










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.108 n.8 suppl.1 Pretoria Aug. 2018
http://dx.doi.org/10.7196/samj.2018.v108i8.13499
RESEARCH
Hepatocellular carcinoma: Epidemiology, pathogenesis and surveillance - implications for sub-Saharan Africa
K ZakhariaI, II, III; C A LutherIV; H AlsabbakI; L R RobertsV
IMD; Internal Medicine Residency Program, Department of Medical Education, Beaumont Health, Dearborn, Michigan, USA
IIMD; Division of Gastroenterology, University of Michigan, Ann Arbor, Michigan, USA
IIIMD; Division of Gastroenterology and Hepatology, Mayo Clinic, Rochester, Minnesota, USA
IVMD; Department of Dermatology, Henry Ford Health System, Detroit, Michigan, USA
VMB ChB, PhD; Division of Gastroenterology and Hepatology, Mayo Clinic, Rochester, Minnesota, USA
ABSTRACT
Hepatocellular carcinoma (HCC) originates from hepatocytes usually secondary to chronic inflammation and cirrhosis. It is an important disease of global significance with a high incidence and mortality. It is the fifth and eighth most common cancer in males and females, respectively. HCC is also extremely lethal; in 2015 it was the second and sixth most common cause of death from cancer in males and females, respectively. Chronic viral hepatitis B and C are the most frequent risk factors for the development of HCC, and the global distribution of HCC largely mirrors that of chronic viral hepatitis. More recently, there has been a notable increase in the incidence of HCC as a result of obesity-related fatty liver disease. Here, we review the epidemiology of HCC, examine recent advances in our understanding of the pathogenesis of HCC, discuss the implications for identification of potential therapeutic targets, and provide the most updated recommendations on surveillance for HCC, with particular attention to the unique challenges and potential opportunities to reduce the burden of illness and death from HCC in sub-Saharan Africa.
Hepatocellular carcinoma (HCC) is a cancer of global significance owing to its high incidence and extremely high mortality. It is the sixth most common cancer worldwide, with 854 000 new cases estimated to occur in 2015. Moreover, because of its high mortality, HCC is estimated to be the second, third or fourth most common cause of cancer deaths, causing ~810 000 deaths in 2015.1 Since most HCCs occur in countries in Asia and Africa that do not have population-based cancer registries, it is estimated that there may be as much as a 40% undercount of HCC cases in these regions, resulting in a 20% underestimation of HCC incidence and mortality globally.2 In addition to the lack of registries in sub-Saharan Africa (SSA) countries, this underestimation is at least partially due to a general lack of appreciation of the high burden of disease and death from chronic viral hepatitis, resulting in a lack of population screening for viral hepatitis, lack of implementation of HCC surveillance in at-risk individuals, and lack of access to diagnostic imaging modalities and healthcare providers trained in HCC treatment, including hepatologists, interventional radiologists, and hepatobiliary surgeons.3 HCC usually develops in the setting of chronic inflammation of the liver induced by viruses, toxins, metabolic liver disease or autoimmunity, and cirrhosis. The most important risk factors for HCC are chronic viral hepatitis B (HBV) and C (HCV), alcohol abuse and aflatoxin B1 (AFB1) exposure.4 In middle and high income countries, obesity-related fatty liver disease is increasingly important as a cause of HCC. Due to the lack of surveillance and treatment capability in many high-incidence countries, HCC is typically diagnosed at late stages, and is thus associated with poor survival, with an estimated global mortality rate of 95%.5 In this focused review we discuss the epidemiology of HCC, its association with viral hepatitis, and its pathogenesis. We also discuss the primary and secondary prevention of HCC along with challenges to implementation of comprehensive programmes to address the HCC burden in SSA counties.
Methods
We reviewed the published data comprehensively using PubMed and Google Scholar. Keywords used include: HCC, viral hepatitis, HBV, HCV, pathogenesis, primary and secondary prevention, and challenges in Africa. The quality of the evidence is indicated in parenthesis after each recommendation.
Results
Epidemiology and association with viral hepatitis
Viral hepatitis is a leading cause of disability and mortality worldwide, with a gradual increase in the number of deaths over the last few decades. The global yearly estimate of deaths due to viral hepatitis has increased from 0.89 million in 1990 to 1.45 million in 2013, higher than the estimated number of deaths from HIV, tuberculosis, or malaria.6 Chronic viral infection is a major risk factor for HCC. Between 1990 and 2013, viral hepatitis increased from the tenth leading cause of death to the seventh leading cause of death globally.6 HBV is the most common risk factor for HCC in most countries in SSA and Asia, while HCV is the most common risk factor for HCC in North America, Europe, Japan and Egypt.7,8 Most countries in Africa have high (>8%) or higher-intermediate (5 - 7.99%) prevalence of chronic HBV infection, with the exception of Algeria, Eritrea, Madagascar and the Seychelles, which have low (<2%) to lower-intermediate (2 - 4.99%) prevalence.9 In South Africa (SA), the prevalence of chronic HBV was estimated as 6.7% of the general population. Chronic HBV occurs more commonly in black South Africans than other racioethnic population groups. This is partly because only a small percentage of babies born to black mothers receive the HBV vaccine.10 The prevalence of HBV infection also varies between regions of SA and between males and females. In older studies, HBV prevalences were estimated at 5 - 16% v. 8 - 9% in black males living in rural v. urban areas, respectively, and 4 - 12% v. 2.7 - 4% in black females living in rural v. urban areas, respectively.10 In a recent study, the prevalence of HBV infection in healthy blood donors in SA was estimated at 0.66%.11
There is substantial global variation in the prevalence of chronic HCV infection. In Africa, the prevalence of chronic HCV infection is highest in Egypt, which has anti-HCV and viraemic prevalences of 14.7% and 10.0%, respectively, rates that are higher than in almost all other countries. The high infection rates in Egypt are likely due to extensive iatrogenic transmission during national campaigns for the eradication of schistosomiasis.12 Viraemic prevalence of HCC is also high (≥2.5%) in Central and Western SSA. For example, in Nigeria, the reported adult anti-HCV antibody and viraemic prevalences were 8.4% and 6.9%, respectively.13 In Eastern and Southern SSA, viraemic prevalences are generally lower, varying between 0.75% and 1.25%. In SA and Zimbabwe, the anti-HCV prevalence was 1.7% and 1.6%, respectively, which was marginally higher than viraemic prevalence.13 In North Africa and the Middle East, HCV prevalences vary substantially, with most countries having a viraemic prevalence between 0.75% and 1.25%.13
Given the substantial global variations in prevalence of the major risk factors, the epidemiology of HCC varies between regions and countries. The highest incidences of HCC are seen in regions with high prevalences of chronic HBV and HCV. In the most recent Global Burden of Disease Study, HCC is ranked first in cancer incidence in four countries (including Mongolia and three SSA countries: the Republic of the Gambia, Guinea, and Mali) and first in cancer mortality in 30 countries (including Egypt, Djibouti, Mozambique, and 24 other countries in central and western SSA).11 In SA, HCC is ranked 14th in incidence and seventh in mortality.11
The incidence and mortality of HCC is generally higher in males than in females, with an incidence ratio of 2:1 to 6:1, depending on the region. In males, HCC is the most commonly diagnosed cancer in 10 SSA countries (Mauritania, Republic of the Gambia, Mali, Burkina Faso, Cameroon, South Sudan, Democratic Republic of the Congo, Angola, Mozambique) and the most common cause of cancer deaths in most countries of western, eastern and central SSA.11 Regionally, males in Central SSA have the third highest age-standardised incidence rate (ASIR) (per 100 000 person-years) of 24.4, after high-income Asia Pacific and East Asia, and the second highest age-standardised death rate (ASDR) (per 100 000 person-years) of 29.4 after East Asia.1 Similarly, females in Western SSA have the third highest ASIR of 10.9 after high-income Asia Pacific and East Asia, but the second highest ASDR of 10.9 after East Asia.1 Currently, the incidence of HCC is underestimated in many countries, particularly developing countries, which is partially due to decreased access to care and poor reporting of health data. In 2012, at least 120 722 cases of HCC were estimated to have been missed.21 The revised global incidence was 12.0 per 100 000, while the reported incidence was 10.1 per 100 000.21 The incidence of HCC was significantly underestimated in 78 countries, of which 34 (44%) were in Africa and included SA.21
The age at the time of HCC diagnosis also varies based on aetiology of HCC and by region. In Africa, patients with HCC present at a younger age than in other regions of the world; therefore, surveillance of Africans with chronic HBV who are at risk for HCC is recommended from the age of 20 years.2,14 In a study of a 1 552 HCC patients from 7 African countries, i.e. Nigeria, Ghana, Uganda, Malawi, Côte D'Ivoire, Sudan and Tanzania, the median age at the time of diagnosis was 42 years in patients with HBV, and 43 years in patients with co-infection (HBV and HCV), 47 years in those with HCC of unknown aetiology, and 55 years in patients with HCV.14 HBV-induced HCC was most frequently diagnosed between age 32.5 and 37.5 years, while HCV-induced HCC was mostly diagnosed between 57.5 and 62.5 years of age.14 In the same study, the age of onset of HBV-induced HCC substantially varied between the countries included in the study. The median age of onset was youngest in Malawi (35 years) and highest in Sudan (58 years), with most countries ranging between 40 and 46 years. Compared with HCC patients in other regions, Africa has the youngest mean age (years) at diagnosis (45) compared with Japan (69), Europe (63 - 65), North America (62), Korea (57) and China (55 - 59), which results in the greatest number of years of potential life lost.14-18 In a recently published US population-based study, country of birth (rather than race or ethnicity) had the largest impact on the age of diagnosis of HCC in the US population. The highest percentages of patients diagnosed with early onset HCC (younger than 50 years) were observed in patients born in West Africa (57%) followed by patients born in Oceania (24%) compared with 10 - 15% and <5% of patients born in Asia and Europe, respectively.18 Birth in West, Central East or Southern Africa, or Oceania had the strongest associations with very early onset of HCC (age at the diagnosis younger than 40 years) and early onset of HCC.18 On the other hand, birth in Japan, Canada, or Europe had the strongest inverse associations with early-onset HCC.18
The underlying reasons for the young onset of HBV-induced HCC in Africa are incompletely understood. Potential causes of bias such as the younger population age distribution in Africa appear not to account entirely for the observed phenomenon. Data from Asia suggests that particular HBV genotypes and sub-genotypes are associated with increased viral replication, which in turn is associated with an increased risk of HCC. However, HBV-induced HCC in Africa is associated with different HBV genotypes and appears to occur in individuals with relatively low viral loads. The extent of the contribution of dietary Aflatoxin B1 exposure to the younger onset of HCC in Africa is also not clear.
Increasingly, non-alcoholic fatty liver disease (NAFLD) is recognised as an important contributor to liver carcinogenesis. While this is now most fully appreciated in North America, where fatty liver disease and the metabolic syndrome are now the largest single contributor to the burden of HCC, it is unclear how NAFLD may interact with HBV or HCV in determining the risk of HCC in Africa.19
Survival of patients with HCC also varies between countries. In the Global HCC BRIDGE study8 of ~18 000 patients, Taiwan and Japan, the countries with established and effective national HCC surveillance programs had substantially better median overall survival of patients with HCC. Over 84 months of follow up, median survival was not reached in Taiwan and was 60 months in Japan, as compared to regions or countries with less effective programs such as North America (33 months), South Korea (31 months), Europe (24 months), and China (23 months). In comparison, a study of the survival of patients with HCC in Africa showed substantially shorter median survival periods than was shown in the BRIDGE study. Egypt had the longest median survival (10.9 months) compared to 2.5 months in a group of other African countries (Cöte D'Ivoire, Ghana, Nigeria, Cameroon, Sudan, Ethiopia, Uganda and Tanzania).20
Pathogenesis of HCC
The molecular pathogenesis of HCC varies nearly as much as the epidemiology of this devastating disease. Fortunately, continual progress in genetic and molecular analyses is yielding rapidly increasing amounts of data on the genetic and molecular alterations associated with development and progression of HCC. HCCs contain, on average, 20 - 100 mutations per genome, which is similar to the majority of solid tumours.21 It is hoped that increased understanding of the HCC genomic landscape will lead to significant advances in tumour characterisation for targeted therapies. In this section, we outline the most significant genetic and genomic aberrations.
The aetiology of HCC influences the genetic aberrations found in HCCs. HBV is a DNA virus that can induce HCC through several potential mechanisms: viral genome integration into the host genome; immune-mediated destruction and concomitant regeneration of HBV-infected hepatocytes; and the activity of HBV X (HBx) protein, a key regulatory protein in HBV replication that acts as a cofactor in the development of HCC.22 In contrast, HCV appears to induce HCC by more indirect methods, mediating inflammation and inducing recurrent cycles of cell injury, repair and regeneration that result in premature senescence and activation of a fibrogenic repair response in the liver. The inflammatory environment produces high levels of genotoxic reactive oxygen species (ROS), which cause oncogenic mutations and mutational and epigenetic inactivation of tumor suppressors, contributing to the acquisition of the minimum complement of molecular alterations needed for the malignant phenotype.23 The HCV viral core also plays a role in HCC carcinogenesis through inhibition of tumor suppressor genes, accelerating proliferative pathways, and generating ROS.24
The most significant mutations associated with hepatocellular carcinoma include mutations in the telomerase reverse transcriptase (TERT) promoter (30 - 60%), tumor protein p53 (TP53) (18 - 50%), and β-catenin (CTNNB1) (18 - 40%).25 In cirrhotic liver, while TERT mutations occur early in premalignant cells, CTNNB1 and TP53 mutations occur only in progressed HCC.26 In a normal liver, HCC can develop from hepatocellular adenomas (HCA), in which initiating CTNNB1 mutations predispose cells to malignant transformation, and TERT promotor mutations appear to occur as a second hit for full transformation.26,27 Patients with HCC due to TERT promotor mutation tend to be older males and are more likely to be HCV-positive.28 TERT, which is one of the two major components of telomerase, functions to preserve chromosome telomere length and protect the telomeres at the ends of chromosomes from fusion with neighboring chromosomes, thus protecting the cell from chromosomal damage. In HCC, mutations in the TERT promoter region result in reactivation of TERT transcription, and thus cell immortalisation. 29 The TERT region has been shown to be the most frequent site of recurrent HBV integration in the hepatocyte genome, and HBV integrations appear to substitute for TERT promoter mutations in mediating TERT reactivation.30 HBV integrations can also mediate intra-chromosomal or inter-chromosomal rearrangements. TERT mutations and CTNNB1 mutations are more frequent in alcohol associated HCC, whereas HBV-induced HCC harbors more TP53 mutations.31TERT promoter mutation frequency can also differ geographically, with mutation frequencies twice as high in African (53%) v. non-African (24%) tumours.32
Mutations associated with the tumour suppressor gene, TP53, are the second most common genetic alteration in HCC. The mutational spectrum of p53 in HCC also varies across geographical regions.33 For example, G:C to T:A transversions dominate p53 mutations in HCCs occurring in African regions and China, but are much less common in North America. CTNNB1 mutations were found at double the frequency in HCC tumours with underlying TERT mutations, in contrast to those without TERT mutations (41% v. 21%).27 Epigenetic changes are also important in HCC, as transcription of tumour suppressor genes can be inactivated by promoter hypermethylation and their mRNA levels and translation suppressed by microRNAs (miRNAs), which contributes to HCC carcinogenesis.34 For example, the p16 tumor suppressor (encoded by CDKN2A) is frequently inactivated by hypermethylation in HCC, while upregulation of miR-210, miR-221, miR-224, and miR-519d promotes HCC tumorigenesis by targeting specific genes and promoting cell cycle progression.35-37
Primary and secondary prevention of HCC
Primary and secondary prevention of HCC are particularly important in resource-limited countries, including most SSA countries, where imaging technology to identify early-stage disease and effective treatment options are both lacking. In these countries, the main focus should be on primary prevention in order to decrease risk factors such as viral hepatitis and cirrhosis, and secondary prevention through identification of patients with established risk factors and enrolling them in surveillance programmes for HCC, which are more cost effective and require more basic measures. Community and patient education by national education campaigns and through primary care providers on the most common causes of HCC, including viral hepatitis, alcohol abuse, aflatoxin exposure and metabolic syndrome, is an important strategy for primary prevention. Communities should be educated about routes of transmission and methods of protection against viral hepatitis, alcohol abuse screening and prevention, proper storage of grains and other harvested foods in hot, humid climates to prevent aflatoxin exposure, and obesity-associated liver disease. Given the strong association with viral hepatitis, prevention of new infections through applying universal precautions and avoiding unsafe medical procedures and injections,38 HBV vaccination at birth and as part of the expanded programme of immunisation, postexposure prophylaxis and appropriate treatment of existing infections play key roles in the primary prevention of HCC.
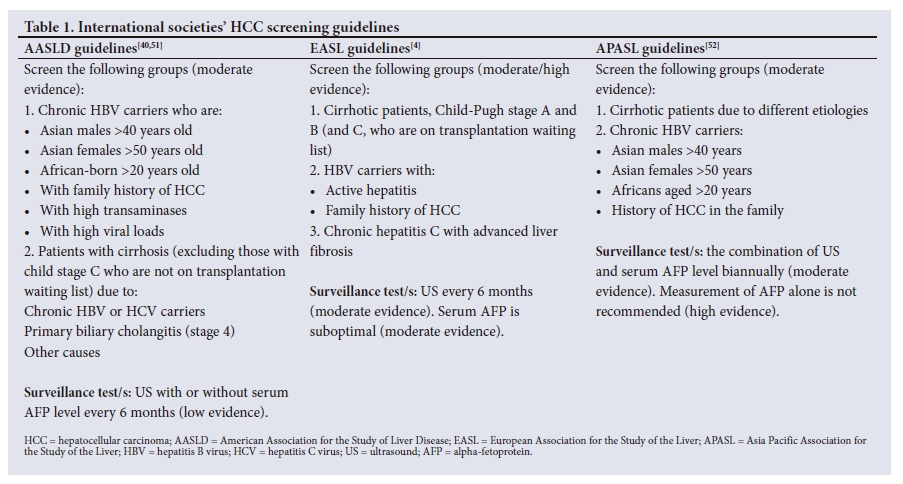
Secondary prevention or screening tests are applied in a continuous programme of ongoing surveillance to enhance detection of cancer at early stages during which treatment is more likely to be curative. The decision to enroll a patient in a surveillance programme for HCC is dependent on the estimated risk for HCC and the likelihood of benefit from therapy if HCC is discovered at an early stage. The American Association for the Study of Liver Diseases (AASLD), European Association for the Study of the Liver (EASL), and Asian Pacific Association for the Study of the Liver (APASL) guidelines consensually agree on surveillance for HCC in high risk patients (moderate/high evidence) (Table 1) using abdominal ultrasound with or without alpha fetoprotein measurement. High-risk patients include those with cirrhosis due to any aetiology (excluding those with Child-Pugh stage C who are not on a transplant waiting list given the low anticipated survival for these patients) and those with chronic viral HBV without cirrhosis if they were born in Africa or Asia and are over 20 years of age for Africans, over 40 years of age for Asian males, and over 50 years of age for Asian females. Individuals with a family history of HCC or with chronic active hepatitis are at particularly increased risk.39 Ultrasonography, the imaging modality of choice for HCC surveillance, has a variable sensitivity (65 - 80%) and a specificity of >90%. The use of alpha-fetoprotein (AFP) for HCC screening has been controversial (Table 1), given its low sensitivity for diagnosis of early-stage disease and difficulties with specificity in individuals with active liver inflammation and regeneration. However, since US is insensitive in patients with central obesity and for those with infiltrative HCCs that do not have a nodular component, there is increasing consensus that the use of AFP in addition to US is warranted. In SSA and Asia, where many patients are diagnosed with intermediate or advanced stage disease, almost all centres employ the AFP test and the World Gastroenterology Organization recommends its use for HCC surveillance.3 No formal recommendations are provided for the use of other biomarkers such as the AFP-L3% and des-gamma carboxyprothrombin (DCP), and further research is encouraged.40 The use of newer models for HCC diagnosis such as the GALAD score,41-44 which incorporates patient Gender and Age in combination with the AFP-L3%, total AFP, and DCP may facilitate HCC diagnosis if it can be provided at low cost in SSA (GALAD Score Calculator: http://www.mayoclinic.org/medical-professionals/model-end-stage-liver-disease/galad). The recommended surveillance interval is 6 months for suitable candidates.40 It has been shown that surveillance leads to earlier detection of HCC, a higher likelihood of receiving curative treatment, and improvement in survival, even when adjusted for lead time bias. Countries such as Taiwan and Japan that have established effective national HCC surveillance programs have substantially better overall survival of patients with HCC compared with countries with less effective programs such as the US, Canada, most European countries, South Korea, China and SSA countries.8
Challenges in SSA countries
Since HBV is the most common cause of HCC worldwide, a full appreciation of the current status and secular trends in rates of chronic HBV infection, the consequent development of cirrhosis, end-stage liver disease, and HCC, as well as the outcomes of these complications is important for the development of a sound global health policy. With the recent publications of WHO Guidelines for evaluation and management of chronic HBV and chronic HCV, and resolutions by the World Health Assembly promoting the global eradication of chronic HBV and HCV, chronic viral hepatitis finally appears to be attracting the attention of the global health community.45-47 However, large gaps remain, as major funders of global public health efforts still do not have robust programmes or a significant focus on eradication of chronic viral hepatitis and its sequelae.
Several limitations present in SSA countries lead to inadequate primary prevention in these countries. The majority of chronic HBV infections in Africa are due to perinatal or early childhood transmission, which can be successfully prevented by HBV vaccination within 24 hours of birth followed by two additional doses, as recommended by WHO.48 Unfortunately, most SSA countries currently use the pentavalent childhood vaccination programme recommended by the Global Alliance for Vaccines and Immunization (GAVI), which begins at 6 - 8 weeks of age, and have not implemented the HBV vaccine dose at birth. Consequently, a proportion of children who do not receive the birth dose will already be HBV-positive by the time they receive the first dose of pentavalent vaccine. The average regional three-dose HBV vaccine coverage in Africa in 2015 was 76%, with substantial variation between countries; for example, coverage was 71% in SA and 98% in Rwanda and Tanzania. Although significantly improved since year 2000, when coverage was only 5%, it remains lower than the global coverage of 84%.48 Several challenges have limited the administration of the birth dose. These include the high prevalence of home births with lack of resources to allow HBV vaccination at home, unreliable vaccine supplies, and lack of timely administration; for example; only 1% of infants in Nigeria and the Gambia were vaccinated within 24 hours of birth v. 50% of infants in Botswana.48 Additionally, the relatively high cost for HBV vaccines in some African countries, despite the possibility of obtaining HBV vaccine at costs as low as USD0.30 per dose, and the global unavailability of an HCV vaccine are also challenges for the primary prevention of HCC.49 Limitations in viral hepatitis diagnosis and treatment are also prevalent in low-resource countries, including: significant deficits in the numbers and capabilities of healthcare workers; lack of medical infrastructure, diagnostic methods and laboratories; unavailability of first line HBV treatments, e.g. tenofovir, which has a high barrier to resistance, necessitating the use of older medications with a higher risk of resistance; high costs of HCV treatment; and the required specific follow-up.38 Several strategies have been suggested to improve viral hepatitis management in African countries: engaging decision makers from governmental and non-governmental organisations to find the needed resources within the country's budget; developing a clear policy that recommends administration of the HBV vaccine to all newborn infants (not only those at high-risk) at birth, preferably within 24 hours, and definitely within 7 days;50establishing appropriate registries to document vaccination; engaging local community and religious leaders to encourage hospital rather than home deliveries, as well as using trained personnel to assist in home deliveries to ensure timely vaccination; storage of vaccines outside the cold chain (CC) in areas with unreliable CC given the stability of HBV vaccine at higher temperatures of 37 - 45°C for up to 4 weeks; identifying the most effective therapy for HBV in the local setting; and decreasing the costs of hepatitis medications.50
Despite the proven benefit for patients who are at risk of developing HCC, comprehensive surveillance programmes are lacking in SSA due to several challenges. Surveillance requires relatively expensive US machines and well-trained personnel. Lack of regional guidelines that take into consideration the limited resources in most SSA countries is another important challenge. Efforts should be spent to adapt the international guidelines (Table 1) and make them more applicable to SSA countries. Patient education about the importance of surveillance through national campaigns, primary care health workers, physicians and/or hepatologists, engaging health policy decision makers, finding financial resources in country budgets, and establishing training programs and documentation registries to monitor surveillance are all suggested strategies for improving HCC surveillance in SSA countries.
Once HCC is diagnosed, there is also a critical need for local capability for the key curative and palliative treatments used for HCC, including surgical resection, local ablation, and locoregional chemoembolisation. There is a need to establish regional centers of excellence, to which patients with early and intermediate stage disease can be referred for treatment. There is also an urgent need for countries governments to approve treatments for advanced stage disease, and to negotiate lower costs for these often-expensive therapies. The recent advances in the development of targeted anticancer therapies, including sorafenib, regorafenib, lenvatinib and the immune checkpoint inhibitor nivolumab can only be deployed to reduce the burden of morbidity and mortality from HCC in sub Saharan Africa if there are ardent efforts to ensure their availability at prices that are within the reach of patients in this region.
Conclusion
HCC incidence correlates closely with the incidence of viral hepatitis B and C, which are the most important risk factors for HCC worldwide. The pathogenic mechanisms underlying HCC development, progression and metastasis are being actively deciphered, and novel discoveries hold promise for the development of effective systemic therapies for patients with intermediate and advanced stage disease. Primary prevention is an important strategy to control HCC in the resource-limited settings of most SSA countries. Finally, screening for HCC in high risk patients leads to detection of HCC at early curative stages, which in turn leads to improvement in overall survival. There is a critical need to build local capability in surgical resection, local ablation, and locoregional chemoembolisation, as well as a major need to address the cost of pharmaceutical treatments for patients with advanced stage disease.
Acknowledgements. We gratefully acknowledge administrative support from Lisa M. Price.
Author contributions. All authors contributed equally to the preparation of the manuscript for publication.
Funding. Mayo Clinic Center for Clinical and Translational Science (CCATS), No. NCATS 1UL1TR002377-01; Mayo Clinic Center for Cell Signaling in Gastroenterology, No. NIDDK P30DK084567-09.
Conflicts of interest. LR has received grant funding from Ariad Pharmaceuticals, Bayer, BTG International, Gilead Sciences, RedHill Biopharma, TARGET PharmaSolutions and Wako Life Sciences. LR also served on advisory boards for Bayer, Exact Sciences and TAVEC.
References
1. Fitzmaurice C, Allen C, Barber RM, et al. Global, regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life-years for 32 cancer groups, 1990 to 2015: A systematic analysis for the global burden of disease study. JAMA oncology 2017;3(4):524-548. https://doi.org/10.1001/jamaoncol.2016.5688 [ Links ]
2. Sartorius K, Sartorius B, Aldous C, Govender PS, Madiba TE. Global and country underestimation of hepatocellular carcinoma (HCC) in 2012 and its implications. Cancer Epidemiol 2015;39(3):284-290. https://doi.org/10.1016/j.canep.2015.04.006 [ Links ]
3. Ladep NG, Lesi OA, Mark P, et al. Problem of hepatocellular carcinoma in West Africa. World J Hep 2014;6(11):783-792. https://doi.org/10.4254/wjh.v6.i11.783 [ Links ]
4. European Association For The Study Of The Liver, European Organisation For Research And Treatment Of Cancer. EASL-EORTC clinical practice guidelines: Management of hepatocellular carcinoma. J Hepatol 2012;56(4):908-943. https://doi.org/10.1016/j.jhep.2011.12.001 [ Links ]
5. Ferlay J, Soerjomataram I, Dikshit R, et al. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer 2015;136(5):E359-386. [ Links ]
6. Stanaway JD, Flaxman AD, Naghavi M, et al. The global burden of viral hepatitis from 1990 to 2013: Findings from the Global Burden of Disease Study 2013. Lancet 2016;388(10049):1081-1088. https://doi.org/10.1016/S0140-6736(16)30579-7 [ Links ]
7. Kew MC. Hepatocellular carcinoma: Epidemiology and risk factors. J Hepatocell Carcinoma 2014;1:115-125. https://doi.org/10.2147/JHC.S44381 [ Links ]
8. Park JW, Chen M, Colombo M, et al. Global patterns of hepatocellular carcinoma management from diagnosis to death: The BRIDGE Study. Liver Int 2015;35(9):2155-2166. https://doi.org/10.1111/liv.12818 [ Links ]
9. Schweitzer A, Horn J, Mikolajczyk RT, Krause G, Ott JJ. Estimations of worldwide prevalence of chronic hepatitis B virus infection: A systematic review of data published between 1965 and 2013. Lancet 2015;386(10003):1546-1555. https://doi.org/10.1016/S0140-6736(15)61412-X [ Links ]
10. Kew MC. Hepatitis B virus infection: The burden of disease in South Africa. South Afr J Epidemiol Infect 2008;23(1):4-8. https://doi.org/10.1080/10158782.2008.11441293 [ Links ]
11. Vermeulen M, Swanevelder R, Chowdhury D, et al. Use of Blood Donor Screening to Monitor Prevalence of HIV and Hepatitis B and C Viruses, South Africa. Emerg Infect Dis 2017;23(9):1560-1563. https://doi.org/10.3201/eid2309.161594 [ Links ]
12. Strickland GT. Liver disease in Egypt: Hepatitis C superseded schistosomiasis as a result of iatrogenic and biological factors. Hepatology 2006;43(5):915-922. https://doi.org/10.1002/hep.21173 [ Links ]
13. Gower E, Estes C, Blach S, Razavi-Shearer K, Razavi H. Global epidemiology and genotype distribution of the hepatitis C virus infection. J Hepatol 2014;61(1 Suppl):S45-57. https://doi.org/10.1016/j.jhep.2014.07.027 [ Links ]
14. Yang JD, Gyedu A, Afihene MY, et al. Hepatocellular carcinoma occurs at an earlier age in Africans, particularly in association with chronic hepatitis B. Am J Gastroenterol 2015;110(11):1629-1631. https://doi.org/10.1038/ajg.2015.289 [ Links ]
15. El-Serag HB. Epidemiology of viral hepatitis and hepatocellular carcinoma. Gastroenterology 2012;142(6):1264-1273.e1261. [ Links ]
16. Ohira H, Abe K, Takahashi A, Zeniya M, Ichida T. Clinical features of hepatocellular carcinoma in patients with autoimmune hepatitis in Japan. J Gastroenterol 2013;48(1):109-114. https://doi.org/10.1007/s00535-012-0616-x [ Links ]
17. Park C-H, Jeong S-H, Yim H-W, et al. Family history influences the early onset of hepatocellular carcinoma. World J Gastroenterol 2012;18(21):2661-2667. https://doi.org/10.3748/wjg.v18.i21.2661 [ Links ]
18. Yang JD, Altekruse SF, Nguyen MH, Gores GJ, Roberts LR. Impact of country of birth on age at the time of diagnosis of hepatocellular carcinoma in the United States. Cancer 2017;123(1):81-89. https://doi.org/10.1002/cncr.30246 [ Links ]
19. Makarova-Rusher OV, Altekruse SF, McNeel TS, et al. Population attributable fractions of risk factors for hepatocellular carcinoma in the United States. Cancer 2016;122(11):1757-1765. https://doi.org/10.1002/cncr.29971 [ Links ]
20. Yang JD, Mohamed EA, Aziz AOA, et al. Characteristics, management, and outcomes of patients with hepatocellular carcinoma in Africa: A multicountry observational study from the Africa Liver Cancer Consortium. Lancet Gastroenterol Hepatol 2017;2(2):103-111. https://doi.org/10.1016/S2468-1253(16)30161-3 [ Links ]
21. Li S, Mao M. Next generation sequencing reveals genetic landscape of hepatocellular carcinomas. Cancer Lett 2013;340(2):247-253. https://doi.org/10.1016/j.canlet.2012.09.027 [ Links ]
22. Lamontagne RJ, Bagga S, Bouchard MJ. Hepatitis B virus molecular biology and pathogenesis. Hepatoma Res 2016;2:163-186. https://doi.org/10.20517/2394-5079.2016.05 [ Links ]
23. De Oliveria Andrade LJ, D'Oliveira A, Melo RC, De Souza EC, Costa Silva CA, Paraná R. Association between hepatitis C and hepatocellular carcinoma. J Glob Infect Dis 2009;1(1):33-37. https://doi.org/10.4103%2F0974-777X.52979 [ Links ]
24. Goossens N, Hoshida Y. Hepatitis C virus-induced hepatocellular carcinoma. Clin Mol Hepatol 2015;21(2):105-114. https://doi.org/10.3350%2Fcmh.2015.2L2.105 [ Links ]
25. Dhanasekaran R, Bandoh S, Roberts LR. Molecular pathogenesis of hepatocellular carcinoma and impact of therapeutic advances. F1000Res 2016;5:F1000 Faculty Rev 879. https://doi.org/10.12688%2Ff1000research.6946.1 [ Links ]
26. Nault JC, Zucman-Rossi J. TERT promoter mutations in primary liver tumors. Clin Res Hepatol Gastroenterol 2016;40(1):9-14. https://doi.org/10.1016/j.clinre.2015.07.006 [ Links ]
27. Pinyol R, Tovar V, Llovet JM. TERT promoter mutations: gatekeeper and driver of hepatocellular carcinoma. J Hepatol 2014;61(3):685-687. https://doi.org/10.1016/j.jhep.2014.05.028 [ Links ]
28. Cancer Genome Atlas Research Network. Comprehensive and integrative genomic characterization of hepatocellular carcinoma. Cell 2017;169(7):1327-1341.e1323. https://doi.org/10.1016/j.cell.2017.05.046 [ Links ]
29. Nault JC, Mallet M, Pilati C, et al. High frequency of telomerase reverse-transcriptase promoter somatic mutations in hepatocellular carcinoma and preneoplastic lesions. Nat Commun 2013;4:2218. https://doi.org/10.1038/ncomms3218 [ Links ]
30. Ferber MJ, Montoya DP, Yu C, et al. Integrations of the hepatitis B virus (HBV) and human papillomavirus (HPV) into the human telomerase reverse transcriptase (hTERT) gene in liver and cervical cancers. Oncogene 2003;22(24):3813-3820. https://doi.org/10.1038/sj.onc.1206528 [ Links ]
31. Schulze K, Nault JC, Villanueva A. Genetic profiling of hepatocellular carcinoma using next-generation sequencing. J Hepatol 2016;65(5):1031-1042. https://doi.org/10.1016/j.jhep.2016.05.035 [ Links ]
32. Cevik D, Yildiz G, Ozturk M. Common telomerase reverse transcriptase promoter mutations in hepatocellular carcinomas from different geographical locations. World J Gastroenterol 2015;21(1):311-317. https://doi.org/10.3748/wjg.v21.i1.311 [ Links ]
33. Hussain SP, Schwank J, Staib F, Wang XW, Harris CC. TP53 mutations and hepatocellular carcinoma: Insights into the etiology and pathogenesis of liver cancer. Oncogene 2007;26(15):2166-2176. https://doi.org/10.1038/sj.onc.1210279 [ Links ]
34. Inokawa Y, Inaoka K, Sonohara F, Hayashi M, Kanda M, Nomoto S.Molecular alterations in the carcinogenesis and progression of hepatocellular carcinoma: Tumor factors and background liver factors. Oncol Lett 2016;12(5):3662-3668. https://doi.org/10.3892/ol.2016.5141 [ Links ]
35. Gramantieri L, Fornari F, Callegari E, et al. MicroRNA involvement in hepatocellular carcinoma. J Cell Mol Med 2008;12(6A):2189-2204. https://doi.org/10.1111/j.1582-4934.2008.00533.x [ Links ]
36. Kgatle MM, Setshedi M, Hairwadzi HN. Hepatoepigenetic alterations in viral and nonviral-induced hepatocellular carcinoma. BioMed Res Int 2016;2016:3956485. https://doi.org/10.1155/2016/3956485 [ Links ]
37. Wang Y, Toh HC, Chow P, et al MicroRNA-224 is up-regulated in hepatocellular carcinoma through epigenetic mechanisms. FASEB J 2012;26(7):3032-3041. https://doi.org/10.1096/fj.11-201855 [ Links ]
38. Lemoine M, Nayagam S, Thursz M. Viral hepatitis in resource-limited countries and access to antiviral therapies: current and future challenges. Future Virol 2013;8(4):371-380. https://doi.org/10.2217/fvl.13.11 [ Links ]
39. Bolondi L, Sofia S, Siringo S, et al. Surveillance programme of cirrhotic patients for early diagnosis and treatment of hepatocellular carcinoma: a cost effectiveness analysis. Gut 2001;48(2):251-259. [ Links ]
40. Bruix J, Sherman M, American Association for the Study of Liver Diseases. Management of hepatocellular carcinoma: An update. Hepatol 2011;53(3):1020-1022. https://doi.org/10.1002/hep.24199 [ Links ]
41. Berhane S, Toyoda H, Tada T, et al. Role of the GALAD and BALAD-2 serologic models in diagnosis of hepatocellular carcinoma and prediction of survival in patients. Clinic Gastroenterol Hepatol 2016;14(6):875-886.e876. https://doi.org/10.1016/j.cgh.2015.12.042 [ Links ]
42. Best J, Bilgi H, Heider D, et al The GALAD scoring algorithm based on AFP, AFP-L3, and DCP significantly improves detection of BCLC early stage hepatocellular carcinoma. Z Gastroenterol 2016;54(12):1296-1305. https://doi.org/10.1055/s-0042-119529 [ Links ]
43. Caviglia GP, Abate ML, Petrini E, Gaia S, Rizzetto M, Smedile A. Highly sensitive alpha-fetoprotein, Lens culinaris agglutinin-reactive fraction of alpha-fetoprotein and des-gamma-carboxyprothrombin for hepatocellular carcinoma detection. Hepatol Res 2016;46(3):E130-135. https://doi.org/10.1111/hepr.12544 [ Links ]
44. Johnson PJ, Pirrie SJ, Cox TF, et al. The detection of hepatocellular carcinoma using a prospectively developed and validated model based on serological biomarkers. Cancer Epidemiol Biomarkers Prev 2014;23(1):144-153. https://doi.org/10.1158/1055-9965.EPI-13-0870 [ Links ]
45. Kyei-Nimakoh M, Carolan-Olah M, McCann TV. Millennium development Goal 5: Progress and challenges in reducing maternal deaths in Ghana. BMC Pregnancy Childbirth 2016;16(1):51. https://doi.org/10.1186/s12884-016-0840-0 [ Links ]
46. World Health Organisation. Guidelines for the Prevention Care and Treatment of Persons with Chronic Hepatitis B Infection. Geneva: WHO, 2015. [ Links ]
47. Shiferaw F, Letebo M, Bane A. Chronic viral hepatitis: policy, regulation, and strategies for its control and elimination in Ethiopia. BMC Pub Health 2016;16(1):769. https://doi.org/10.1186/s12889-016-3459-1 [ Links ]
48. Breakwell L, Tevi-Benissan C, Childs L, Mihigo R, Tohme R. The status of hepatitis B control in the African region. Pan Afr Med J 2017;27(Suppl 3):17. https://doi.org/10.11604/pamj.supp.2017.27.3.11981 [ Links ]
49. Lingwood RJ, Boyle P, Milburn A, et al. The challenge of cancer control in Africa. Nature Rev Cancer 2008;8(5):398-403. https://doi.org/10.1038/nrc2372 [ Links ]
50. Borresen ML, Koch A, Biggar RJ, et al Effectiveness of the targeted hepatitis B vaccination program in Greenland. Am J Public Health 2012;102(2):277-284. https://doi.org/10.2105/AJPH.2011.300239 [ Links ]
51. Heimbach J, Kulik LM, Finn R, et al. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatol 2017;67(1):358-380. https://doi.org/10.1002/hep.29086 [ Links ]
52. Omata M, Cheng AL, Kokudo N, et al Asia-Pacific clinical practice guidelines on the management of hepatocellular carcinoma: A 2017 update. Hepatol Int 2017;11(4):317-370. https://doi.org/10.1007/s12072-017-9799-9 [ Links ]
 Correspondence:
Correspondence:
L R Roberts
roberts.lewis@mayo.edu


{kind=link}