










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.107 n.9 Pretoria Sep. 2017
http://dx.doi.org/10.7196/samj.2017.v107i9.12206
RESEARCH
White blood cell count and C-reactive protein together remain useful for diagnosis and staging of acute appendicitis in children
S MonsalveI, II; A EllwangerIII; S MontedonicoIV, V, VI
IMD; Department of Pediatric Surgery, Hospital Carlos van Buren, Valparaiso, Chile
IIMD; Clínica Ciudad del Mar, Vina del Mar, Chile
IIIMD; Hospital de Contulmo, Arauco, Chile
IVMD, PhD; Department of Pediatric Surgery, Hospital Carlos van Buren, Valparaiso, Chile
VMD, PhD; Clínica Ciudad del Mar, Vina del Mar, Chile
VIMD, PhD; Centro de Investigaciones Biomédicas, Escuela de Medicina, Universidad de Valparaiso, Valparaiso, Chile
ABSTRACT
BACKGROUND. Acute appendicitis (AA) is the most common acute surgical condition of the abdomen, and the most commonly misdiagnosed.
OBJECTIVE. To analyse the white blood cell count (WBCC) and C-reactive protein (CRP) contribution to the diagnosis of AA in children.
METHODS. This was a retrospective study of 943 consecutive patients operated on with the preoperative diagnosis of AA, in whom preoperative WBCC and CRP had both been measured. Postoperatively, the patients were divided into three groups: normal appendix (no AA), simple AA and complicated AA.
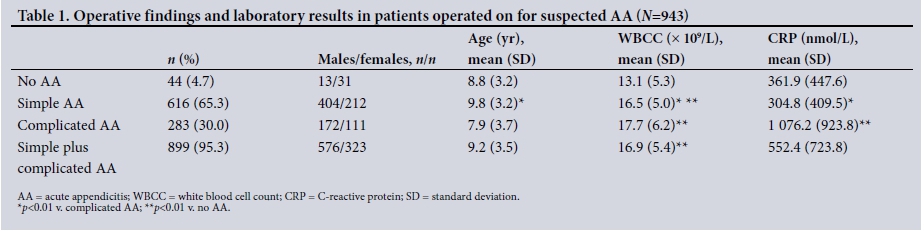
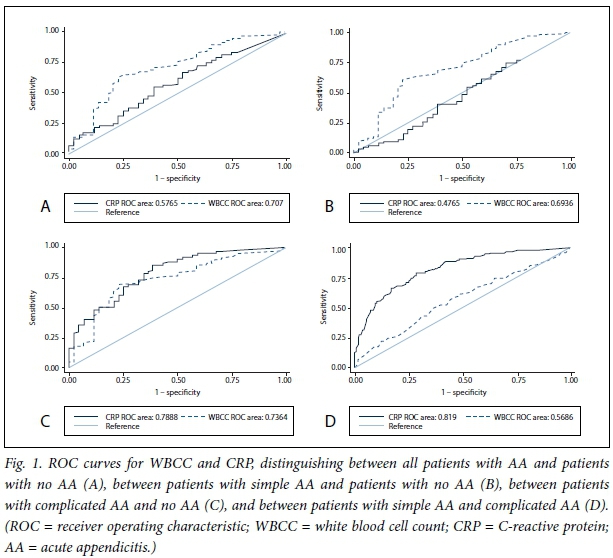
RESULTS. Of the 943 patients, 616 (65.3%) had simple AA. The mean (standard deviation (SD)) age for this group was 9.8 (3.2) years (p<0.01 v. complicated AA), the mean WBCC was 16.5 (5.0) χ 109/L (p<0.01 v. complicated AA and no AA), and the mean CRP level was 304.8 (409.5) nmol/L (p<0.01 v. complicated AA). The mean age of the patients with complicated AA (283/943, 30.0%) was 7.9 (3.7) years, the mean WBCC was 17.7 (6.2) χ 109/L (p<0.01 v. no AA) and the mean CRP level was 1 076.2 (923.8) nmol/L (p<0.01 v. no AA). The mean age of the patients with no AA (44/943, 4.7%) was 8.8 (3.2) years, the mean WBCC was 13.1 (5.3) χ 109/L and the mean CRP was 361.9 (447.6) nmol/L. The WBCC was normal in 113/899 patients with appendicitis (12.6%) and CRP in 139 (15.5%). Both the WBCC and CRP were normal in 17 patients with appendicitis (1.9%). The best receiver operating characteristic (ROC) curve was obtained for WBCC when comparing all AA with no AA: cut-off point 15.0 χ 109/L, sensitivity 65%, specificity 68%, area under the curve 0.70. The best ROC curve for CRP was obtained when comparing simple AA with complicated AA: cut-off point 361.9 nmol/L, sensitivity 74%, specificity 74%, area under the curve 0.81.
CONCLUSIONS. The WBCC is helpful in diagnosing simple AA and CRP in diagnosing complicated AA. If both are normal, AA is very unlikely. Together the WBCC and CRP are useful tools in diagnosing and staging AA.
Acute appendicitis (AA) is the most common acute surgical condition in childhood. The lifetime risk for AA is 9% for men and 7% for women, and the peak incidence occurs between ages 11 and 12 years[1] In children, the classic clinical picture of AA is rare and the diagnosis cannot always be based on history and physical examination alone. The diagnosis of AA is often challenging even in experienced hands, and it is still frequently misdiagnosed. Delays in diagnosis, ranging from 50% to 84% of cases,[2,3] often lead to complicated AA in children aged <5 years. On the other hand, the rate of overdiagnosis leading to negative appendicectomy varies according to age and sex, ranging from 10% to 30%.[4,5] Diagnostic errors in AA have significant economic implications. In a recently published study, the hospital costs of negative appendicectomy in the USA were >USD740 million over a 1-year period.[6
The introduction of ultrasonography and computed tomography (CT) has improved the accuracy of AA diagnosis in recent years. However, heavy reliance on these imaging modalities has some disadvantages. First, CT exposes the patient to radiation and may increase the lifetime risk of cancer. Second, equipment and doctors qualified to interpret images are not always available for every patient in all hospitals worldwide.[6-8]
Leucocytosis and an elevated CRP level have been associated with AA, but there are contradictory results in the literature regarding the contribution of each individual laboratory test or the combination of several values in children. Moreover, the majority of the studies involve small numbers of patients.[9-16]
Objective
To analyse the individual and combined values of the white blood cell count (WBCC) and C-reactive protein (CRP) level in the diagnosis and staging of AA in a large series of children.
Methods
This cross-sectional diagnostic test study was performed in children operated on for AA between August 2007 and December 2011. The Bioethics Committe for Human Research, Faculty of Medicine, Universidad de Valparaiso, Chile, approved the study (date 21 August 2015, no reference number). The medical records were reviewed and the preoperative laboratory tests and intraoperative findings recorded. The inclusion criteria were patients aged <15 years operated on with a presumptive diagnosis of AA, in whom both preoperative WBCC and CRP had been measured. Patients who underwent an interval appendicectomy after non-surgical treatment of AA were excluded from the study.
The WBCC was expressed as χ 109/L and CPR as nmol/L. The upper limit of the reference interval for WBCC was 12.0 χ 109/L[12] and that for CPR was 57 nmol/L.[12,17]
Postoperatively, all patients included in the study were divided into three groups according to the intraoperative macroscopic findings, as follows:
• Normal appendix (no AA). All patients operated on with the preoperative diagnosis of AA but in whom the appendix was found to be macroscopically normal. The findings on histological analysis of the appendix in this group were recorded.
• Simple AA. All non-perforated AA.
• Complicated AA. Perforated appendix, peritonitis, appendicular abscess and appendicular mass.
Statistical analysis
Means (standard deviations (SDs)) were used to describe the numerical variables. Statistical analysis was performed with parametric tests (Student's f-test or analysis of variance). A cross-sectional analysis of the diagnostic tests was performed where sensitivity, specificity and likelihood ratios were calculated. Receiver operating characteristic (ROC) curves were also elaborated for each test and prediction, calculating the area under the curve with a confidence interval of 95%. The level of significance was set at p<0.05.
Results
A total of 943 patients were recruited. The number of patients, gender, mean age and mean WBCC and CRP for each group are shown in Table 1. Of the 943 patients, 899 had a postoperative diagnosis of AA and 44 had a normal appendix. The majority of the patients with AA fell into the simple AA group (n=616, 65.3%). There were only 44 patients (4.7%) with normal appendices. In both AA groups, the vast majority of patients were boys, whereas patients with a negative appendicectomy were mostly girls. Mean age was significantly lower in the complicated AA group than in the other two groups.
Table 1 shows that the WBCC was significantly higher in the patients with AA than in those without. However, separate analysis of the three groups showed that the WBCC was significantly higher in patients with simple AA that in those with no AA, and that patients with complicated AA had higher values than those in the other two groups. CRP was not significantly increased in the overall group of AA compared with the no AA group. CRP was comparable in the simple AA and no AA groups, but was significantly increased in cases of complicated AA in comparison with the other two groups.
Of the 44 patients with a negative appendicectomy, only 5 had no other intra-abdominal cause of pain; 24 children (54.5%) had mesenteric lymphadenitis, 8 (18.2%) had a primary peritonitis, 3 girls had a gynaecological disease, and 4 patients had other diagnoses.
The proportion of simple v. complicated AA varied according to age group. Of the 160 children aged 1 - 5 years, 7 (4.4%) had a normal appendix, 67 (41.9%) had simple AA and 86 (53.8%) had complicated AA. Of the 404 children aged 6 - 10 years, 24 (5.9%) had a normal appendix, 263 (65.1%) had simple AA and 117 (29.0%) had complicated AA. Of the 379 children aged 11 - 15 years, 13 (3.4%) had a normal appendix, 286 (75.5%) had simple AA and 80 (21.1%) had complicated AA.
Patients with normal laboratory results are described in Table 2. There was a similar number of patients with a normal WBCC in the simple AA and complicated AA groups. CRP levels were normal in only 4.2% of patients with complicated AA and 20.6% of those with simple AA. Only 1.9% of the entire group of patients with AA had both WBCCs and CRP levels within the normal ranges
To investigate the diagnostic values of the WBCC and CRP further, ROC curves were calculated (Table 3 and Fig. 1).
Discussion
AA is the most common acute surgical problem in childhood and is frequently misdiagnosed. WBCC and CRP are laboratory tests that are often used to aid diagnosis in children with right lower quadrant pain. Most studies analysing the contribution of inflammatory markers in AA are contradictory, probably because they involved small series of patients, sometimes only numbering 100.[9-16,18] The present study on the contribution of inflammatory markers to the diagnosis of AA was done on >900 patients, making it one of the largest paediatric series reported to date.
The proportion of simple and complicated AA in our study was similar to other paediatric series. [12,18-20]The negative appendicectomy rate was 5%, which is quite low.[21-22] The mean age at diagnosis of AA was similar to those reported in other studies.[11,12,19] However, children with complicated AA were significantly younger than those with simple AA. In the group of children up to 5 years old, more than 50% cases of AA were complicated,[22-24] probably because the diagnosis of complicated AA is a particularly difficult one in this age group. Interestingly, the negative appendicectomy rate in this series was similar in all age groups.
Patients operated on for AA were mainly boys in all groups, in accordance with most previous reports.[20,25,26] However, other researchers have found similar proportions of boys and girls,[10-12,14,18,19] and even a predominance of girls over boys.[15] It is interesting to point out that patients with negative appendicectomies were mainly girls,[13] even when the three patients in this group who had a gynaecological disease are excluded. These findings suggest that girls with right lower quadrant pain should be particularly carefully investigated.
The contribution of the WBCC to the diagnosis of AA in children is controversial. It has been reported that the WBCC was increased in children with AA in comparison with those with negative appendi-cectomies.[14,18] However, other studies did not find differences in the WBCC between the two groups. Stefanutti et al.,[12] in a study of 100 patients who underwent appendi-cectomy, found similar results in children with simple AA and those with negative operative findings. Kim et al.[10]found no differences in the WBCC between children with AA, those with a perforated appendix and those with negative appendicectomies. The results of the present study, involving a large number of patients, demonstrated that WBCC was significantly increased in children with AA in comparison with those with a negative appendicectomy, and also that the WBCC was higher in complicated AA than in simple AA.
We found that CRP levels were similar in children with simple AA and negative appendicectomies. As inflammation of the appendix progresses, CRP increases, reaching values three times higher in complicated AA than in simple AA. Although CRP is therefore not a useful inflammatory marker for simple AA, it does seem useful for detecting appendiceal perforation. These results are in accordance with some earlier reports.[10,11,16,19,25]
Several studies of adult patients have reported that when the WBCC and CRP are normal, the diagnosis of AA can be excluded with high accuracy.[13,27,28] The present study showed that children with AA quite frequently have either a normal WBCC or normal CRP. However, both values were in the normal range in only 1 out of 52 patients with AA. These findings are valuable and are in agreement with previous reports.[10,12]
ROC analysis enables improved estimation of the usefulness of diagnostic tests. However, ROC curves of inflammatory markers in AA in children have rarely been used.[11,19,29] We therefore included this analysis in our study to assess the overall diagnostic value of the WBCC and CRP in AA. Using ROC curves, a substantial degree of heterogeneity was observed for CRP and WBCC.
The WBCC had a mediocre discriminative capability in the overall diagnosis of AA. Of the two laboratory markers, CRP had better discriminative capability in staging AA. A CPR level >362 nmol/L was 2.81 times more frequent in patients with complicated AA than in those with simple AA. These findings are also in agreement with some previous studies.[11,19,29]
Conclusions
The WBCC and CRP level together are useful laboratory tests for diagnosing and staging AA. Whereas an increase in WBCC is an early marker of inflammation of the appendix, CRP is superior in reflecting its perforation. AA is very unlikely in a patient with a normal WBCC and CRP level.
Acknowledgements. The authors thank Hospital Carlos van Buren, Valparaiso, Chile.
Author contributions. S Monsalve: design of the work, data collection and drafting the artricle; A Ellwanger: data analysis, interpretation and statistics; S Montedonico: conception of the work, critical revision of the article and final approval of the version to be published.
Funding. None.
Conflicts of interest. None.
References
1. Addiss DG, Shaffer N, Fowler BS, Tauxe RV. The epidemiology of appendicitis and appendectomy in the United States. Am J Epidemiol 1990;132(5):910-925. https://doi.org/10.1093/oxfordjournals.aje.a115734 [ Links ]
2. Rothrock SG, Pagane J. Acute appendicitis in children: Emergency department diagnosis and management. Ann Emerg Med 2000;36(1):39-51. https://doi.org/10.1067/mem.2000.105658 [ Links ]
3. Colvin JM, Bachur R, Kharbanda AT. The presentation of appendicitis in preadolescent children. Pediatr Emerg Care 2007;23(12):849-855. https://doi.org/10.1097/pec.0b013e31815c9d7f [ Links ]
4. Bachur RG, Hennelly K, Callahan MJ, Chen C, Monuteaux MC. Diagnostic imaging and negative appendectomy rates in children: Effects of age and gender. Pediatrics 2012;129(5):877-884. https://doi.org/10.1542/peds.2011-3375 [ Links ]
5. Flum DR, Morris A, Koepsell T, Dellinger EP. Has misdiagnosis of appendicitis decreased over time? A population-based analysis. JAMA 2001;286(14):1748-1753. https://doi.org/10.1001/jama.286.14.1748 [ Links ]
6. Wray CJ, Kao LS, Millas SG, Tsao K, Ko TC. Acute appendicitis: Controversies in diagnosis and management. Curr Probl Surg 2013;50(2):54-86. https://doi.org/10.1067/j.cpsurg.2012.10.001 [ Links ]
7. Douglas CD, Macpherson NE, Davidson PM, Gani JS. Randomised controlled trial of ultrasonography in diagnosis of acute appendicitis, incorporating the Alvarado score. BMJ 2000;321(7266):919-922. https://doi.org/10.1136/bmj.321.7266.919 [ Links ]
8. Kharbanda AB, Taylor GA, Fishman SJ, Bachur RG. Decision rule can help identify children at lower risk for appendicitis. Pediatrics 2005;116(3):709-716. https://doi.org/10.1542/peds.2005-0094 [ Links ]
9. Grönroos JM. Do normal leukocyte count and C-reactive protein value exclude acute appendicitis in children? Acta Paediatr 2001;90(6):649-951. https://doi.org/10.1111/j.1651-2227.2001.tb02428.x [ Links ]
10. Kim E, Subhas G, Mittal VK, Golladay ES. C-reactive protein estimation does not improve accuracy in the diagnosis of acute appendicitis in pediatric patients. Int J Surg 2009;7(1):74-77. https://doi.org/10.1016/j.ijsu.2008.11.001 [ Links ]
11. Sack U, Biereder B, Elouahidi T, Bauer K, Keller T, Tröbs RB. Diagnostic value of blood inflammatory markers for detection of acute appendicitis in children. BMC Surg 2006;6(1):15. https://doi.org/10.1186/1471-2482-6-15 [ Links ]
12. Stefanutti G, Ghirardo V, Gamba P. Inflammatory markers for acute appendicitis in children: Are they helpful? J Pediatr Surg 2007;42(5):773-776. https://doi.org/10.1016/j.jpedsurg.2006.12.028 [ Links ]
13. Grönroos JM, Grönroos P. Leucocyte count and C-reactive protein in the diagnosis of acute appendicitis. Br J Surg 1999;86(4):501-504. https://doi.org/10.1046/j.1365-2168.1999.01063.x [ Links ]
14. Mekhail P, Naguib N, Yanni F, Izzidien A. Appendicitis in paediatric age group: Correlation between preoperative inflammatory markers and postoperative histological diagnosis. Afr J Paediatr Surg 2011;8(3):309-312. https://doi.org/10.4103/0189-6725.91676 [ Links ]
15. Sengupta A, Bax G, Paterson-Brown S. White cell count and C-reactive protein measurement in patients with possible appendicitis. Ann R Coll Surg Engl 2009;91(2):113-115. https://doi.org/10.1308/003588409X359330 [ Links ]
16. Wu HP, Fu YC. Application with repeated serum biomarkers in pediatric appendicitis in clinical surgery. Pediatr Surg Int 2010;26(2):161-166. https://doi.org/10.1007/s00383-009-2535-3 [ Links ]
17. Oosterhuis WP, Zwinderman AH, Teeuwen M, et al. C reactive protein in the diagnosis of acute appendicitis. Eur J Surg 1993;159(2):115-119. [ Links ]
18. Beltran MA, Almonacid J, Vicencio A, Gutierrez J, Cruces KS, Cumsille MA. Predictive value of white blood cell count and C-reactive protein in children with appendicitis. J Pediatr Surg 2007;42(7):1208-1214.http://dx.doi.org/10.1016/j.jpedsurg.2007.02.010 [ Links ]
19. Okamoto T, Sano K, Ogasahara K. Receiver-operating characteristic analysis of leukocyte counts and serum C-reactive protein levels in children with advanced appendicitis. Surg Today 2006;36(6):515-518. https://doi.org/10.1007/s00595-006-3189-6 [ Links ]
20. Bröker ME, van Lieshout EM, van der Elst M, Stassen LP, Schepers T. Discriminating between simple and perforated appendicitis. J Surg Res 2012;176(1):79-83. https://doi.org/10.1016/j.jss.2011.09.049 [ Links ]
21. El Ghoneimi A, Valla JS, Limonne B, et al. Laparoscopic appendectomy in children: Report of 1,379 cases. J Pediatr Surg 1994;29(6):786-789. https://doi.org/10.1016/0022-3468(94)90371-9 [ Links ]
22. Ponsky TA, Huang ZJ, Kittle K, et al. Hospital- and patient-level characteristics and the risk of appendiceal rupture and negative appendectomy in children. JAMA 2004;292(16):1977-1982. https://doi.org/10.1001/jama.292.16.1977 [ Links ]
23. Alloo J, Gerstle T, Shilyansky J, Ein SH. Appendicitis in children less than 3 years of age: A 28-year review. Pediatr Surg Int 2004;19(12):777-779. https://doi.org/10.1007/s00383-002-0775-6 [ Links ]
24. Sakellaris G, Tilemis S, Charissis G. Acute appendicitis in preschool-age children. Eur J Pediatr 2005;164(2):80-83. https://doi.org/10.1007/s00431-004-1568-9 [ Links ]
25. Wu HP, Lin CY, Chang CF, Chang YJ, Huang CY. Predictive value of C-reactive protein at different cutoff levels in acute appendicitis. Am J Emerg Med 2005;23(4):449-453. https://doi.org/10.1016/j.ajem.2004.10.013 [ Links ]
26. Calvo RF, Sendra ES, Mialaret LA, et al The value of C-reactive protein in the diagnosis of acute appendicitis in children. An Esp Pediatr 1998;48(4):376-380. [ Links ]
27. Yang HR, Wang YC, Chung PK, Chen WK, Jeng LB, Chen RJ. Laboratory tests in patients with acute appendicitis. Aust N Z J Surg 2006;76(1-2):71-74. https://doi.org/10.1111/j.1445-2197.2006.03645.x [ Links ]
28. Andersson REB. Meta-analysis of the clinical and laboratory diagnosis of appendicitis. Br J Surg 2004;91(1):28-37. https://doi.org/10.1002/bjs.4464 [ Links ]
29. Yu CW, Juan LI, Wu MH, Shen CJ, Wu JY, Lee CC. Systematic review and meta-analysis of the diagnostic accuracy of procalcitonin, C-reactive protein and white blood cell count for suspected acute appendicitis. Br J Surg 2012;100(3):322-329. https://doi.org/10.1002/bjs.9008 [ Links ]
 Correspondence:
Correspondence:
S Montedonico
sandra.montedonico@uv.cl
Accepted 10 March 2017


{kind=link}
{kind=link}
{kind=link}
{kind=link}