










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSAMJ: South African Medical Journal
versión On-line ISSN 2078-5135
versión impresa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.107 no.9 Pretoria sep. 2017
http://dx.doi.org/10.7196/samj.2017.v107i9.12525
IN PRACTICE
MEDICINE AND THE LAW
Facilitating access to adolescent sexual and reproductive health services through legislative reform: Lessons from the South African experience
A StrodeI, II; Z EssackIII, IV, V
ILLM, PhD School of Law, University of KwaZulu-Natal, Pietermaritzburg, South Africa
IILLM, PhD HIV AIDS Vaccines Ethics Group (HAVEG), University of KwaZulu-Natal, Pietermaritzburg, South Africa
IIIMSS (Research Psychology), PhDSchool of Law, University of KwaZulu-Natal, Pietermaritzburg, South Africa
IVMSS (Research Psychology), PhDHIV AIDS Vaccines Ethics Group (HAVEG), University of KwaZulu-Natal, Pietermaritzburg, South Africa
VMSS (Research Psychology), PhD Human and Social Development Programme, Human Sciences Research Council, Pietermaritzburg, South Africa
ABSTRACT
South Africa (SA) has progressive legislation enabling adolescents to access various sexual- and reproductive-health services (SRH) independently, without consent from parents or legal guardians. This article reviews the SA legislative framework for adolescent access to SRH interventions. It outlines the five approaches adopted in current legislation to address adolescents' capacity to independently consent to specified health interventions, based on age, capacity and public policy requirements, or combinations thereof. Rather than subsume various health interventions under the umbrella of medical treatment, SA has separately legislated on many SRH interventions (e.g. HIV testing, contraceptives and terminations of pregnancy, among others). We identify strengths and weaknesses of the SA approach, and conclude with lessons learned from the SA experience which could inform discussion and debate on the most appropriate ways for countries to consider law reform that facilitates adolescent access to SRH services.
The South African (SA) Constitutional Court found that in certain specific circumstances, adolescents have a constitutional right to engage in sexual behaviour without incurring criminal sanctions. [1] This rights-based approach to adolescent sexuality is reflected in the recently revised Criminal Law (Sexual Offences and Related Matters) Amendment Act No. 32 of 2007 (hereafter the Sexual Offences Act). [2] The Sexual Offences Act provides that the age of consent to sex in SA is 16 years;[2] nevertheless, it also provides that adolescents aged 12 - 15 years old may engage in consensual sex with peers in the same age category (12 - 15 years) without criminal sanction.[2] Likewise, adolescents aged 12 - 15 may have sex with 16 - 17-year-olds, provided that there is no more than a 2-year age gap between them.[2] This new approach follows from the Constitutional Court's finding that sexual activity and exploration is part of normative development from adolescence to adulthood.[1,3]
The right to have sex at 16 must be understood in the context of the age at which adolescents can consent to a range of other sexual-and reproductive-health (SRH) services. This article uses the World Health Organization's (WHO's) definition of adolescents as young persons between the ages of 10 and 19.[4] Currently in SA, adolescents have the right to access five SRH services. These rights are expressly provided for in legislation (Table 1). The Children's Act No. 38 of 2005[5] states that children may consent independently to HIV testing, male circumcision, contraceptives (including contraceptive advice) and virginity testing at various points before the age of 18. The Choice of Termination of Pregnancy Act No. 92 of 2007'61 allows a woman (including a girl child) of any age to consent to a termination of pregnancy without assistance. The legal framework also refers to a number of general health rights which facilitate independent access to SRH services, including consent to medical treatment'[5] and scheduled drugs on the presentation of a prescription.[7] The only SRH service which adolescents <18 and their proxies are prohibited from consenting to is sterilisation.[8]
There have been increasing calls for legislative frameworks to enable adolescent access to SRH services.'[9] Reviewing the ages of consent to SRH services is considered one way of achieving this objective, as it enables an assessment of the extent to which the framework hinders or facilitates access to such services.[10] This article builds on earlier work which reviewed the ages of consent to various health interventions in SA.[11,12] It develops this preliminary work by critically interrogating the current SA legislative approach to the evolving capacity of adolescents to consent to SRH services. SA provides a good case study on adolescent SRH, given the extensive law reform relating to SRH over the last 2 decades.
The article reviews the SA legislative framework and discusses the strengths and weaknesses of the SA approach. It identifies lessons that can be learned from SA's legislative approach that could inform discussion and debate on the most appropriate ways for countries to consider law reform that facilitates adolescent access to SRH services.
Potential legal barriers to adolescents' access to SRH services
Adolescents' right to engage in sexual intercourse, and the imperative to address potential legal barriers to accessing SRH services, is set within the context of their many health risks. SA adolescents are at risk of HIV, sexually transmitted infections and pregnancy owing to high-risk sexual behaviour, physical, social and structural challenges, and limited access to key primary SRH services,[13] among other factors. Approximately 30% of teenagers (aged 13 - 19 years) in SA report ever being pregnant,'141 and in 2013, Statistics SA[15] reported that 99 000 school-going adolescent girls were pregnant. The most recent National HIV Prevalence, Incidence and Behaviour Survey found an HIV prevalence of 7.1% for youth aged 12 - 24 years.[16] The HIV incidence among young women (15 - 24 years old) is particularly alarming, with 113 000 new infections annually, four times higher than that of their male peers.[16]
Laws permitting independent consent to SRH services are an important mechanism to ensure accessible services for adolescents. It is argued that requiring parental permission may deter adolescents from accessing SRH services,[17] including HIV testing.[18] For example, an empirical study in Connecticut, USA found that a significantly higher proportion of adolescents volunteered for HIV testing once the parental consent requirement was abolished.[19] Parental consent may be a barrier to adolescents' accessing services for several reasons, such as that adolescents may not wish to disclose their sexual activity to their parents.[20,21] Commentators have reported that the most common reason for non-disclosure to parents appears to be a concern for the parents' feelings, including a fear of disappointment or embarrassment and expected negative results, such as physical punishments or other forms of retaliation.[19] In the SA context, the requirement for parental consent is also problematic for those adolescents who do not live with their parents (e.g. child-headed households or children living with other caregivers).
Parental consent is not the only potential legal barrier to adolescent access to SRH services. Disparate approaches to the ages at which children can consent to sex and make use of SRH services can be a problem.[9'22'23] Previously in SA, the Children's Act[5] enabled adolescent access to a range of SRH services, while the Sexual Offences Act[2] continued to criminalise underage sex. This hindered access because children who used such services could be reported to the police.[23] This was compounded by the requirements in the Sexual Offences Act that any person with 'knowledge' of a sexual offence against a child (including a consensual offence) had to report it.[23,24]
The legal framework dealing with access to SRH services in SA
The primary principle on which access to SRH services is based is the capacity to consent, as this is an essential element of informed consent. Consent can only be provided by a person with the 'intellectual and emotional capacity for the required knowledge, appreciation and consent'.[25] Furthermore, the 'capacity to consent depends on the ability to form an intelligent will on the basis of an appreciation of the nature and consequences of the act consented to'.[25]
In SA law, children are considered minors until the age of 18, and do not have the capacity to make legally binding decisions. However, in line with their evolving capacity, the legislature has expressly described a number of SRH rights that are applicable to adolescents. There are eight SRH and related rights which have a range of consent requirements based on age, capacity and/or public policy criteria (Table 1).
The legislature appears to view access to contraceptives as requiring the least capacity and consent, with sterilisations requiring the most. Age 12 also marks the beginning of many of the SRH rights, despite this being 2 years after the age at which the WHO views adolescence as having started. Nevertheless, this is in line with criminal law, which provides that adolescents under the age of 12 do not have the capacity to consent to sex,[2] as discussed below.
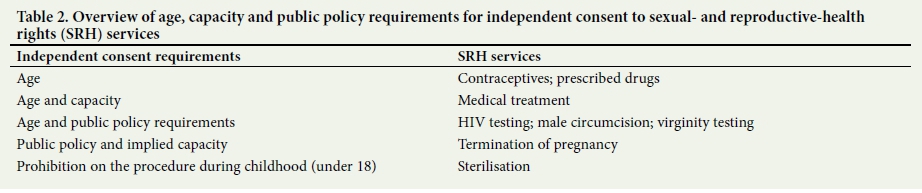
An examination of the capacity requirements suggests that the legislature has used five broad approaches to addressing adolescent capacity to consent to SRH services (Table 2). The first approach only sets an age requirement. Consent to contraceptives and contraceptive advice may be provided to a child from the age of 12,[5] prescribed drugs from 14,[7] and sterilisations from 18.[8] Children are also able to consent to sex from the age of 16.[2] This approach presumes that a child of the specified age has the capacity to consent.[26]
The second approach requires both age and an express capacity requirement. Medical treatment is the only intervention that requires the child to be 12 years and older, and to have 'sufficient maturity' and the 'mental capacity to understand the benefits, risks, social and other implications of the treatment'.[5] This means that a child must be developmentally sufficiently mature to consent, and able to weigh up the various important factors that must be considered.
The third approach combines age and an express public policy requirement. HIV testing, male circumcision and virginity testing require a child to be a certain age and for a certain public policy norm to be satisfied. For HIV testing, the adolescent must be 12 years or older, and the test must be in their 'best interests' and be accompanied by counselling.[5] For male circumcision and virginity testing, adolescents must be 16 years or older and receive 'proper counselling'.[5]
The fourth approach requires only an express public policy requirement. For terminations of pregnancy, there are no specified age or capacity requirements, but the healthcare worker performing the procedure must 'advise such minor to consult with her parents, guardian, family members or friends before the pregnancy is terminated'.[6]
The fifth approach is a complete prohibition of the service for adolescents under the age of 18. Sterilisations are the only SRH service which may not be offered to persons under the age of 18, even with proxy consent.[8] Older adolescents, aged 18 - 19 years, can, however, consent to a sterilisation.
Discussion
To its credit, SA expressly identifies an age of consent to sex. Importantly, the age of consent applies equally to boys and girls, and does not discriminate based on sexual orientation. Further, recent law reform increases the protection of adolescents, as it ensures that children below the age of consent (12 - 15-year-olds) who have consensual sex with their peers will not face criminal sanction.[2] A key barrier to accessing SRH services is concern about confidentiality - but since service providers are now absolved of reporting consensual sex in certain age categories to authorities, this may improve the uptake of these services.[27]
International guidelines recommend that legislators ensure that adolescents can consent independently to medical treatment before the age of 18.[28] SA has addressed this issue by creating both an age and a capacity requirement for consent to medical treatment (Table 1). The age requirement of 12 years is moderated by the capacity requirement of 'sufficient maturity'. The advantage of this approach is that it does not treat all forms of medical treatment alike, as it assumes that more complex forms of treatment may require greater capacity. This approach of having a low age of consent, but introducing a capacity requirement, is an inversion of the principle established in Gillick v West Norfolk and Wisbeck Area Health Authority and the DHSS 1985,[29] where the court held that children under the age of 16 years (the age of consent to medical treatment in the UK) did not lack legal capacity to make their own decisions by age alone. They had the capacity to make such decisions when they had sufficient understanding and intelligence to fully understand what was proposed.[29]
SA has also elected to deal with consent to accessing prescribed drugs, contraceptives, HIV testing and male circumcision separately from medical treatment. In many other countries, these would be subsumed within a broad definition of medical treatment.[8] Separating these services has allowed for specific and different obligations to be put in place in relation to each service (Table 1). The only SRH service which could arguably form part of medical treatment that adolescents under the age of 18 are expressly excluded from consenting to is sterilisation. This is an important and appropriate protective mechanism, given that the WHO[28] does not ordinarily recommend that the procedure be carried out before a person is 30 years old.
Despite this liberal approach, some key concerns remain. Firstly, there remains some disjuncture between the approach in criminal and children's law pertaining to adolescents: when there is more than a 2-year age gap between older (16 - 17 years) and younger (12 - 15 years) adolescents who engage in consensual sex with each other, both parties could still be prosecuted.[3] This has a disparate impact on girls, who are more likely to have older partners.[16] Where such cases are reported, young girls may be required to testify against their older partners, which may result in social harm to them.[3] Furthermore, the legislature retained the strict mandatory reporting requirements, and as a result, if adolescents declare that they have older partners whilst seeking SRH services, this information would have to be reported to the police.[3,27]
Secondly, the legal framework only recognises SRH rights for adolescents over the age of 12 years. This ensures that there is consistency between criminal and children's law in this regard, as the Sexual Offences Act provides that adolescents below the age of 12 do not have the capacity to consent to sex.[2] However, it also means that the Act is not in sync with the WHO approach or with recent empirical research showing that children aged 10 - 11 have the capacity to consent to medical research.[31,32] It is argued that many research-related decisions would be similar to SRH choices.
Thirdly, incorporating capacity requirements into consent norms has its disadvantages, including in terms of how best to assess capacity.[11] Commentators recommend that assessing 'sufficient maturity', for example, involves ensuring that the adolescent understands the risks, benefits and implications of the SRH services.[18] Such assessments should also consider the adolescent's circumstances at the time, including their age, knowledge, experience and judgement.[18]
Fourthly, the Children's Act[5] does not define medical treatment, and this has left some uncertainty regarding new forms of HIV prevention, such as vaccines and microbicides. If these HIV-prevention methods are registered in future, it is unclear whether adolescents will be able to access them as a form of medical treatment.
Fifthly, the Children's Act[5] has legitimated the cultural practice of virginity testing. The Act allows girls who are over the age of 16 years to consent to be physically examined to establish whether they are virgins.[5] Mubangizi[33] argues that by making this customary practice lawful in certain circumstances, children's rights to privacy, bodily integrity and dignity are being violated. These provisions are out of step with the pro-children's rights approach to other SRH interventions.
Finally, SA has adopted a novel approach by linking public-policy requirements to consent for four SRH services: HIV testing, male circumcision, terminations of pregnancy and virginity testing. Public-policy requirements can serve to strengthen protection for adolescents generally. However, the HIV-testing standard, which requires the test to be in the best interests of the child, has been criticised as being unwieldy and a barrier to HIV testing.[18]
Conclusion
Post-apartheid SA has created a comprehensive SRH-rights framework for adolescents. The SA framework is different from that of many other countries, as it has legislated separately on many SRH services rather than simply creating a blanket age of consent to medical treatment. It has also introduced a number of protective public-policy measures to ensure that children are supported in making SRH decisions.
There are several lessons that can be learned from the SA legislative experience. Firstly, legislating on the ages of consent to SRH services creates a framework within which youth-friendly services can be designed and implemented.
Secondly, progressive new legislation that has decriminalised certain categories of underage consensual sex enables services to be provided in an accessible manner without state sanction. The age of consent to sex should not be a barrier to accessing SRH services. This requires that countries ensure harmony between the ages of consent to sex, medical treatment and any other SRH services, such as HIV testing.
Thirdly, specifying that access to contraceptives, HIV testing and male circumcision fall outside the area of medical treatment creates clarity regarding the capacity requirements for each of these interventions. Countries are encouraged to follow this nuanced approach. If this is not possible, they should, at a minimum, provide that children can consent to medical treatment below the age of 18, and clarify the issue of specific SRH services through policies and regulations.
SA has made a disputed cultural practice into a lawful SRH service. Other countries should be very cautious regarding this approach, and should carefully consider the value of this type of legal provision vis-a-vis the protection of children.
Finally, as described, SA has a divergent approach to the evolving capacity of adolescents, with some anomalies. Careful consideration should be given to the capacity requirements for each intervention, in order to ensure that there is consistency in any legislative approach. Pragmatic guidance for service providers on how to assess capacity should also be drafted.
In conclusion, SRH research with adolescents is critically important, but must occur alongside efforts to ensure that the legal framework is conducive to facilitating access to such improved services and products.
Acknowledgements. The authors would like to thank reviewers for their helpful comments on this manuscript.
Author contributions. AS conceptualised the paper. AS and ZE both contributed to the content of the paper and revisions of drafts.
Funding. The work described here was supported by the SA AIDS Vaccines Initiative (SAAVI) and the National Institutes of Health award (1RO1 A1094586) CHAMPS (Choices for Adolescent Methods of Prevention in SA). The content is solely the responsibility of the authors and does not necessarily represent the official views of SAAVI or the National Institutes of Health. This paper does not necessarily reflect the views of any institution or committee or council with which the authors are affiliated.
Conflict of interest. None.
References
1. Teddy Bear Clinic for Abused Children, and Resources Aimed at the Prevention of Child Abuse and Neglect (RAPCAN) v Minister Of Justice And Constitutional Development And Another 2012 (Case Number 73300/10). [ Links ]
2. Department of Justice and Constitutional Development, South Africa. Criminal Law (Sexual Offences and Related Matters) Amendment Act No. 32 of 2007. [ Links ]
3. Bhamjee S, Essack Z, Strode AE. Amendments to the Sexual Offences Act dealing with consensual underage sex: Implications for doctors and researchers. S Afr Med J 2016;106(3):256-259. https://doi.org/10.7196/samj.2016.v106i3.9877 [ Links ]
4. Sacks D, Canadian Pediatric Society. Age limits and adolescents. Paediatr Child Health 2003;8(9): 577. [ Links ]
5. South Africa. Children's Act No. 38 of 2005. [ Links ]
6. South Africa. Choice of Termination of Pregnancy Act No 92 of 2007. [ Links ]
7. South Africa. Medicines and Related Substances Control Amendment Act No. 90 of 1997. [ Links ]
8. South Africa. Sterilisation Act No. 44 of 1998. [ Links ]
9. United Nations Development Programme. Global commission on HIV and the law: Risk, rights and health. New York: UNDP, 2012. [ Links ]
10. Joint United Nations Programme on HIV/AIDS (UNAIDS). All In To #EndAdolescentAIDS. Geneva: UNAIDS, 2015. [ Links ]
11. Strode A, Slack C, Essack Z. Child consent in South African law: Implications for researchers, service providers and policy-makers. S Afr Med J 2010;100(4):247-249. [ Links ]
12. Strode A, Slack C, Essack Z. Child consent in South African law - implications for researchers, service providers and policy-makers. S Afr Med J 2011;101(9):604-606. [ Links ]
13. Beksinska ME, Pillay L, Milford C, Smit JA. The sexual and reproductive health needs of youth in South Africa - history in context. S Afr Med J 2014;104(10):676-678. https://doi.org/10.7196/SAMJ.8809 [ Links ]
14. Willan S. A review of teenage pregnancy in South Africa - experiences of schooling, and knowledge and access to sexual & reproductive health services. Partners in Sexual Health 2013:1-63. [ Links ]
15. Stats SA. General household survey. Statistical release P0318. 2012;318:1-164. [ Links ]
16. Shisana O, Rehle T, Simbayi LC, et al. South African National HIV Prevalence, Incidence and Behaviour Survey, 2012. Cape Town: HSRC Press, 2014. [ Links ]
17. Wood K, Jewkes R. Blood blockages and scolding nurses: Barriers to adolescent contraceptive use in South Africa. Reprod Health Matters 2006;14(27):109-118. https://doi.org/10.1016/S0968-8080(06)27231-8 [ Links ]
18. Van Rooyen HE, Strode AE, Slack CM. HIV testing of children is not simple for health providers and researchers: Legal and policy frameworks guidance in South Africa. S Afr Med J 2016;106(5):451-453. https://doi.org/10.7196/samj.2016.v106i5.10484 [ Links ]
19. Jackson S, Hafemeister TL. Impact of parental consent and notification policies on the decisions of adolescents to be tested for HIV. J Adolesc Health 2001;29(2):81-93. https://doi.org/10.1016/S1054-139X(00)00178-6 [ Links ]
20. Delany-Moretlwe S, Cowan FM, Busza J, Bolton-Moore C, Kelley K, Fairlie L. Providing comprehensive health services for young key populations: Needs, barriers and gaps. J Int AIDS Soc 2015;18(Suppl 1):S29. https://doi.org/10.7448/IAS.18.2.19833 [ Links ]
21. Moodley N, Gray G. Global evidence reaffirms the case for routine HPV and potential HIV adolescent vaccination in South Africa. Future Virol 2014;9(2):207-220. https://doi.org/10.2217/fvl.13.131 [ Links ]
22. Strode A, Toohey J, Slack C, Bhamjee S. Reporting underage consensual sex after the Teddy Bear case: A different perspective. S Afr J Bioeth Law 2013;6(2):45-47. https://doi.org/10.7196/SAJBL.289 [ Links ]
23. Strode A, Slack C. Sex, lies and disclosures: Researchers and the reporting of under-age sex. S Afr J HIV Med 2009;10(2):8-10. [ Links ]
24. Essack Z, Strode A. The mandatory reporting of consensual, underage sex: Knowledge, practices and perspectives of social workers in KwaZulu-Natal. S Afr J Bioeth Law. 2015;8(2):21-25. https://doi.org/10.7196/SAJBL.435 [ Links ]
25. Christian Lawyers Association v Minister of Health and Others (Reproductive Health Alliance as Amicus Curiae) 2005 (1) SA 509 (TDP). [ Links ]
26. Van Wyk C. HIV preventative vaccine research on children. Is it possible in terms of South African law and research guideline? Tydskrif vir Hedendaagse Romeins-Hollandse Reg 2005;68:35-50. [ Links ]
27. Essack Z, Toohey J, Strode A. Reflecting on adolescents' evolving sexual and reproductive health rights: Canvassing the opinion of social workers in KwaZulu-Natal, South Africa. Reprod Health Matters 2016;24(47):195-204. https://doi.org/10.1016/j.rhm.2016.06.005 [ Links ]
28. United Nations General Assembly. Convention on the Rights of the Child. Geneva: UN, 1989. [ Links ]
29. Gillick v West Norfolk and Wisbeck Area Health Authority and the DHSS, 1985 (3) All England Law Reports 402. House of Lords. [ Links ]
30. World Health Organization. Reproductive Health. Medical eligibility criteria for contraceptive use. Geneva: WHO , 2010. [ Links ]
31. Hein IM, Troost PW, Lindeboom R, et al. Accuracy of the MacArthur competence assessment tool for clinical research (MacCAT-CR) for measuring children's competence to consent to clinical research. JAMA Pediatr 2014;168(12):1147-1153. https://doi.org/10.1001/jamapediatrics.2014.1694 [ Links ]
32. Nelson LR, Stupiansky NW, Ott MA. The influence of age, health literacy, and affluence on adolescents' capacity to consent to research. J Empir Res Hum Res Ethics 2016;11(2):115-121. https://doi.org/10.1177/1556264616636232 [ Links ]
33. Mubangizi JC. A South African perspective on the clash between culture and human rights, with particular reference to gender-related cultural practices and traditions. J Int Womens Studies 2012;13(3):33. [ Links ]
 Correspondence:
Correspondence:
A Strode
StrodeA@ukzn.ac.za
Accepted 8 June 2017


{kind=link}
{kind=link}