










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.107 n.10 Pretoria Oct. 2017
http://dx.doi.org/10.7196/samj.2017.v107i10.12171
RESEARCH
Distribution of hepatitis B virus infection in Namibia
P MhataI; T W RennieII; L F SmallIII; P M Nyarang'oIV; Z ChaglaV; C J HunterVI
IMPH; Disease Surveillance Officer, World Health Organization, Windhoek, Namibia
IIPhD; Department of Pharmacy Practice and Policy, School of Pharmacy, Faculty of Health Sciences, University of Namibia, Windhoek, Namibia
IIIRN, PhD; Department of General Nursing Science, School of Nursing, Faculty of Health Sciences, University of Namibia, Windhoek, Namibia
IVMB ChB, MPH; Department of Surgery, School of Medicine, Faculty of Health Sciences, University of Namibia, Windhoek, Namibia
VMD, MPH; Division of Infectious Diseases, Department of Medicine, Faculty of Health Sciences, McMaster University, Hamilton, Canada
VIMD, PhD; Departments of Internal Medicine and Physiology, School of Medicine, Faculty of Health Sciences, University of Namibia, Windhoek, Namibia
ABSTRACT
BACKGROUND. Namibia regards hepatitis B virus (HBV) infection as a public health problem and introduced hepatitis B vaccinations for infants during 2009. However, information on HBV infection in the country remains limited, and effective public health interventions may be compromised in the absence of adequate evidence-based data. Available data from the World Health Organization (WHO) estimate that 15 - 60% of the normal population in many African countries may be positive for one or more of the HBV serological markers.
OBJECTIVE. To investigate the distribution of HBV infection in Namibia, using available laboratory data for 2013.
METHODS. A cross-sectional descriptive study was conducted using pre-existing electronic laboratory data on HBV infection. The data were retrieved from the central Namibia Institute of Pathology laboratory in Windhoek during January - December 2013. Tests were done on the following three main groups: (i) pregnant women during routine antenatal care (ANC) visits; (ii) patients with HIV/AIDS during antiretroviral therapy clinic visits; and (iii) any other individual suspected of having HBV infection.
RESULTS. Of a total of 77 238 hepatitis B surface antigen test results retrieved countrywide, 9 087 (11.8%) were positive. Of the positive results, 246/9 087 (2.7%) were in children aged 0 - 14 years, with the sexes equally affected. HBV infections increased markedly, particularly among females, in the age group 15 - 39 years, reaching a peak in the age group 30 - 34 years. Routine screening of pregnant women for HBV during ANC visits was found to be systematically conducted in only two regions, Ohangwena and Khomas.
CONCLUSIONS. This study showed high proportions of positive results in pregnant women, patients with HIV/AIDS and individuals suspected of having HBV infection. The Ministry of Health and Social Services and stakeholders may wish to consider improving the routine and surveillance reporting systems for viral hepatitis and uptake of screening for pregnant women in all regions, and expanding HBV screening to other population groups. Population-based or similar studies are therefore required to determine the HBV prevalence and risk factors. This will assist Namibia in developing appropriate national viral hepatitis strategies as per WHO recommendations.
Hepatitis is a potentially life-threatening viral infection that can be caused by the hepatitis A, B, C, D or E viruses.[1] Of these five types, hepatitis B virus (HBV) infection is the commonest and poses a major global health problem. It can result in chronic infection, putting people at an increased risk of death from cirrhosis and liver cancer.[1,2] The World Health Organization (WHO) estimates that 15 - 60% of the apparently healthy population in many African countries may be positive for one or more of the HBV serological markers.[1,2] Data on both the population-based and facility-based HBV burden in sub-Saharan Africa (SSA) are limited, but the rate of chronic HBV infection is estimated to be >8% in this region.[1-3] Prevention of hepatitis B includes vaccination, screening, monitoring asymptomatic positive patients (and treating them with antivirals if necessary), and follow-up care for symptomatic patients.[4,5]
Namibia, with a population of 2.3 million, currently has 14 political regions, but at the time of the study there were 13 regions, and our analysis is based on the latter figure.[5] The regions are further divided into regional constituencies, localities and villages. The regional health directorates are subdivided into 34 health districts, 34 district hospitals, 44 health centres and over 265 clinics.[5] There are four main private hospitals with numerous smaller private care facilities across the country.[5] The Namibia Institute of Pathology (NIP) is the main laboratory, and has a presence in each of the 34 health districts. All the pathology test results are captured in the central NIP database in Windhoek. The Ministry of Health and Social Services (MoHSS) antiretroviral therapy (ART) policy requires that: (i) all pregnant women be screened for hepatitis B at their first antenatal care (ANC) clinic visit; and (ii) all HIV-positive clients be screened during their first ART visit, so that HBV infection can be identified early and remedial action taken.[5] Furthermore, doctors would normally request a laboratory test for hepatitis B for people presenting with jaundice or any suspected liver disease, to rule out HBV infection.
As in many SSA countries, data on the burden of viral hepatitis in Namibia are limited.[5,6] Available HBV prevalence data are from studies conducted more than two decades ago. These include a prevalence study in a general population in Kavango region in 1983,[7] studies on the carrier state in children in Ovamboland in 1984[8] and on serological markers of HBV in Eastern Caprivi in 1991,[9] and a study of the !Kung children in Bushmanland in 1994.[10] HBV prevalence in these studies ranges from 11% to 17%. The absence of recent and updated HBV data may compromise the country's efforts to initiate an informed and appropriate national viral hepatitis strategy in 2016 - 2021 and to achieve the goal of global elimination of hepatitis B and C by 2030, as recommended by the WHO.
Objective
To investigate the distribution of HBV infection in Namibia using the pre-existing NIP laboratory data for 2013, to provide an update on and evidence-based policy guidance for HBV prevention and control in the country.
Methods
Design. This was a cross-sectional descriptive health facility-based study of all pre-existing test results for hepatitis B that were extracted from the main NIP laboratory database in Windhoek during 1 January - 31 December 2013.
Setting. The Windhoek NIP laboratory is the central point where the database of all results of specimens taken or tested in all district or health facility NIP laboratories countrywide is located and managed.
Study population. The study population included: (i) all pregnant women who were tested for HBV during their first ANC visit; (ii) all patients with HIV/AIDS who were tested for HBV during their routine ART visits; and (iii) any other individual suspected of having HBV infection. The three groups were inferred from information on laboratory request forms, e.g. those with HAART/CDC/ARV on their form were categorised as patients with HIV/AIDS, and those with Maternity/ANW/ANCW/ANC on their form were categorised as pregnant women or infants, depending on age and sex.
For the purposes of the study, if individual results were not explicitly recorded as ANC or HIV/AIDS-related (as described above) on the request form, they were grouped as 'tested on clinical suspicion'. The accuracy of the information recorded by the requesting clinician could not be verified. In addition, demographic and clinical information on the patients was sometimes either missing or incomplete.
Serological testing. The NIP laboratory uses the ARCHITECT hepatitis B surface antigen (HBsAg) qualitative assay (Abbott Laboratories, Sligo, Ireland) which is a chemiluminescent micro-particle immunoassay for the qualitative detection of HBsAg in human serum and plasma.
Statistical analysis. Records were retrieved and cleaned by removing obvious duplications or inconsistencies. Duplications were identified through filtering for surname, sex and age. These records were then reviewed and deleted if found to be duplicates. Data were analysed using IBM SPSS Statistics, version 24 (IBM Corporation, USA).
Ethical considerations. Permission to conduct the survey was granted by the permanent secretary of the MoHSS (ref. no. 17/3/3) and the chief executive officer of the NIP laboratories (no reference number provided). After the database had been filtered for duplications, the data were de-identified to ensure confidentiality.
Results
A total of 77 238 HBsAg test results were retrieved and analysed during the study period. A total of 9 087 results (11.8%) were positive, and these were analysed by region and by selected population groups.
Kavango region showed the highest number of positive results for HBV (n=2 027, 16.3%), followed by Ohangwena (n=535, 11.2%) and Omusati (n=820, 16.1%) (Table 1).

The HBV-positive results from Kavango region represented 22.3% of the total positive results in the country, and the positive results from Ohangwena and Khomas represented 16.9% each. The health facilities in eight regions, starting from Otjozondjupa northwards and including those bordering Angola and Zambia, showed the highest HBsAg positivity rates in the country (Fig. 1). Kavango, Ohangwena and Khomas also had the highest number of HBV-positive results in the age group 15 - 34 years.

Of the total 9 087 positive HBV test results, 5 391 (59.3%) were for females and 3 519 (38.7%) for males (gender was missing for 177 positive results (1.9%)).
Of the positive results, 246/9 087 (2.7%) were in children aged 0 -14 years, with the sexes equally affected. Fig. 2 shows that there was a high rate of HBV-positive results in the age group 15 - 39 years (72.9%, 6 625 out of the total 9 087 positive results). Females were the most affected, with over twice as many positive results than males, peaking in the age group 30 - 34 years. From the age of 40 years, however, the number of positive HBV test results for males exceeded that for females (1 238 positive results for males v. 948 for females).

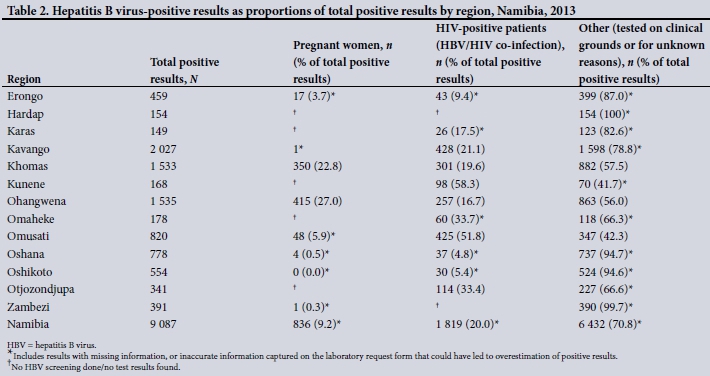
Tables 2 and 3 show further analysis of the HBV screening results for routine ANC clients and for people living with HIV/AIDS, as well as those tested on clinical suspicion for hepatitis B or unknown reasons on the laboratory request form.
The numbers and proportions of positive HBV results in the HIV-positive patients tested at ART visits, and in the pregnant women who were tested at ANC visits, were 1 819 (20.0%) and 836 (9.2%), respectively. The remaining positive HBV results ('other'), numbering 6 432 (70.8%) of the total 9 087 positive results, included the results of tests requested on clinical grounds and results with missing information or inaccurate information captured on the laboratory request form.
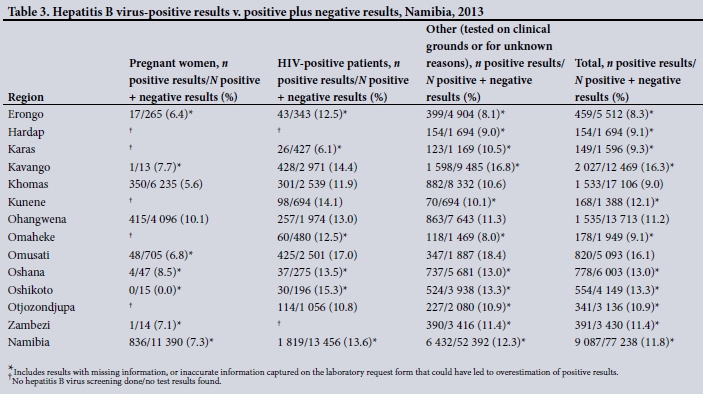
Routine screening for HBV of pregnant women during ANC visits was found to be systematically conducted only in two regions, Ohangwena, with 415 (10.1%) positive out of 4 096 test results, and Khomas, with 350 (5.6%) positive out of 6 235 test results (Table 3). Data on HBV screening of pregnant women from the remaining 11 regions were incomplete or missing (Tables 2 and 3).
A total of 836 (7.3%) of 11 390 (positive plus negative) HBV results retrieved for pregnant women were positive. For patients with HIV/AIDS (i.e. co-infected with HBV and HIV/AIDS), the figure was 1 819 (13.6%) out of 13 456 results retrieved (Table 3).
Omusati region recorded the highest positivity rate of 17.0% (HIV/HBV co-infection). Rates of HBV/HIV co-infection were also high in Oshikoto (15.3%), Kavango (14.4%), Kunene (14.1%), Oshana (13.5%) and Ohangwena (13%). With the exception of Karas (6.1%), all the regions had HIV/HBV co-infection rates >10%.
The HBV positivity rate for individuals tested on clinical grounds or for other reasons was 12.3% (6 432 positive out of a total of 52 392 tests in this category) (Table 3).
Data from the annual returns of the MoHSS health information system on hepatitis B notifications to the MoHSS Health Information System (inpatients and out-patients) showed a total of only 501 cases of hepatitis B during January - December 2013 nationally, compared with 77 238 test results retrieved from the NIP laboratory database, of which 9 087 were positive, during the same reporting period.
Discussion
This study findings show that rates of HBV-positive results were very high (11.8%) in Namibia, particularly in the seven northern regions of Kavango, Omusati, Ohangwena, Oshikoto, Oshana, Kunene and Zambezi (formerly Caprivi). These findings are similar to those in a prevalence study conducted in 1983 in Kavango by Joubert et al.,[7] which showed an HBsAg prevalence of 13.6%. The current study showed the rate of positive results to be highest for Kavango (16.3%).
A high proportion of positive results among 0 - 14-year-olds nationally (246 (2.7%) of the total of 9 087 positive results) can be attributed to historical trends in the northern regions that include both vertical transmission of HBV and later horizontal transmission during early childhood. This is in accordance with a 1984 study of hepatitis B in children in Ovamboland, Namibia, by Botha et al.,[8] which showed a 13% rate of HBsAg positivity among children aged >6 months.[8] A study of HBsAg prevalence among the !Kung (San) children in 1994 showed a similar trend, with a figure of 7.8%.[10] We found that positive results in the age group 10 - 14 years occurred mainly in the northern regions, i.e. Kavango (19.8%), Omusati (19.8%) and Ohangwena (14.9%), together with Khomas (13.2%), where Namibia's capital city is situated. HBsAg rates are similar in many other sub-Saharan African countries.[11-13]
HBsAg screening of pregnant women was not done systematically in 11 out of 13 regions, and data capturing on the laboratory request forms may have been inaccurate, resulting in over-estimation of positive results in the category of tests done on clinical grounds. HBV screening of pregnant women needs to be strengthened to improve early detection and consequent prevention of vertical transmission from the infected mother to the newborn.
The HBV positivity and HBV/HIV co-infection rates of 11.8% and 13.6% in this study were based on only a small proportion of the Namibian population - mainly pregnant women, people with HIV/AIDS, and individuals with signs and symptoms suggestive of viral hepatitis. The vast majority, who are not pregnant or whose HIV status is unknown, will remain undiagnosed and in many cases continue to constitute a reservoir of infection and a threat to their household, social and sexual contacts. They are likely to be screened only when they present with clinical features of liver disease and even evidence of complications. Namibia must be commended for maintaining high HBV immunisation coverage of infants aged <1 year (83%), although there is a need to improve coverage of healthcare workers.[11,13]
Recommendations
The study findings have several implications for Namibia's public health programmes. While the data are clearly limited, there is evidence of a significant burden of HBV in the country. Further prospective studies should be planned and carried out in order to address key issues facing the Namibian MoHSS. These include expanding immunisation to other age groups, and treatment and monitoring of HBV-positive individuals who are not pregnant or are of unknown HIV status. Significant work is needed to improve the information captured at and recorded from the clinical sites. Better data collection and storage will allow for a more informed and programmatic approach to the public health control of HBV in Namibia.
Study limitations
These findings are based on health facility data only, and some duplicate test results may have been included in the analysis. Furthermore, it was not possible to identify risk factors that could be associated with sociocultural and economic variables in the population-derived samples. While the findings could be useful in estimating health facility-based HBV prevalence in specific selected groups or regions, they may not be generalisable to or a true representation of the general population. Data capturing for morbidity and mortality due to HBV infections, including liver cancer, in Namibia are generally insufficient to provide evidence-based policy/strategy guidance.
Conclusions
This study showed high proportions of positive results among pregnant women, people with HIV/AIDS, and individuals suspected of having HBV infection on clinical grounds. However, the general population, who are not pregnant or whose HIV status is unknown, are unlikely to have access to HBV screening.
The MoHSS and stakeholders may wish to consider improving the uptake of screening for pregnant women, and even expanding HBV screening to other population groups. Furthermore, the identification and management of HBV-positive women and their newborns may need to be improved to prevent or reduce vertical transmission.
Viral hepatitis seems to be under-reported by both the routine and surveillance reporting systems in Namibia. This compromises evidence-based national strategy development for attaining the WHO goal of global elimination of hepatitis B and C by the year 2030. Population-based or similar studies are therefore required to determine the prevalence of and risk factors for HBV. This will assist the country in developing appropriate national viral hepatitis strategies as per the WHO recommendations.
Acknowledgements. We thank the Namibian Ministry of Health and Social Services and the Namibia Institute of Pathology for giving us access to the HBV data.
Author contributions. PM (with CJH and LFS) conceived the study, collected the data and authored the article; TWR (with CJH) supervised the data analysis and critically reviewed the manuscript; LFS critically reviewed the manuscript; ZC audited the data analysis and critically reviewed the manuscript; PMN audited the data analysis and critically reviewed the manuscript; and CJH provided overall supervision for the project.
Funding. The study was funded by the Faculty of Health Sciences, University of Namibia.
Conflicts of interest. None.
References
1. World Health Organization. Prevention & Control of Viral Hepatitis Infection: Framework for Global Action. Geneva: WHO, 2012. [ Links ]
2. World Health Organization. Global Policy Report on the Prevention and Control of Viral Hepatitis. Geneva: WHO, 2013. [ Links ]
3. Ministry of Health and Social Services, Namibia. Namibia Demographic and Health Survey. Windhoek: MoHSS, 2013. [ Links ]
4. World Health Organization. Guidelines for the Prevention Care and Treatment of People Infected with Viral Hepatitis. Geneva: WHO, 2015. [ Links ]
5. Ministry of Health and Social Services, Namibia. National Guidelines for Antiretroviral Therapy. 4th ed. Windhoek: MoHSS, 2014. [ Links ]
6. Brandt LR, Tadesse T, Angala MP, Kalibbala M, Mendai R, Egodhi MT. Prevalence of chronic hepatitis B virus infection among HIV-infected children in northern Namibia. Presented at AIDS 2012, Washington, DC, 22 - 27 July 2012. http://www.go2itech.org/where-we-work/namibia/downloads/FINAL_iAS_NAM_HepB_HIV.pdf/view (accessed 11 August 2017). [ Links ]
7. Joubert JJ, Prozesky OW, Lourens JG, et al. Prevalence of hepatitis virus and some arbovirus infections in Kavango, Northern Namibia. S Afr Med J 1985;67(13):500-502 [ Links ]
8. Botha JF, Ritchie MJ, Dusheiko GM, Mouton HW, Kew MC. Hepatitis B virus carrier state in black children in Ovamboland: Role of perinatal and horizontal infection. Lancet 1984;1(8388):1210-1212. https://doi.org/10.1016/s0140-6736(84)91694-5 [ Links ]
9. Joubert J J, van der Merwe C A, Lourens J H, Lecatsas G, Siegrühn C. Serological markers of hepatitis B virus and certain other viruses in the population of eastern Caprivi, Namibia. Ann Trop Paediatr 1991;85(1):101-103. https://doi.org/10.1016/0035-9203(91)90176-Y [ Links ]
10. Aspinall S, Joubert JJ, Evans AC, Joseph S, Steele AD, Lecatsas G. Prevalence of hepatitis B in !Kung (San) children from Bushmanland, Namibia. Ann Trop Paediatr 1994;14(2):163-167. https://doi.org/10.1080/02724936.1994.11747711 [ Links ]
11. World Health Organization, HIV Department and Global Hepatitis Program. Towards the Elimination of Hepatitis B and C by 2030. Draft WHO Global Hepatitis Strategy, 2016-2021 and Global Elimination Targets. Geneva: WHO, 2015. [ Links ]
12. Burnett RJ, Kramvis A, Dochez C, Meheus A. An update after 16 years of hepatitis B vaccination in South Africa. Vaccine 2012;30(Suppl 3):C45-C51. https://doi.org/10.1016/j.vaccine.2012.02.021 [ Links ]
13. Ministry of Health and Social Services, Namibia. Quality Assurance: Annual Report on Hepatitis B Vaccinations among Health Care Workers. Namibia. Windhoek: MoHSS, 2012. [ Links ]
 Correspondence:
Correspondence:
C J Hunter
chunter@unam.na
Accepted 2 May 2017


{kind=link}
{kind=link}