










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSAMJ: South African Medical Journal
versión On-line ISSN 2078-5135
versión impresa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.107 no.8 Pretoria ago. 2017
http://dx.doi.org/10.7196/samj.2017.v107i8.12034
RESEARCH
Suicide in Pretoria: A retrospective review, 2007 - 2010
C EngelbrechtI; R BlumenthalII; N K MorrisIII; G SaaymanIV
IMSc (MedCrim); Department of Forensic Medicine, Faculty of Health Sciences, University of Pretoria, South Africa
IIMB ChB, MMed (MedForens), FCForPath (SA), PhD; Department of Forensic Medicine, Faculty of Health Sciences, University of Pretoria, South Africa
IIIMSc (MedCrim); Department of Forensic Medicine, Faculty of Health Sciences, University of Pretoria, South Africa
IVMB ChB, MMed (MedForens), FCForPath (SA) Department of Forensic Medicine, Faculty of Health Sciences, University of Pretoria, South Africa
ABSTRACT
BACKGROUND. The World Health Organization has declared suicide a global health crisis, predicting that ~1.53 million people will commit suicide annually by 2020.
OBJECTIVE. A study from South Africa reviewed 1 018 suicide cases in Pretoria over 4 years (1997 - 2000). Our study was undertaken to establish whether there have been substantial changes in the profile of suicide victims who died in Pretoria a decade later.
METHODS. Case records at the Pretoria Medico-Legal Laboratory were reviewed retrospectively from 2007 to 2010.
RESULTS. A total of 957 suicide cases were identified. Hanging was the most common method of suicide, followed by self-inflicted firearm injury. The true incidence of suicidal intake of prescription drugs/medication was difficult to determine, because of a backlog at the state toxicology laboratories. White males and females appeared to be over-represented among suicide victims, but there has been an increase in suicide among blacks. There seems to have been a substantial decrease in the use of firearms to commit suicide - possibly reflecting a positive outcome of gun control legislation that has been introduced in the interim.
CONCLUSION. Suicide continues to constitute almost 10% of all fatalities admitted to the Pretoria Medico-Legal Laboratory, confirming suicide as a major cause of mortality in our society. Further research is needed to clarify the profile of suicidal deaths, with a view to informing resource allocation and to improve preventive strategies.
Background
Suicide is a major public health problem - the main cause of unnatural death in some countries - and was declared a global health crisis by the World Health Organization in 1994.[1-5] It has been estimated that by 2020 ~1.53 million people will commit suicide annually.[6-8] Globally, suicide rates reported for 2009 range from 71.7/100 000 of the population (Lithuania) to 0.1/100 000 (Egypt).[5] The suicide rate for South Africa (SA) in 2007 was reported as 1.8/100 000.[5] More specifically, a suicide rate of 25/100 000 was reported for Pretoria, the capital city of SA, from 1997 to 2000.'91 In the past 7 years research has been published on the profile of suicide in SA and Africa.[10-14]
Most studies have shown that males commit suicide more often than females and that men tend to use more 'violent' methods.[1,5,9,11,15-18] However, Scribante et al.[9]reported a remarkably high incidence of suicide by firearms among women in Pretoria for 1997 - 2000. Hanging is the most common method of committing suicide in most countries.[1,11,15,16,19-20] This is also the case in SA, followed by the use of firearms and (self) poisoning.[15-17,20] In contrast, Scribante et al.'9 reported that self-inflicted gunshot wounds were the most common method of committing suicide in Pretoria. Other relatively common methods include medication overdose, gassing (i.e. the use of carbon monoxide and nitrogen), jumping from a height, stabs and cuts, and self-immolation.[9,10,21,22]
Objectives
In view of the global and SA increase in the incidence of suicide and the unusual findings previously reported for Pretoria, a follow-up study was undertaken to assess the profile of suicide in this city to compare the findings with those reported some 10 years earlier.[7,9] Despite becoming a non-racial democracy in 1994, SA remains a country with many sociopolitical and economic problems; it has been reported to be the country with the highest crude death rate and one of the highest non-natural death rates in the world.[23]
Methods
Case records at the Pretoria Medico-Legal Laboratory (PMLL) for January 2007 - December 2010 were reviewed retrospectively. The study was approved by the Faculty of Health Sciences Research Ethics Committee, University of Pretoria (ref. no. 76/2013).
The study was not designed to establish the epidemiological profile and incidence of suicide according to the relevant population denominators for Pretoria. As part of the statutory routine medico-legal investigation of the death process, all unnatural deaths in Pretoria, whether homicide, suicide, accident, natural or undetermined, are admitted to the PMLL. The case files of deceased persons admitted to the PMLL are contemporaneously assessed by the attending forensic medical practitioner (FMP), usually in conjunction with investigating police officers and by making use of information gathered at the scene of death, as well as by considering the medical history and information provided by witnesses (including family members). After completing the autopsy, a preliminary opinion is then given by the FMP responsible for the case as to the probable manner of death (homicide, suicide, accident, natural or undetermined). However, the classification of a particular case as, for example, homicide or suicide, will ultimately be the function and prerogative of the SA Police Service (SAPS), usually in conjunction with the director of public prosecutions or the inquest court magistrate (as provided for by the Inquests Act of 1959). For the purpose of this study, all cases contemporaneously identified by the FMP responsible for the autopsy as being probably due to suicide, were included. Where suicidal action or intent was not deemed clear or probable, the case was excluded from our study.
In this study, race was used for comparison; race classification was also used in the article by Scribante et al.[9]Race classification was included because it deviates from our norm. The race of suicide victims was identified by how it was presented in the case files, either by their identification (ID) books or by family members, only where the victim was unknown did the investigator use the race as identified by the FMP during the autopsy.
Results
Over the 4-year-span from 2007 to 2010, 9 379 cases were admitted to the PMLL for investigation. Of these, 957 were due to suicide, thus constituting 10.2% of the total case load over the study period. Among the suicide victims, there were 731 (76.4%) males and 226 (23.6%) females. Although racial profiling may be problematic and contentious, 447 (46.7%) victims were black, while 477 (49.8%) were grouped as being white, reflecting a ratio of 1:1.07 (Fig. 1). There were only 33 (3.5%) victims who were of Asian race or mixed racial descent.

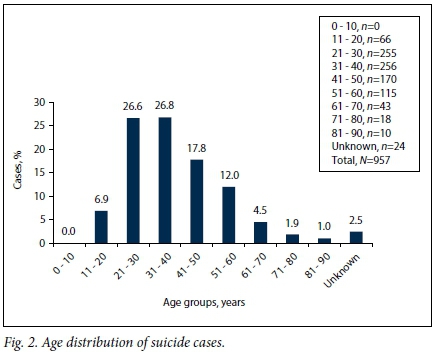
The ages of the victims ranged from 14 to 88 years, with a mean of 38.31 years. The highest number of victims fell within the age groups 21 - 30 years and 31 - 40 years (Fig. 2). The youngest age group (11 -20 years) comprised 66 victims, including, inter alia, the following age profiles: 14-year-olds (n=2), 15-year-olds (n=7), 16-year-olds (n=9), 17-year-olds (n=11) and 18-year-olds (n=14).
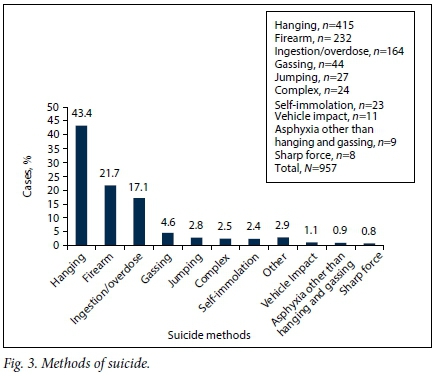
In most cases (97.5%) only one method of suicide was apparent, the single most common method being hanging, accounting overall for 415 (43.4%) cases, followed by 232 (24.2%) firearm fatalities and 164 (17.1%) ingestion/overdose cases (Fig. 3). Cases of drowning and suffocation were classified as asphyxial deaths, but hangings and gassings were excluded from that category. Complex suicide (where more than one method was used, e.g. ingestion of medication followed by a gunshot wound) was recorded in 24 (2.5%) cases.
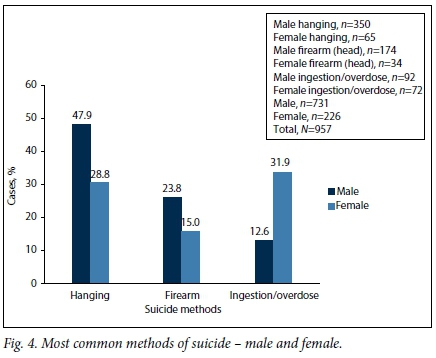
Although the top three methods of suicide were the same among men and women, the order differed, the preferred method among males being hanging, while in women ingestion/overdose was the most common (Fig. 4).
When the data are disaggregated by race and gender, interesting trends appear: 62% of black males who committed suicide did so by hanging, while white males most commonly shot themselves (124; 33.3%). Black females rarely committed suicide (73; 7.6%), of whom most (28; 38.4%) hanged themselves, while white females (144; 15%) most commonly died from ingestion/overdose (45; 31.3%). Among victims of Asian and mixed racial descent, hanging was the most common method of suicide.
Blood was analysed for alcohol in 885 (92.5%) cases; of these, 459 (51.9%) were found to be negative. Among those with positive values, the average blood alcohol concentration was 0.06 g/100 mL, the highest recorded value being 0.92 g/100 mL.
Of the cases where additional information was provided by the next of kin, the following was revealed: 400 (41.8%) of the victims were employed and 165 (17.2%) were unemployed, while in 309 (32.3%) of cases no reliable information regarding employment status was available. There were 39 (4.1%) students and scholars among the victims, and 44 (4.6%) pensioners. Of those who were employed, 40 (10%) were members of SAPS or the SA National Defence Force (SANDF). Of the 957 cases in the study population, 17 (1.8%) committed suicide while in custody, and only 3 (0.3%) victims were from a psychiatric hospital or similar institution.
In total, 329 (34.4%) victims were reported to have been married at the time of their death, 470 (49.1%) were single, 89 (9.3%) were divorced and 30 (3.1%) were widows/widowers. In 39 (4.1%) cases no marital status was recorded. In 20 (2.1%) cases, the suicide was recorded as having been part of a dyadic death (homicide-suicide event). In five of these latter cases the suicide victims (perpetrators) were members of the police or defence force. In only 12 (1.3%) cases information of a previous attempted suicide was forthcoming. In 123 (12.9%) cases the presence of a suicide note was recorded.
Of 957 suicide victims, 24 (2.5%) remained unidentified after medico-legal investigation.
Discussion
The 957 suicide victims (of a total of 9 379 bodies admitted to the PMLL over the study period) constitute 10.2% of the total number of admissions - differing only marginally from the 9.7% reported by Scribante et al.[9]for the study period of a decade earlier. Most of the victims were, once again, males, with a ratio of 3:1 male to female (again similar to the data collected for 1997 - 2000).[9,24,25]! When population groups and gender are juxtaposed, a distinct over-representation of white males is noted, with ~25% of all such admissions to the mortuary being suicide victims, while only 9% of black males were admitted because of suicide. Similarly, ~27% of white females admitted to the mortuary were victims of suicide, while only 5% of black female admissions were because of suicide.[9]
The overall population of Pretoria comprises ~75% blacks, ~22% whites and ~3% people of Asian origin and mixed racial descent. These figures (ratios) are also reflected in the total admissions to PMLL (i.e. unnatural deaths from all causes).1251 However, the finding that there are almost equal numbers of suicide victims among white and black population groups suggests that suicide is much more prevalent among white persons. Nevertheless, there has been an increase in the proportion of black suicide victims compared with that in Scribante et al's[9] study, indicating that suicide may be increasing among blacks. The increase in black suicide victims is also mentioned in the article by Naidoo and Schlebusch,1121where research was done on suicide in Durban, KZN, another province of SA. More detailed research is required in this area.
This study supports the findings of Scribante et al.[9]with regard to the age groups at greatest risk for suicide. In our study, 53.4% of victims were aged between 21 and 40 years, in contrast to reported findings that global suicide rates are highest in people aged >70 years, but correlating with the reported finding that in low- and middle-income countries young adults and elderly women have higher rates of suicide than their counterparts in high-income countries.[13,15,16,,24]Notably, suicide is the second leading cause of death in 15 - 29-year-olds globally.[11]The youngest victim in our study was 14 years old.
Comparing our findings with Scribante et al.'s[9] data published 10 years ago, the latter reveals a major decline in suicides by firearm, but a sharp increase in hanging. There was also an increase in suicide from ingestion/overdose, but a decrease in the number of gassings. What may be of particular significance, is that the Firearms Control Act (Act No. 1 of 2000) came into effect in 2004, together with its subsidiary regulations. These laws put in place stringent criteria and strict procedural prescriptions with regard to the obtaining and possession of firearms. Previous studies have indicated that the introduction of such statutory measures is associated with a decline in firearm-related suicide (but not necessarily with firearm-related homicides).[26] Therefore, it may be argued that the introduction of firearm control legislation has positively impacted on the use of such weapons in committing suicide, but it is debatable whether this has had an effect on the overall incidence of suicide.
Jumping from a height, self-immolation and sharp force injury accounted for a small number of suicide victims in our study. Suicidal deaths from road traffic crashes/incidents and drowning are difficult to classify reliably as being due to suicide, and require greater reliance on other sources of information.
Previous studies have drawn attention to differences between suicide methods in relation to race and gender.[6,9,10,15,27] This was also observed in our study, but distinct differences seemed to emerge when compared with the data of Scribante et al.[9] In our study, black females were more likely to hang themselves, in contrast to the reported findings of self-immolation as the (previously) preferred method of suicide among this group. Nonetheless, white females were now more likely to commit suicide by ingestion or overdosing, as opposed to the finding that a decade ago the preferred method of suicide was firearm injury.[9] Our study, however, further confirms the relatively high incidence of firearm-related suicide among white women in Pretoria.
While 10 years ago the use of prescription medication was preferred in cases of ingestion/overdose, this study shows that the intake of agrochemicals, such as insecticides and pesticides, is now more common.[9] This may be in keeping with their widespread use and ready availability, especially of pesticides in certain communities.[28]
Alcohol was documented to be present in 43.5% of our cases, with an average blood alcohol concentration of 0.06 g/100 mL, which is consistent with that in the previous study.191 According to Jones et al.,[3] ethanol intoxication is a common finding at autopsy in suicide cases, perhaps because such intoxication results in poor judgement, less inhibition, poor self-control and impulsive behaviour - all of which may predispose to suicide in vulnerable individuals.
Jones et al.[3]stated that information related to e.g. marital status and employment shed light on a possible reason for the suicide, but we could not verify this. An interesting observation is that 25% of dyadic death incidents were committed by members of the SAPS and SANDF. This appears to be in keeping with data published by Jena et al.[29]in 2009 for dyadic deaths in Pretoria, from 1997 to 2001. Our study had a number of limitations. Firstly, there were changes to the geographical feeding area/catchment area of the mortuaries in the greater Pretoria area; an epidemiological profile could consequently not be created. Secondly, some of the suicide cases could have been omitted because the suicidal action or intent was not deemed clear or probable. Lastly, some toxicology information was still outstanding when this research was done.
Conclusion
These results show that the incidence of suicide as a percentage of the caseload at the PMLL has remained almost unchanged over the past decade (~10%).[9] However, significant changes appear to have taken place with regard to the methods used, with a substantial decrease in firearm-related suicides, but with an apparent parallel increase in hangings. The possibility exists, as mentioned in the article by Matzopoulos et al.,[26]that the latter may reflect changes brought about by the introduction of the Firearms Control Act No. 1 of 2000 in the interim period, but this needs to be studied further. White males continue to be heavily over-represented as victims of suicide in Pretoria, but suicidal deaths currently appear to constitute an increasing percentage of deaths among black people admitted to the PMLL. More studies are needed, especially taking into account population denominators, to further expose the profile of suicide as a cause of death in our society.
Acknowledgements. None.
Author contributions. Each of the authors made a substantial contribution to the following areas: (i) conception and design, acquisition of data, or analysis and interpretation of data; (ii) drafting the article or revising it critically for important intellectual content; and (iii) final approval of the version to be published.
Funding. One of the authors (CE) was the recipient of a study grant from the National Research Foundation (NRF). Opinions expressed and conclusions arrived at are those of the authors and do not necessarily reflect the views of the NRF.
Conflicts of interest. None.
References
1. World Health Organization. Suicide rates per 100 000 by country, year and sex. Geneva: WHO, 2011. [ Links ]
2. Ajdacic-Gross V, Weiss M, Ring M, et al. Methods of suicide: International suicide patterns derived from the WHO mortality database. Bull World Health Organ 2008;86(9):726-732. http://dx.doi.org/10.2471/BLT.07.043489 [ Links ]
3. Jones AW, Holmgren A, Ahlner J. Toxicology findings in suicides: Concentrations of ethanol and other drugs in femoral blood in victims of hanging and poisoning in relation to age and gender of the deceased. J Forensic Leg Med 2013;20(7):842-847. http://dx.doi.org/10.1016/j.jflm.2013.06.027 [ Links ]
4. Zupanc T, Agius M, Paska AV, Pregelj P. Blood alcohol concentration of suicide victims by partial hanging. J Forensic Leg Med 2013;20(8):976-979. http://dx.doi.org/10.1016/j.jflm.2013.09.011 [ Links ]
5. Office of Disease Prevention and Health Promotion, US Department of Health and Human Services. Mental health and mental disorders. 2012. www.healthypeople.gov/2020/topicsobjectives2020/objectiveslist.aspx?topicId=28 (accessed 23 May 2017). [ Links ]
6. Bertolote JM, Fleischmann A. A global perspective in the epidemiology of suicide. Suicidologi 2002;7(2):6-8. http://dx.doi.org/10.5617/suicidologi.2330 [ Links ]
7. World Health Organization. Preventing Suicide: A Global Imperative. Geneva: WHO, 2014:1-141. [ Links ]
8. South African Federation for Mental Health. World Suicide Prevention Day. 2015. http://www.safmh.org.za/ (accessed 19 June 2017). [ Links ]
9. Scribante L, Blumenthal R, Saayman G, Roos JL. A retrospective review of 1 018 suicide cases from the capital city of South Africa for the period 1997 - 2000. Am J Forensic Med Pathol 2004;25(1):52-55. http://dx.doi.org/10.1097/01.paf.0000113862.03302.1d [ Links ]
10. Stark K, Joubert G, Struwig M, et al. Suicide cases investigated at the state mortuary in Bloemfontein, 2003 - 2007. S Afr Fam Pract 2010;52(4):332-335. http://dx.doi.org/10.1080/20786204.2010.10874001 [ Links ]
11. Mars B, Burrows S, Hjelmeland H, Gunnell D. Suicidal behaviour across continent: A review of the literature. BMC Public Health 2014;14(1):606-620. http://dx.doi.org/10.1186/1471-2458-14-606 [ Links ]
12. Naidoo SS, Schlebusch L. Sociodemographic characteristics of persons committing suicide in Durban, South Africa: 2006 - 2007. Afr J Prim Health Care 2014;6(1):568-575. http://dx.doi.org/10.4102/phcfm.v6i1.568 [ Links ]
13. Van Niekerk L, Scribante L, Raubenheimer PJ. Suicidal ideation and attempt among South African medical students. S Afr Med J 2012;102(6):372-373. http://dx.doi.org/10.7196/samj.5503 [ Links ]
14. Medical Research Council. A profile of fatal injuries in South Africa. Seventh annual report of the National Injury Mortality Surveillance System 2005. http://www.mrc.ac.za/crime/national2005.pdf (accessed 19 June 2017). [ Links ]
15. Schlebusch L. Depression and suicide. S Afr Fam Pract 2005;47(5):61-63. [ Links ]
16. Seedat M, Ratele K, van Niekerk A, Sukhai A. A profile of fatal injuries in Gauteng 2010. Cape Town: Medical Research Council, 2012. [ Links ]
17. Pitman A, Krysinska K, Osborn D, King M. Suicide in young men. Lancet 2012;379(9834):2383-2392. http://dx.doi.org/10.1016/S0140-6736(12)60731-4 [ Links ]
18. Hawton K, van Heeringen K. Suicide. Lancet 2009;373(9672):1372-1381. http://dx.doi.org/10.1016/S0140-6736(09)60372-X [ Links ]
19. Chestnov O. Public Health Action for the Prevention of Suicide. Geneva: World Health Organization, 2012; 2-21. [ Links ]
20. Meel BL. Determinants of suicide in the Transkei sub-region of South Africa. J Clin Forensic Med 2003;10(2):71-76. http://dx.doi.org/10.1016/S1353-1131(03)00038-5 [ Links ]
21. Panczak R, Geissbühler M, Zwahlen M, Killias M, Tal K, Egger M. Homicide-suicides compared to homicides and suicides: Systematic review and meta-analysis. Forensic Sci Int 2013;233(13):28-36. http://dx.doi.org/10.1016/j.forsciint.2013.08.017 [ Links ]
22. Poeschla B, Combs H, Livingstone S, Romma S, Klein MB. Self-immolation: Socioeconomic, cultural and psychiatric patterns. Burns 2011;37(6):1049-1057. http://dx.doi.org/10.1016/j.burns.2011.02.011 [ Links ]
23. Central Intelligence Agency. CIA World Factbook 2010. https://www.cia.gov/library/publications/theworld-factbook/fields/2010.html (accessed 8 March 2016). [ Links ]
24. World Health Organization. Report on a Workshop in Suicide Prevention for Countries in the African Region. Port Louis, Mauritius, 13 - 15 October 1999. Geneva: WHO, 1999. [ Links ]
25. Statistics South Africa. Census 2011: Census in Brief, 2013. Pretoria: Stats SA, 2013. http://www.statssa.gov.za/census/census_2011/census_products/Census_2011_Census_in_brief.pdf (accessed 19 June 2017). [ Links ]
26. Matzopoulos RG, Thompson ML, Myers JE. Firearm and nonfirearm homicide in 5 South African cities: A retrospective population-based study. Am J Public Health 2014;104(3):455-460. http://dx.doi.org/10.2105/AJPH.2013.310650 [ Links ]
27. Töro K, Pollak S. Complex suicide versus complicated suicide. Forensic Sci Int 2009;184(1-3):6-9. http://dx.doi.org/10.1016/j.forsciint.2008.10.020 [ Links ]
28. Veale DJH, Wium CA, Müller GJ. Toxicovigilance I: A survey of acute poisonings in South Africa based on Tygerberg Poison Information Centre data. S Afr Med J 2013;103(5):293-297. http://dx.doi.org/10.7196/samj.6647 [ Links ]
29. Jena S, Mountany L, Muller A. A demographic study of homicide-suicide in the Pretoria region over a 5 year period. J Forensic Leg Med 2009;16(5):261-265. http://dx.doi.org/10.1016/j.jflm.2008.12.009 [ Links ]
 Correspondence:
Correspondence:
N Morris
neil.morris@up.ac.za
Accepted 28 March 2017

