson-Piercy C. Risks of contraception and pregnancy in heart disease. Heart 2006;92(10):1520-1525. https://doi.org/10.1136/hrt.2006.095240 [ Links ]
7. Soma-Pillay P, Seabe J, Sliwa K. The importance of cardiovascular pathology contributing to maternal death: Confidential Enquiry into Maternal Deaths in South Africa, 2011 - 2013. Cardiovasc J Afr 2016;27(2):60-65. https://doi.org/10.5830/CVJA-2016-008 [ Links ]
8. Zühlke L, Engel ME, Karthikeyan G, et al. Characteristics, complications and gaps in evidence-based interventions in rheumatic heart disease: The Global Rheumatic Heart Disease Registry (the REMEDY study). Eur Heart J 2015;36(18):1115a-1122a. https://doi.org/10.1093/eurheartj/ehu449 [ Links ]
9. Watkins DA, Sebitloane M, Engel ME, Mayosi BM. The burden of antenatal heart disease in South Africa: A systematic review. BMC Cardiovasc Disord 2012;12:23. https://doi.org/10.1186/1471-2261-12-23 [ Links ]
10. Silversides CK, Colman JM, Sermer M, et al. Cardiac risk in pregnant women with rheumatic mitral stenosis. Am J Cardiol 2003;91(11):1382-1385. https://doi.org/10.1016/S0002-9149(03)00339-4 [ Links ]
11. Hameed A, Karaalp IS, Tummala PP, et al. The effect of valvular disease on maternal and fetal outcome of pregnancy. J Am Coll Cardiol 2001;37(3):893-899. [ Links ]
12. Lesnaik-Sobelga A, Tracz W, KostKiewicz M, et al. Clinical and echocardiographic assessment of pregnant women with valvular heart diseases - maternal and fetal outcome. Int J Cardiol 2004;94(1):15-23. https://doi.org/10.1016/j.ijcard.2003.03.017 [ Links ]
13. Bhatla N, Lal S, Behera G, et al. Cardiac disease in pregnancy. Int J Gynaecol Obstet 2003;82(2):153-159. https://doi.org/10.1016/S0020-7292(03)00159-0 [ Links ]
14. Van Hagen IM, Thorne S, Taha N, et al. Pregnancy outcomes in women with rheumatic mitral valve disease: Results from the Registry of Pregnancy and Cardiac Disease. Circulation 2018;137(8):806-816. https://doi.org/10.1161/CIRCULATIONAHA.117.032561 [ Links ]
15. Silversides CK, Colman JM, Sermer M, Siu SC. Cardiac risk in pregnant women with rheumatic mitral stenosis. Am J Cardiol 2003;91(11):1382-1385. https://doi.org/10.1016/S0002-9149(03)00339-4 [ Links ]
16. Rezk M, Gamal A. Maternal and fetal outcome in rheumatic heart disease: A 3-year observational study. Arch Gynelcol Obstet 2016;294:273-278. https://doi.org/10.1007/s00404-015-3990-9 [ Links ]
17. Remenyi B, ElGuindy A, Smith SC Jr, Yacoub M, Holmes DR Jr. Valvular aspects of rheumatic heart disease. Lancet 2016;387(10025):1335-1346. https://doi.org/10.1016/S0140-6736(16)00547-X [ Links ]
18. Silversides CK, Colman JM, Sermer M, et al. Early and immediate-term outcome of pregnancy with congenital aortic stenosis. Am J Cardiol 2003;91(11):1386-1389. [ Links ]
19. Kimbally-Kaky G, Gombet T, Voumbo Y, et al. Rheumatic heart disease in schoolchildren in Brazzaville. Med Trop (Mars) 2008;68(6):603-605. [ Links ]
20. Marijon E, Ou P, Celermajer DS, et al. Prevalence of rheumatic heart disease detected by echocardiography screening. N Engl J Med 2007;357(5):470-476. https://doi.org/10.1056/NEJMoa065085 [ Links ]
21. Sadiq M, Islam K, Abid R, et al. Prevalence of rheumatic heart disease in school children of urban Lahore. Heart 2009;95(5):353-357. https://doi.org/10.1136/hrt.2008.143982 [ Links ]
22. Diao M, Kane A, Ndiaye MB, et al. Pregnancy in women with heart disease in sub-Saharan Africa. Arch Cardiov Dis 2011;104(6-7):370-374. https://doi.org/10.1016/j.acvd.2011.04.001 [ Links ]
23. Sliwa K, Hilfiker-Kleiner D, Petrie MC, et al. Current state of knowledge on aetiology, diagnosis, management and therapy of peripartum cardiomyopathy: A position statement from the Heart Failure Association of the European Society of Cardiology Working Group on Peripartum Cardiomyopathy. Eur Heart Fail 2010;12(8):767-778. https://doi.org/10.1093/eurjhf/hfq120 [ Links ]
24. Hilfiker-Kleiner D, Sliwa K. Pathophysiology and epidemiology of peripartum cardiomyopathy. Nat Rev Cardiol 2014;11(6):364-370. https://doi.org/10.1038/nrcardio.2014.37 [ Links ]
25. Department of Health. Saving Mothers 2008 - 2010: Fifth Report on the Confidential Enquiries into Maternal Deaths in South Africa. Pretoria: DoH, 2012. [ Links ]
26. Sliwa K, Pterie MC, Hilfiker-Kleiner D, et al. Long-term prognosis, subsequent pregnancy, contraception and overall management of peripartum cardiomyopathy: Practical guidance paper from the Heart Failure Association of the European Society of Cardiology Study Group on Peripartum Cardiomyopathy. Eur J Heart Fail 2018;20(6):951-962. https://doi.org/10.1002/ejhf.1178 [ Links ]
27. Salazar E, Izaguiurre R, Verdejo J, Mutchinick O. Failure of adjusted doses of subcutaneous heparin to prevent thromboembolic phenomena in pregnant patients with mechanical cardiac valve prostheses. J Am Coll Cardiol 1996;27(7):1698-1703. [ Links ]
28. Chan WS, Anand S, Ginsberg JS. Anticoagulation of pregnant women with mechanical heart valves. A systematic review of the literature. Arch Intern Med 2000;160(2):191-196. https://doi.org/10.1001/archinte.160.2.191 [ Links ]
29. Quinn J, von Klemperer K, Brooks R, Peebles D, Walker F, Cohen H. Use of high intensity adjusted dose low molecular weight heparin in women with mechanical heart valves during pregnancy: A single centre experience. Haematologica 2009;94(11):1608-1612. https://doi.org/10.3324/haematol.2008.002840 [ Links ]
30. McClintock C, McCowan LME, North R. Maternal complications and pregnancy outcome in women with mechanical prosthetic heart valves treated with enoxaparin. Obstet Gynecol Surv 2010;65(2):82-84. https://doi.org/10.1097/01.ogx.0000368140.16599.56 [ Links ]
31. Basu S, Aggarwal P, Kakani N, Kumar A. Low dose maternal warfarin intake resulting in fetal warfarin syndrome: In search for a safe anticoagulant regimen during pregnancy. Birth Defect Res 2016;106(2):142-147. https://doi.org/10.1002/bdra.23435 [ Links ]
32. Keelan JA, Blumenstein RJA, Helliwell TA, et al Cytokines, prostaglandins and parturition - a review Placenta 2003;24(Suppl A):S33-S46. https://doi.org/10.1053/plac.2002.0948 [ Links ]
33. Romero R, Espinoza J, Goncalves LF, et al. Inflammation in preterm and term labour and delivery. Semin Fetal Neonat Med 2006;11(5):317-326. https://dolorg/10.1016/j.siny.2006.05.001 [ Links ]
34. Tower C, Nallapeta S, Vause S. Prophylaxis against infective endocarditis in obstetrics: New NICE guidance. Br J Obstet Gynaecol 2008;115(3):1601-1604. https://doi.org/10.1111/j.1471-0528.2008.01938.x [ Links ]
35. Paragioudaki M, Stamouli F, Kolonitsiou ED, et al. Intravenous catheter infections associated with bacteraemia: A 2-year study in a university hospital. Clin Microbiol Infect 2004;10:431-435. https://doi.org/10.1111/j.1469-0691.2004.00851.x [ Links ]
36. Nishimura RA, Otto CM, Sorajja P, et al 2014 AHA/ACC guideline for the management of patients with valvular heart disease. J Am Coll Cardiol 2014;63(22):2438-2488. https://doi.org/10.1016/j.jacc.2014.02.537 [ Links ]
37. Vause S, Clarke B, Tower CL, et al. Pregnancy outcomes in women with mechanical prosthetic heart valves: A prospective descriptive population based study using the United Kingdom Obstetric Surveillance System (UKOSS) data collection system. Br J Obstset Gynaecol 2017;214(9):1411-1419. https://doi.org/10.1111/1471-0528.14478 [ Links ]
 Correspondence:
Correspondence:
P Soma-Pillay
priya.somapillay@up.ac.za
Accepted 4 May 2018


{kind=link}
{kind=link}