










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSAMJ: South African Medical Journal
versão On-line ISSN 2078-5135
versão impressa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.108 no.10 Pretoria Out. 2018
http://dx.doi.org/10.7196/samj.2018.v108i10.13002
RESEARCH
Can routine inpatient mortality data improve HIV mortality estimates? Inpatient mortality at an urban hospital in South Africa
L C LongI, II, III, IV; D H EvansV, VI, VII; S RosenVIII, IX, X; C SaulsXI, XII; A T BrennanI, III, IV; I M SanneXIII, XIV, XV, XVI; M P FoxXVII, XVIII, XIX, XX
IPhD; Department of Internal Medicine, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IIPhD; School of Public Health, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IIIPhD; Health Economics and Epidemiology Research Office, Wits Health Consortium, Johannesburg, South Africa
IVPhD; Department of Global Health, School of Public Health, Boston University, USA
VDTech; Department of Internal Medicine, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
VIDTech; School of Public Health, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
VIIDTech; Health Economics and Epidemiology Research Office, Wits Health Consortium, Johannesburg, South Africa
VIIIMPA; Department of Internal Medicine, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IXMPA; Health Economics and Epidemiology Research Office, Wits Health Consortium, Johannesburg, South Africa
XMPA; Department of Global Health, School of Public Health, Boston University, USA
XIMPH; Department of Internal Medicine, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
XIIMPH; Health Economics and Epidemiology Research Office, Wits Health Consortium, Johannesburg, South Africa
XIIIMB BCh, FCP, FRCP; Department of Internal Medicine, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
XIVMB BCh, FCP, FRCP; School of Public Health, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
XVMB BCh, FCP, FRCP; Health Economics and Epidemiology Research Office, Wits Health Consortium, Johannesburg, South Africa
XVIMB BCh, FCP, FRCP; Department of Global Health, School of Public Health, Boston University, USA
XVIIDSc; Department of Internal Medicine, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
XVIIIDSc; Health Economics and Epidemiology Research Office, Wits Health Consortium, Johannesburg, South Africa
XIXDSc; Department of Global Health, School of Public Health, Boston University, USA
XXDSc; Department of Epidemiology, School of Public Health, Boston University, USA
ABSTRACT
BACKGROUND. South Africa (SA) has one of the world's largest HIV treatment programmes, to which a dramatic increase in life expectancy has been attributed. However, there continue to be concerns regarding the reporting of HIV-related mortality in SA, which varies by source. As accurate HIV mortality estimates are key to measuring the success of the national programme as well as identifying areas for improvement, we propose a complementary approach to monitoring changes in HIV-related mortality using routine inpatient records to examine trends in causes of death and HIV status over time.
OBJECTIVES. To investigate the feasibility of this approach by calculating mortality due to natural causes in the medical ward of a hospital during 2010 by HIV status.
METHODS. We conducted a cross-sectional study of inpatient mortality at a regional hospital in Johannesburg, SA, analysing all deaths due to natural causes among adult medical ward inpatients. Cause of death was recorded from the mortuary register. HIV status was ascertained directly from the mortuary register or from laboratory tests specific for HIV diagnosis or monitoring.
RESULTS. Of 1 167 inpatients who died, the majority were HIV-positive (58%). HIV positivity among males (55%) was slightly lower than that among females (61%), and HIV-positive patients were younger (median 40 years) than those who were HIV-negative (56 years) and of unknown HIV status (68 years). 'Infections and parasites' was the most common cause of natural death (29%). On average, HIV-positive patients were admitted for slightly longer (mean 10.5 days) than HIV-negative patients (9.6 days) and those of unknown HIV status (8.9 days), yet HIV-positive inpatient deaths accounted for the majority (62%) of the total bed days.
CONCLUSIONS. Even with widespread access to antiretroviral therapy, the majority of inpatient natural deaths at a large public sector hospital in 2010 were of HIV-positive patients and were probably related to HIV. In view of the importance of accurate data on causes of death, both for the HIV programme and to track other diseases, large-scale expansion of this approach over a longer period should be considered.
South Africa (SA) has a large generalised HIV epidemic, with >6 million HIV-positive citizens and one of the world's largest HIV treatment programmes, with ~3.9 million patients on treatment at the end of 2016.[1] Key indicators used to measure the success of this programme include an increase in life expectancy and a reduction in HIV-related mortality for patients on antiretroviral therapy (ART). SA has reported a steadily increasing life expectancy since 2006, and this has largely been attributed to the success of the national HIV programme.[2,3] HIV-related mortality is more difficult to measure, and as a result it has been difficult to accurately estimate and attribute the impact of the HIV programme on this indicator.
Mortality reporting in SA is managed by the Department of Home Affairs and governed by the Births and Deaths Registration Act 1992 (Act No. 51 of 1992).[4] In 2013, Statistics South Africa (Stats SA) reported that 90% of all deaths were due to natural causes.[5] In 2011, they reported the percentage of mortality attributable to HIV to be 3.4% (17 338/514 486), and they showed this percentage to increase between 2011 and 2013.[5] This is in contrast to the results of the Thembisa model, an integrated demographic and epidemiological model of the SA HIV/AIDS epidemic, which shows a decreasing percentage of deaths attributable to AIDS since 2005 with the introduction of antiretroviral treatment.[6] Thembisa estimates that in 2011 there were 169 000 AIDS deaths, which would put the percentage of mortality attributable to HIV at almost 10 times that estimated in the Stats SA report (169 000/514 486 = 32%).[5,6] Bradshaw et al.[7]estimated that fewer than 10% (20 012/207 685) of deaths due to HIV/AIDS in 2010 were registered with HIV as the primary cause of death, which supports the discrepancy between the results of Stats SA and modelled estimates. The inconsistency between Deaths Registry data as reported by Stats SA, modelling estimates of HIV-attributable mortality and analyses of the registration data suggests that other sources of information are needed to understand the role of HIV in mortality as ART access expands.[8]
Data on the contribution of HIV to total mortality from sources other than the Deaths Registry are scarce. The majority of mortality with a known place of death occurs in hospitals. In 2010 and 2013, 52% and 57%, respectively, of mortality with a known place of death occurred in hospitals.[5,9] A complementary approach to monitoring changes in HIV-related mortality may be to use the relatively detailed information available from inpatient care records to examine trends in causes of death and HIV status over time.
Objectives
To investigate the feasibility of this approach by estimating mortality due to natural causes by HIV status in the medical ward of a large urban public sector hospital during 2010 using routine data.
Methods
Study population and data
We conducted a retrospective, cross-sectional study of inpatient mortality at a regional Gauteng Province Department of Health hospital in Johannesburg, SA. The hospital serves an urban population of both formal and informal settlements and has 11 inpatient medical wards with 347 beds.
The study population included all adult (>18 years old) deaths due to natural causes (attributed to illness or an internal malfunction of the body) among patients admitted to a medical ward between 1 January and 31 August 2010, an 8-month period intended to capture seasonal variation. Deaths from other (non-natural) causes (e.g. motor vehicle accident) or that occurred during admission to specialist wards (e.g. casualty, surgery) were excluded. Inpatient deaths that were missing the data required to determine study eligibility, such as date of admission, were excluded. Deaths of pregnant women were also excluded because pregnant women requiring admission were routinely referred to another hospital.
Cause of death and HIV status
All persons who die in hospital are taken to the hospital mortuary, where the details of death are recorded in the mortuary register. This register includes date of death, gender, age, date of admission, hospital ward and primary cause of death. In some instances, additional information about comorbid conditions potentially related to the cause of death is also recorded. SA classifies and codes deaths according to the 10th revision of the International Statistical Classification of Diseases and Related Health Problems (ICD-10).[9,10] We assigned a three-character ICD-10 code to each primary cause of death as recorded in the mortuary register. The study team did not have access to death certificates and could not distinguish between the immediate and underlying cause of death. If HIV was not included as part of the cause of death, then the cause of death was not attributed to HIV. If the cause of death was classified as code R00 - R99 ('Symptoms, signs and abnormal clinical and laboratory findings not elsewhere classified'), other comorbid conditions were examined and if available coded as the primary cause of death. Patients whose final primary cause of death is classified as signs or symptoms (R00 - R99), heart failure, unspecified renal failure or malignant neoplasms of ill-defined sites are often not reported on individually and are classified as 'ill-defined' causes of death. We included these deaths and reported these codes to allow for full comparison with other publications.
HIV status was determined independently of the listed cause of death and comorbid conditions. Patients were classified as HIVpositive if positive HIV status was noted in the mortuary register or if laboratory test results specific for HIV diagnosis or monitoring (e.g. HIV test, CD4+ count or viral load test) could be retrieved from National Health Laboratory Service records. Patients were classified as HIV-negative if a negative HIV test was recorded in the mortuary register or laboratory record (during the current admission or in the month prior to admission). Patients for whom HIV status could not be determined definitively (i.e. no positive HIV test, no HIV monitoring tests, and no negative HIV test during the admission or within the month prior to admission) were classified as having unknown HIV status.
Ethics approval
The study protocol was reviewed by the institutional review boards of the University of the Witwatersrand and Boston University, which approved the collection of the data without informed consent and the use of an anonymous analytical dataset (ref. nos M101011 and H-30029).
Results
Baseline description
Baseline characteristics of the study population are presented in Table 1. Over the 8-month period, 1 201 natural inpatient deaths met the study inclusion criteria. Of these, 34 had a missing admission date and were excluded. The final analytical cohort included 1 167 inpatient deaths, an average of 145 deaths per month. The majority of inpatients who died were HIV-positive (n=682, 58%), in less than a third HIV status was unknown (n=343, 29%), and just over a tenth were confirmed HIV-negative (n=142, 12%).
There were similar numbers of males and females in the sample, but the rate of HIV positivity among males (55%, 331/595) was slightly lower than that among females (61%, 350/571), which reflects what is seen in the general population. The median age of the cohort was 46 years (interquartile range (IQR) 36 - 62), with HIV-positive patients younger (40 years, IQR 33 - 48) than those who were HIV-negative (56 years, IQR 46 - 64) and of unknown HIV status (68 years, IQR 53 - 79).
Fig. 1 plots inpatient mortality by age group. Mortality occurred at much younger ages in HIV-positive patients than in those of negative or unknown status. The percentage of subjects with confirmed HIV status (HIV-positive + HIV-negative/Total patients) fell rapidly by age group, with 89% of 18 - 49-year-olds having a confirmed status v. only 24% of those aged >65; in other words, patients of unknown HIV status were older. Similarly, known HIV positivity (confirmed HIV-positive/Total patients) in the cohort fell from 82% among 18 -49-year-olds to 10% among those aged >65 years.

Patients who have compromised immune systems (such as those with HIV and the elderly) may be more likely to be admitted and die during months when infectious diseases such as influenza are more prevalent. To explore this, mortality is plotted by calendar month of death and HIV status in Fig. 2. The peak of the annual severe acute respiratory illness (influenza) infections in 2010 occurred in July and August,[11] coincident with the peak of mortality in the group with unknown HIV status (elderly). Mortality due to influenza, acute lower respiratory infections and chronic respiratory infections showed raised rates during the months of July and August (data not presented). In contrast, mortality in the HIV-negative and HIVpositive groups showed no clear seasonal patterns.

Description of causes of death
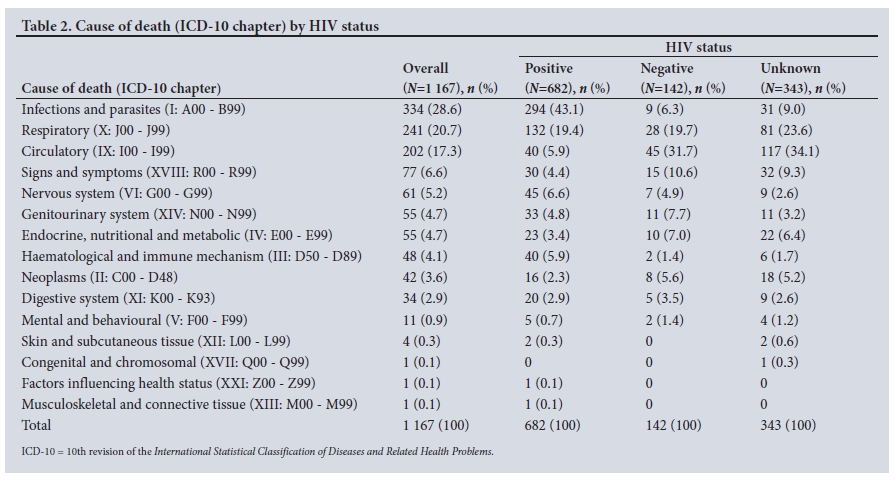
Table 2 describes the major causes of death using ICD-10 code chapters by HIV status. 'Infections and parasites' was the most common natural cause of death (29%), followed by 'Respiratory' (21%) and 'Circulatory' (17%) conditions. HIV-positive patients accounted for nearly 9 out of every 10 deaths related to 'Infections and parasites' (294/334), despite comprising just 58% of all deaths.
Despite 'Infections and parasites' accounting for 43% of deaths among HIV-positive patients, only one patient had HIV listed as the primary cause of death. The most common infectious disease across all groups was 'Tuberculosis' (A15 - A19), responsible for 19% of deaths overall (n=224) and nearly a third (n=204, 30%) of deaths among HIV-positive patients. 'Other heart disease' (I30 - I52), in contrast, was the leading cause of death among HIV-negative patients (n=25, 18%) and those of unknown HIV status (n=68, 20%). Further details on the most common specific causes of death by broad age group are reported in Table 3.
In Fig. 3, distribution of mortality by major cause is illustrated across age groups, revealing a distinct pattern of mortality by age and cause, which would be expected in a population with a high HIV prevalence. Infectious diseases follow the same mortality profile as that of the HIV-positive group shown in Fig. 1, with the peak in the mortality in the younger age groups. Bradshaw et al.[7]dubbed this type of characteristic age-specific mortality profile the 'AIDS signature'. Diseases of the circulatory system, which are not directly related to HIV, show steadily increasing mortality with increasing age. Respiratory disease appears more evenly spread among HIVpositives, HIV-negatives and those with unknown HIV status (Fig. 3).

Bed days
On average, patients in the sample were admitted for 9.9 days prior to death. HIV-positive patients were admitted for slightly longer (mean 10.5 days, 95% confidence interval (CI) 9.8 - 11.3 days) than HIV-negative patients (9.6 days, 95% CI 8.1 - 11.1) and those of unknown HIV status (8.9 days, 95% CI 8.1 - 9.6). However, because HIV-positive inpatient deaths were more common, they accounted for the majority (62%) of the bed days (a proxy for resource usage) associated with inpatient deaths (Total HIV-positive bed days/Total bed days), compared with HIV-negative and HIV status unknown inpatient deaths (12% and 26%, respectively).
Discussion
In 2010, SA's national ART programme was 5 years old, and >1.2 million people were estimated to be on ART. This equated to ART coverage of >60% at the prevailing eligibility threshold of a CD4+ count <200 cells/uL.[12] Despite relatively high levels of access to care, however, the results of this study suggest that HIV-positive inpatient medical mortality remained high in 2010, with an HIV positivity of at least 58% among all natural inpatient deaths and at least 82% among natural deaths between the ages of 18 and 49 years.
The role of HIV in inpatient mortality in 2010 can be compared with results of a similar study (W D F Venter, unpublished data, 2004) at the same site covering the years just preceding the national rollout of ART in SA (2000 - 2003). That study examined all 2 138 inpatient deaths occurring over 3 months of each year over a 4-year period. A large majority (94%) were deaths due to natural causes, and most (75%) were from the medical wards, making them comparable to the sample in our study. The numbers of deaths per month and the gender and age distribution were similar between the two studies. The proportion of patients known to be HIV-positive more than doubled from 20% in 2000 - 2003 to 58% in 2010. This is probably due in part to poor ascertainment of HIV status before 2004, but the large increase in HIV-positives could also suggest a real increase in the proportion of HIVpositive deaths over this time period.
Stats SA reported that there were 28 660 natural deaths in the City of Johannesburg Metropolitan Municipality in 2010.[9] Our sample of 1 167 therefore covers 4% (1 167/ 28 660) of the natural deaths in Johannesburg that year.[9] The Stats SA report also notes that in Gauteng Province, where Johannesburg is located, 'HIV disease' (ICD-10 B20 - B24) was the seventh leading cause of natural death, accounting for 3.4% of all natural deaths. This is equivalent to only 15% of the 21 548 deaths classified as 'Infections and parasites (A00 - B99)'.[5] Our study, in contrast, found that 88% of all deaths classified as 'Infections and parasites' were among HIV-positive patients. If we conservatively assume that only those HIV-positive deaths classified as 'Infections and parasites' can be directly attributed to HIV (i.e. we assume that 56% of deaths among HIV-positive patients are not caused by HIV), then 25% of all natural deaths in our study would be directly attributable to HIV, a seven-fold increase over the Stats SA estimate for the province. While deaths due to HIV may be over-represented in hospital admissions compared with the population at large, the largest contributor to this difference is likely to be under-reporting of HIV as a cause of death, even when the HIV status of patients is known.
Stats SA reported that in 2010 44% of all deaths occurred in hospitals, which translates into ~91 381 AIDS deaths in hospitals.[7,9] The mean length of stay associated with an inpatient-related HIV-positive death was 10.5 days in our cohort, so these deaths could equate to ~959 500 bed days. While it is impossible to remove inpatient AIDS deaths completely, it is reasonable to assume that HIV-related inpatient mortality can be reduced substantially with earlier ART initiation and better treatment adherence, which would lessen what is currently a significant burden on the hospital system.
Study limitations
Our study had several limitations. As noted above, the mortality reported here accounts for only 4% of natural-cause mortality in the City of Johannesburg Metropolitan Municipality in 2010. When compared with national mortality statistics, however, the distribution by major causes of death is similar, which suggests that the findings have relevance beyond a single site. Of more concern is that only 70% of the sample had verified HIV status, and older patients were more likely to be of unknown HIV status. The mortality associated with HIVpositive inpatients here should therefore be regarded as a lower boundary on true HIV-positive mortality, as it is likely that at least a few patients of unknown status were in fact HIV-positive. Finally, as noted in the 'Methods' section, ICD-10 codes were assigned based on the cause of death as recorded in the mortuary register. This did not allow for the distinction to be made between the underlying and immediate cause of death, and it is possible that patients may have been assigned the wrong cause of death.
Conclusions
We found that even with widespread access to ART, the majority of inpatient natural deaths at a large public sector hospital in 2010 were among HIV-positive patients and were probably related to HIV. Our results provide support to the contention that HIV-related mortality is dramatically under-reported[7,8] in national statistics. A solution to this problem may be the introduction of an electronic mortuary register that would allow for rapid, real-time identification of any trends observed in the mortality of patients, both HIV-positive and HIV-negative. In view of the importance of accurate data on causes of death, both for HIV interventions and to track other diseases, research on this or other solutions is needed.
Acknowledgements. The authors express their gratitude to the management and staff of the study site for providing permission to conduct the study as well as the care that they provided to the patients included in the study. The authors' views expressed in this publication do not necessarily reflect the views of the United States Agency for International Development or the US government.
Author contributions. LCL was the principal investigator and was primarily responsible for designing and co-ordinating the study, preparing and cleaning the analytical dataset and analysing the data. MPF, DHE and AB provided assistance with statistical analysis and supervision. CS assisted with co-ordinating field study activities, data collection and data cleaning. SBR contributed to the original design of the study, provided assistance with the interpretation of the results and provided supervision. IMS provided supervision and support on the clinical aspects of the analysis. LCL did the analysis and prepared the first draft of the manuscript. All authors reviewed and approved the final draft of the manuscript.
Funding. LCL, MPF, CS, DHE, AB and SBR were funded for this work by the United States Agency for International Development (USAID) through the following agreements: 674-A-00-09-00018-00 and 674-A-12-00029. IMS was funded for this work by USAID through the following agreement: 674-A-12-00029.
Conflicts of interest. None.
References
1. Joint United Nations Programme on HIV/AIDS (UNAIDS). UNAIDS Data 2017. 2017. http://www.unaids.org/en/resources/documents/2017/2017_data_l (accessed 22 March 2018). [ Links ]
2. Statistics South Africa. Mid-year population estimates 2014. Statistical Release P0302. Pretoria: Stats SA, 2014. https://www.statssa.gov.za/publications/P0302/P03022014.pdf (accessed 21 November 2017). [ Links ]
3. Bor J, Herbst AJ, Newell ML, Barnighausen T. Increases in adult life expectancy in rural South Africa: Valuing the scale-up of HIV treatment. Science 2013;339(6122):961-965. https://doi.org/10.1126/science.1230413 [ Links ]
4. South Africa. Births and Deaths Registration Act No. 51 of 1992. Government Gazette 1992;323 (No. 13953). [ Links ]
5. Statistics South Africa. Mortality and causes of death in South Africa, 2013. Statistical release P0309.3 Pretoria: Stats SA, 2014. http://www.statssa.gov.za/publications/P03093/P030932013.pdf (accessed 20 October 2017). [ Links ]
6. Johnson L. Thembisa version 1.0: A model for evaluating the impact of HIV/AIDS in South Africa. Centre for Infectious Disease Epidemiology and Research Working Paper. 2014. https://www.thembisa.org/publications (accessed 20 October 2017). [ Links ]
7. Bradshaw D, Msemburi W, Dorrington R, et al. HIV/AIDS in South Africa: How many people died from the disease between 1997 and 2010? AIDS 2015;30(5):771-778. https://doi.org/10.1097/QAD.0000000000000947 [ Links ]
8. Skingsley A, Takuva S, Brown A, Delpech V, Puren A. Monitoring HIV-related Mortality in South Africa: The Challenges and Urgency. Report No. 4. Johannesburg: National Health Laboratory Service, National Institute for Communicable Diseases, November 2014. [ Links ]
9. Statistics South Africa. Mortality and causes of death in South Africa, 2010. Statistical release P0309.3. Pretoria: Stats SA, 2013. http://www.statssa.gov.za/publications/P03093/P030932010.pdf (accessed 20 October 2017). [ Links ]
10. World Health Organization. International Statistical Classification of Diseases and Related Health Problems. 4th ed. Geneva: World Health Organization, 2010. [ Links ]
11. National Institute for Communicable Diseases. Severe Acute Respiratory Illness (SARI) Surveillance: Influenza Report 04/01/201 - 28/01/2011. National Institute for Communicable Diseases, 2011. http://www.nicd.ac.za/assets/files/Infiuenza%20Report_pdf%20end%20Jan%202011.pdf (accessed 20 October 2017). [ Links ]
12. Johnson LF. Access to antiretroviral treatment in South Africa, 2004 - 2011. South Afr J HIV Med 2012;13(1):22-27. https://doi.org/10.4102/sajhivmed.v13i1.156 [ Links ]
 Correspondence:
Correspondence:
L C Long
lclong@bu.edu
Accepted 13 April 2018


{kind=link}
{kind=link}
{kind=link}