










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSAMJ: South African Medical Journal
versão On-line ISSN 2078-5135
versão impressa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.107 no.9 Pretoria Set. 2017
http://dx.doi.org/10.7196/samj.2017.v107i9.12090
RESEARCH
A third of patients treated at a tertiary-level surgical service could be treated at a secondary-level facility
S van StratenI; C StannardI; J BulabulaI; K PaulI; J LeongI; M J KlipinII
I5th-year MB BCh student; School of Clinical Medicine, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IIFCS (SA); Department of Surgery, School of Clinical Medicine, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
ABSTRACT
BACKGROUND. South Africa (SA) has an overburdened public healthcare system. Some patients admitted to Charlotte Maxeke Johannesburg Academic Hospital (CMJAH), SA, may not require tertiary care, but the numbers and details are uncertain. Clinical research in SA is limited by scarce skills and limited access to data.
OBJECTIVE. To determine the proportion of and length of stay for secondary-, tertiary- and quaternary-level patients discharged from the Department of Surgery at CMJAH over 1 year.
METHODS. This is a retrospective analysis of electronic discharge (ED) summaries from the Department of Surgery at CMJAH between 1 April 2015 and 1 April 2016. An SQL query of the database generated a .csv file of all discharges with the following fields: database reference number, length of stay and level of care. The details of each record were verified by MBBCh V students, using a defined level-of-care template and the full discharge summary. The data were reviewed by a senior clinician.
RESULTS. There were 3 007 discharge summaries - 97 were not classifiable, two were test records and one was a duplicate. These 100 records were excluded. There were no primary-level records. Secondary-level patients represented 29% (854) of those discharged and 19% of total bed days. Tertiary- and quaternary-level patients together represented 71% of the total and 81% of bed days. The average length of stay was 4.31 days for secondary, 6.98 days for tertiary and 9.77 days for quaternary level-of-care allocation.
CONCLUSION. Almost one-third (29%) of patients discharged from CMJAH's Department of Surgery were deemed suitable for secondary-level care. These patients had a shorter length of stay and comprised 19% of total bed days. Students and electronic databases represent an important research resource.
South Africa (SA) suffers from a quadruple burden of disease, i.e. communicable, non-communicable, perinatal and maternal, and injury-related diseases.[1] Non-communicable diseases are increasing in both rural and urban areas, most prominently in the urban poor, resulting in pressure on acute and chronic healthcare services.[2]
The Lancet Commission on Global Surgery estimates that 28 -32% of the global burden of disease is considered to be treatable by surgery, and has labelled surgery as the 'forgotten stepchild' of primary healthcare[3,4]
The public healthcare sector in SA is overburdened at all levels of care.[5] Healthcare funding has not kept pace with inflation and the burden of disease.[6] Data are necessary to make informed decisions at a clinical, research, management and operational level.[7]
Quaternary and tertiary services are the most expensive and limited resources in the healthcare pyramid. Charlotte Maxeke Johannesburg Academic Hospital (CMJAH), SA, is a referral centre for a wide urban area under the Faculty of Health Sciences, University of the Witwatersrand teaching platform. The hospital is one of eight national referral centres in SA.
Clinical practice and service delivery often take priority at the expense of research.[8] Medical students represent a skilled group, who are willing and keen to participate, and student-aided research in surgery has resulted in several recent publications in prominent journals.[5,9]
CMJAH has four general surgical wards, with a total of 92 beds. The four wards are divided into breast and endocrine, gastroenterology, vascular, and trauma. Each ward admits elective and emergency patients.
An electronic discharge (ED) summary database was implemented in the Department of Surgery at CMJAH in April 2015. It replaced the hand-written paper system. A printed discharge summary and an electronic record for each discharge are created.
The ED summary is a web-based electronic instrument developed by the Faculty of Health Sciences, University of the Witwatersrand. Data are hosted on a secure university platform. End users can access password-protected records for point-of-care information and administrators have access to aggregated data.
There is a feeling among clinicians that some patients requiring secondary- or primary-level care are admitted to CMJAH; however, the number of patients and details are uncertain.
The ED summary database was used to determine the proportion of secondary-, tertiary- and quaternary-level patients who were discharged from the Department of Surgery at CMJAH between 1 April 2015 and 1 April 2016 and the proportion of bed days.
Objective
Our objective was to determine the proportion of secondary-, tertiary-and quaternary-level patients discharged from the Department of Surgery at CMJAH between 1 April 2015 and 1 April 2016, and the proportion of bed days they occupied. Furthermore, we aimed to show that medical students are a valuable research resource. An ED summary database enables aggregated analysis and point-of-care clinical information.
Methods
Interns complete an ED summary for every patient who is discharged from the Department of Surgery at CMJAH. One field is a dropdown box allocating the level of care deemed appropriate. There are a mix of secondary-, tertiary- and quaternary-level patients treated at CMJAH.
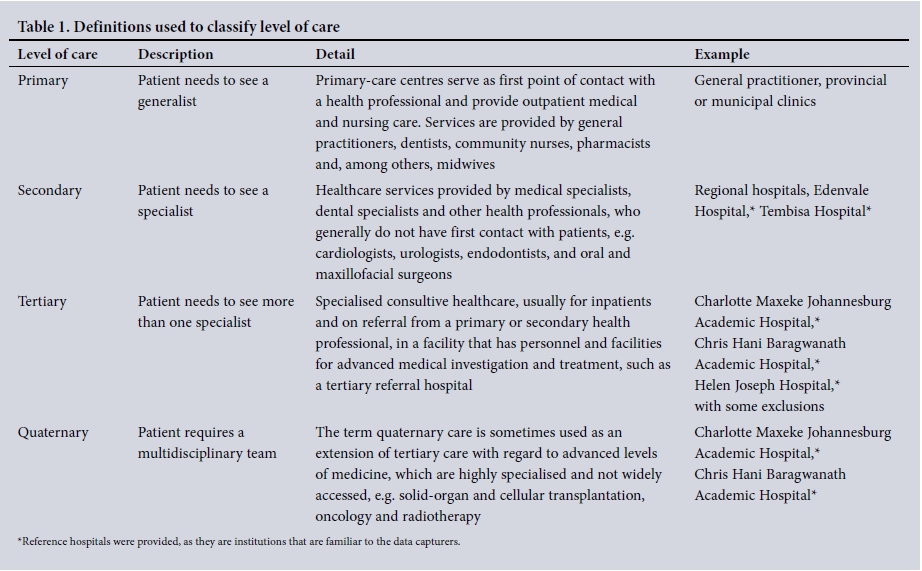
A template with the definition of each level-of-care guided classification is shown in Table 1. For clarity, the levels are listed below.
Primary-care patients are those with conditions within the scope of a first-contact healthcare practitioner. An example would be a skin laceration requiring sutures only.
Secondary care generally requires a specialist opinion or management by more than one clinician. An example would be a healthy young male requiring an appendectomy under general anaesthesia.
Tertiary patients are those with significant comorbidities or who require more than one specialist clinician to manage their condition. An example would be a diabetic patient with renal dysfunction requiring a colectomy.
Quaternary-level patients require highly specialised multi-disciplinary management. Examples include the involvement of solid-organ transplant and oncology teams.
The investigators were less rigid in the distinction between tertiary and quaternary levels, as these patients are managed in the same centre and require access to similar resources.
An SQL query created a list of all discharge summaries from the Department of Surgery at CMJAH from 1 April 2015 to 1 April 2016 in a .csv format (Microsoft Excel 2010, USA). The fields included were: database reference number, length of stay and level of care.
The database reference number is an automatically generated unique number for each record, thus ensuring patient confidentiality.
The length of stay was calculated from the difference between the admission and discharge dates. The number of bed days was calculated from the sum of all recorded lengths of stay. Admission and discharge within a 24-hour period was considered an admission of one day.
Each complete record was reviewed by a 5th-year medical student (Graduate-Entry Medical Programme, Year III, University of the Witwatersrand). These students have 1 year of clinical experience and are familiar with the primary, secondary and tertiary/quaternary classifications and the corresponding healthcare centres that provide the services.
Equivocal records were reviewed with a senior clinician. All records where the length of stay was 0 or >30 days were reviewed and corrected where necessary.
The students were paid at the university undergraduate student rate (ZAR57/hour).
Ethical clearance was obtained from the University of the Witwatersrand Faculty of Health Sciences Human Research Ethics Committee (ref. no. M160431). Permission was granted by the CMJAH chief executive officer.
Results
A total of 3 007 discharge summaries were recorded from 1 April 2015 to 1 April 2016. Of these, 97 were not classifiable, 1 was a duplicate and there were 2 test patients on the system. The final number of records analysed was 2 907 (Table 2).

Primary level
No patients were classified as primary-level care.
Secondary level
Of the 2 907 records, 854 were classified as secondary-level care, comprising 29% of patients discharged, with an average length of stay of 4.31 days. These patients accounted for 19% of the total bed days.
Tertiary level
Records classified as tertiary level numbered 1 612 or 55% of the total discharges, with an average length of stay of 6.98 days. This group accounted for 58% of the total bed days.
Quaternary level
Quaternary level of care comprised 441 or 16% of the total number of patients, with an average stay of 9.77 days. The quaternary group accounted for 23% of total bed days.
Tertiary and quaternary levels together represented 71% of the total discharges and 81% of bed days.
Discussion
There is a paucity of data on the surgical burden of disease in SA and the resources to address this deficit.[10] People who have the skills to abstract clinical data are a scarce and valuable resource.
Higher-income countries report using medical students to address the human resource limitation in data capture and abstraction.[9,11] Productive, relevant research is possible when clinicians engage with and support students toward a defined research goal.
The public healthcare system in SA is overburdened at all levels.[5] Lack of resources results in upward referral owing to local constraints. A tertiary or quaternary hospital is only one component of the healthcare pyramid. If skills and resources are limited, the trend is to refer to better-resourced facilities. The scarcity of skills, supervision and support dictates that doctors in district hospitals refer cases to tertiary centres.[5] This is especially true in surgery, which requires systems to function adequately and simultaneously (theatre, anaesthetics, surgery).[12] In SA, the distribution of doctors and facilities heavily favours urban areas.[5]
The majority of patient records at the Faculty of Health Sciences, University of the Witwatersrand-affiliated teaching hospitals are in a paper-based system format. Data storage and retrieval for point-of-care information and aggregated analysis is cumbersome and often incomplete.
The implementation of the ED summary has provided the Department of Surgery at CMJAH and the Faculty of Health Sciences, University of the Witwatersrand with a platform for clinicians to view patient discharge records for point-of-care information and aggregated data for analysis and research.
In this study, patients requiring secondary-level care represented 29% of the total patient numbers and 19% of the total bed days; the average length of stay was 4.31 days. These patients could potentially be managed at a more cost-effective secondary-level care facility.
Tertiary- and quaternary-level patients represented 71% of the total numbers and 81% of the total bed days. The length of stay was 6.98 and 9.77 days for tertiary and quaternary patients, respectively.
As expected, increasing complexity of disease translates into a prolonged hospital stay.
Study limitations
The ED summary database was implemented in the Department of Surgery at CMJAH in April 2015. There is a learning curve to any technology, which may have skewed the results. This was mitigated by end-user training and support by the ED team.
The ED summary database was designed to mimic the previous paper-based workflow at CMJAH. Patients who were transferred from surgery wards or died may not have had an ED summary.
Conclusion
The ED summary database has made records accessible for patient care and aggregated data analysis. With appropriate technology, end-user training and support, electronic instruments can be successfully implemented and sustained in the SA public healthcare environment.
Medical students are a valuable resource with skills for clinical data abstraction.
At the Department of Surgery, CMJAH, 29% of total patient numbers and 19% of total bed days could potentially have been managed at a more cost-effective secondary-level facility during April 2015 - April 2016.
Acknowledgements. The Department of Surgery at CMJAH, the interns responsible for the generation of the discharge summaries and the Faculty of Health Sciences Biomedical Informatics team are acknowledged.
Author contributions. All authors contributed meaningfully to the production of the manuscript.
Funding. The students were paid the university undergraduate rate (R57/ hour) from research funds of the corresponding author.
Conflicts of interest. None.
References
1. Mayosi BM, Flisher AJ, Lalloo UG, Sitas F, Tollman SM, Bradshaw D. The burden of non-communicable diseases in South Africa. Lancet 2009;374(9693):934-947. https://doi.org/10.1016/S0140-6736(09)61087-4 [ Links ]
2. Coovadia H, Jewkes R, Barron P, Sanders D, McIntyre D. The health and health system of South Africa: Historical roots of current public health challenges. Lancet 2009;374(9692):817-834. https://doi.org/10.1016/s0140-6736(09)60951-x [ Links ]
3. Alkire BC, Raykar NP, Shrime MG, et al. Program in global surgery and social change - global access to surgical care: A modelling study. Lancet Glob Health 2015;3(6):e316-e323. https://doi.org/10.1016/S2214-109X(15)70115-4 [ Links ]
4. Lancet Commission on Global Surgery. Global surgery 2030 indicators policy brief. 2015. http://www.globalsurgery.info/wp-content/uploads/2013/10/Indicators_GS2030.pdf (accessed 27 July 2017). [ Links ]
5. Lloyd B, Sanders D, Lehmann U. Human resource requirements for national health insurance. S Afr Health Rev 2010;2010(1):171-178. [ Links ]
6. Kevany S, Benatar SR, Fleischer T. Improving resource allocation decisions for health and HIV programmes in South Africa: Bioethical, cost-effectiveness and health diplomacy considerations. Glob Public Health 2013;8(10):570-587. https://doi.org/10.1080/17441692.2013.790461 [ Links ]
7. Gray A, Vawda Y. South African Health Review. 2016. https://www.health-e.org.za/wp-content/uploads/2016/05/South-African-Health-Review-2016 (accessed 31 July 2017). [ Links ]
8. Department of Health. Human resources for health. 2011. http://www.gov.za/sites/www.gov.za/files/hrh_strategy_0.pdf (accessed 27 July 2017). [ Links ]
9. STARSurg Collaborative. Multicentre prospective cohort study of body mass index and postoperative complications following gastrointestinal surgery. Br J Surg 2016;103(9):1157-1172. https://doi.org/10.1002/bjs.10203 [ Links ]
10. Beguy D. Poor data affects Africa's ability to make the right policy decisions. 2016. http://theconversation.com/poor-data-affects-africas-ability-to-make-the-right-policy-decisions-64064(accessed 31 July 2017). [ Links ]
11. Nepogodiev D. UK surgical trainees will continue to support European research collaboration. Lancet 2016;388(10043):459-460. https://doi.org/10.1016/S0140-6736(16)31151-5 [ Links ]
12. Meara JG, Leather AJM, Hagander L, et al. Global surgery 2030: Evidence and solutions for achieving health, welfare, and economic development. Lancet 2015;386(9993):569-624. https://doi.org/10.1016/S0140-6736(15)60160-X [ Links ]
 Correspondence:
Correspondence:
M J Klipin
michael.klipin@wits.ac.za
Accepted 21 April 2017


{kind=link}