










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.107 n.6 Pretoria Jun. 2017
http://dx.doi.org/10.7196/samj.2017.v107i6.12149
RESEARCH
The status of vaccine availability and associated factors in Tshwane government clinics
N J NgcoboI; M G KamupiraII
IMB ChB, MSc Med (Bioethics and Health Law), MBA, DOH, DTM&H, DCH; Independent consultant, Pretoria, South Africa
IIMB ChB, PhD (Public Health), MPH; World Health Organization, Country Office, Pretoria, South Africa
ABSTRACT
BACKGROUND. Vaccines have greatly contributed to the control of vaccine-preventable diseases and to human development. Efforts by many countries to introduce new vaccines are a significant move towards achieving the sustainable development goal for health. However, effective vaccine supply chains that ensure an uninterrupted supply of vaccines are pivotal to attaining universal access to life-saving vaccines and sustainable development. The introduction of new vaccines puts a strain on supply chains; South Africa (SA) is no exception, as there are indications of vaccine stock-outs in clinics.
OBJECTIVE. To establish the status of vaccine availability and associated factors in government health facilities of Tshwane Health District in Gauteng Province, SA.
METHODS. A cross-sectional study was conducted in a sample of randomly selected government clinics in the Tshwane health district of Gauteng Province. Data were collected using a structured measurement instrument in participating clinics. Data were analysed using Excel-based software (Microsoft, USA).
RESULTS. A total of 31 clinics participated. In the preceding 12 months, clinics had experienced vaccine stock-outs, especially of the three newer vaccines: pneumococcal conjugate vaccine, rotavirus and Pentaxim. These were also out of stock for a long duration; for over 2 weeks in a majority of clinics. The causes of vaccine stock-outs were: poor management of stock, district depot out of stock, unreliable deliveries, lack of pharmacy assistants and limited fridge capacity. Further burdening the situation is the ineffective emergency-ordering system.
CONCLUSION. Significant shortages of vaccines, which are essential drugs, occur in Tshwane government clinics. Vaccine supply chain issues and vaccine shortages should be treated as a priority at all levels of the healthcare system; therefore, a similar study should be conducted at national level. It is recommended that the vaccine supply chain should be restructured and overhauled with the use of advances in technology and could be linked with current initiatives such as MomConnect.
Immunisation has contributed greatly to human development. Immunisation saves more than 2.5 million lives a year, and could prevent an additional 2 million deaths a year with increased coverage and use of newer vaccines.[1] For immunisation programmes to sustain the impact made in the control of vaccine-preventable diseases and contribute to the attainment of sustainable development goals on health, an uninterrupted supply of quality vaccines maintained in the right cold chain to facilities where children are vaccinated is crucial. Interruption at any point in the supply chain results in stock-outs in all levels below; consequently, children are turned away without being vaccinated. This has serious implications for the health system, as vaccines are essential drugs and should be available at facilities that provide immunisation services at all times.
Reports point to vaccine shortages especially since the introduction of three new vaccines (rotavirus vaccine (RV), pneumococcal conjugate vaccine (PCV) and DTaP-IPV//Hib, a vaccine combination of five antigens referred to as Pentaxim), which are single doses. Reports include direct complaints from the public to the national and provincial departments of health offices, and newspaper reports. The post-introduction evaluation of the new vaccines conducted in all nine provinces by the Expanded Programme on Immunisation (EPI), with the support of the World Health Organization (WHO), found that more than 60% of facilities visited had experienced vaccine shortages in the 18-month period between the end of 2009 and July 2011.[2] Between April 2010 and March 2011, over 221 000 children who received the measles vaccine at 9 months old did not get the third dose of PCV that should have been given at the same time with the measles vaccine. All provinces and districts including Tshwane in Gauteng Province had vaccine stock-outs.
The Stop Stock Outs Project (SSP) reports that in 2015, 11% of facilities countrywide reported shortages of at least one vaccine on the day of contact. Most facilities reported stock-out of the hexavalent (DTaP-IPV-Hib-HBV) vaccine. SSP further reports outliers, such as Limpopo Province, where 28% of facilities reported vaccine stock-out on the day of contact.[3] The South African Health Review 2011[4]refers to frequent stock-outs of drugs in the Essential Drugs List due to poor management. It points out that the introduction of new services such as antiretroviral (ARV) therapy and new vaccines have exposed inadequate infrastructure at facility level, resulting in poor service.
The impact of introducing new vaccines and the resultant stock-outs have been experienced by a number of countries. For example, the introduction of rotavirus vaccine in Latin American countries such as Brazil, Ecuador, El Salvador and Venezuela in 2006/2007 resulted in frequent vaccine stock-outs in clinics.[5]
Vaccine shortages do not only undermine national efforts towards universal access to healthcare services, but they also have far-reaching consequences, which include an increased likelihood of disease outbreaks. It should be noted that Pentaxim, which has been replaced by the hexavalent, is not a new vaccine but merely a newer formulation. Pentaxim shortages meant that children were not protected against infections that had previously been under control. This could result in outbreaks of these conditions.
Literature is scarce on vaccine availability in government facilities, the extent of probable vaccine shortages and their causes. This study examined the extent and factors associated with vaccine stock-outs in government facilities in Tshwane Health District in Gauteng Province over a period of 1 year. Its objective was to establish the status of vaccine availability and associated factors in government health facilities of Tshwane Health District in Gauteng Province.
Methods
This was a cross-sectional survey of a sample of randomly selected government clinics in Tshwane Health District. The District Health Information System was the sampling frame. There are 75 primary healthcare clinics in Tshwane Health District; 32 facilities were sampled. The district office provided support by informing facility managers of the study; with this support and repeated phone calls to facilities requesting participation and setting up appointments, 31 of the 32 sampled facilities participated in the study.
The study was conducted over 2 weeks in December 2013. The principal investigator collected data by conducting interviews and a physical check of vaccine stock in participating clinics, using a structured measurement instrument. Questions were mainly of the closed type or used the Likert scale. Questions focused on: stock management; availability of a pharmacist or pharmacist assistants; stock delivery and emergency orders; fridge capacity; supervision; and the impact of the higher level of the healthcare system. Questions in relation to stock-out elicited: whether there were vaccine stock shortages on the day of the visit; whether there had been vaccine stock shortages in the last 12 months; which vaccines were out of stock; and the duration of stock-out. A few open-ended questions allowed for comments on opinion and experiences.
The Nelson Mandela Metropolitan University (NMMU) Unit for Statistical Consultation used in-house Excel-based (Microsoft, USA) statistical software to analyse the data.
Ethical approval was obtained from the Tshwane Health District Committee on Research (project number 45/2013 - Clearance Certificate). Ethical clearance was also obtained from the Human Research Ethics Committee of NMMU (ref. no. H13-BES-BS-010).
Results
Thirty-one of the 75 government primary healthcare facilities in Tshwane Health District participated, which covered the east, central and north regions. Respondents were the facility manager, the vaccinator, the pharmacist or pharmacist assistant, or the supervisor.
On the day of the visit, 11 items were out of stock in 9 (29%) of 31 clinics. These included rotavirus and measles vaccines, Pentaxim, measles diluent, tetanus and low strength diphtheria and tetanus (Td) and syringes. Practically all vaccines had been out of stock over different periods in the preceding 12 months in participating clinics (Table 1).
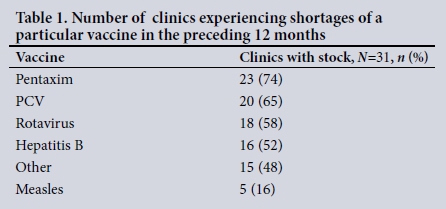
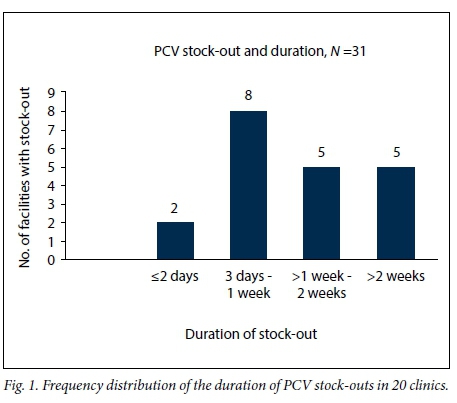
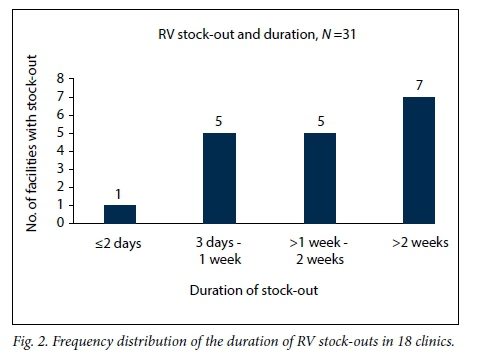
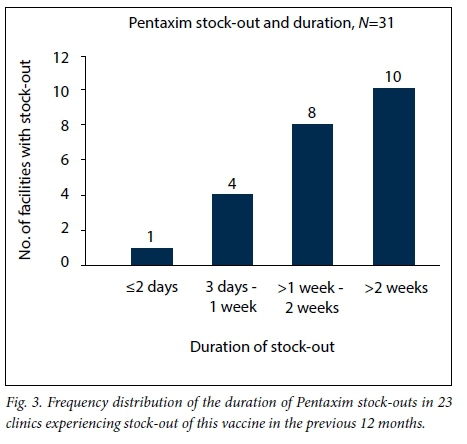
All clinics had experienced a shortage of at least one vaccine in the preceding 12 months. Vaccine shortages lasted from <2 days to >2 weeks (Figs 1 - 3).
Vaccine shortages were attributed to a number of reasons, which were not mutually exclusive. Reasons included delays in delivery, depot being out of stock, orders reduced by the district depot and shortage of vehicles to collect vaccines.
Clinics reported that the district depot reduced the quantities and supplied fewer doses than ordered. Only six (19%) of the 31 clinics positively indicated that their orders were not reduced. The vaccines that were most likely to be reduced by the depot were Pentaxim, PCV and RV, in that descending order.
Nineteen clinics had limited fridge capacity. Statistical analysis did not find an association between inadequate fridge capacity and vaccine shortage.
Clinics used stock cards to manage vaccine stock. Challenges with stock management contributed to stock shortages. Stock cards that correctly reflected the stock at hand were observed in 16 (52%) clinics. Stock cards indicated zero balances in the previous 12 months, which was in keeping with stock shortages.
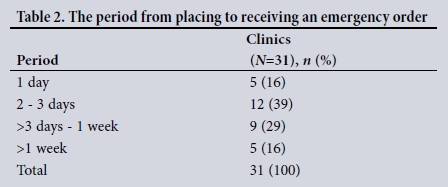
There were delays in delivery of pharmaceuticals. Although all clinics have an emergency ordering system, emergency orders took up to a week or more to be delivered (Table 2).
Of the 31 clinics, 18 (58%) had a health worker - a pharmacist, pharmacy assistant or enrolled nurse - dedicated to the management of pharmaceuticals, including vaccines. Statistical analysis revealed a significant association between the presence of a pharmacist or pharmacist assistants and the duration of vaccine stock-outs. The clinics without pharmacists or assistants were more likely to be out of stock of vaccines for longer periods than clinics that had them. None of the health workers responsible for vaccines, including pharmacists, had specific training on vaccine stock management.
Enrolled nurses who were assigned the responsibility of management of pharmaceuticals stated their resentment and frustration with this responsibility. It was observed in two facilities that vaccines were left in the boxes in which they were delivered for 2 - 3 days without being unpacked; no one took on this responsibility. This was observed in facilities without a pharmacist assistant, and was more likely to occur when vaccines were delivered on a Friday or just before a long weekend.
Supervision is conducted monthly in 24 (77%) clinics, quarterly in 6 (19%) and weekly in 1 clinic (3%). All 31 clinics indicated that specific EPI supervision was conducted. Only two clinics reported financial constraints as a possible cause of vaccine shortages. Nineteen (61%) indicated that there were no financial or budgetary issues.
In response to stock-outs, clinics borrow vaccines from the nearest clinics.
On pre-warning about impending shortages, three clinics reported that the depot had warned them of vaccine stock shortages, which was communicated by the national suppliers. None of the clinics had been able to warn users of health services in advance of expected stock shortages.
Discussion
The study findings point to significant shortages of vaccines in government clinics in Tshwane Health District. Shortages of vaccines are a serious national challenge and negate the national EPI policy statements that 'every day is an immunisation day' and 'every child that is well enough to go home, should go home immunised'.[6] These policy statements imply that there are sufficient quantities of vaccines at all times in all clinics and other healthcare facilities.
The findings of serious vaccine shortages are in keeping with those of the SSP.[3] However, the proportion of facilities that are out of stock are lower in the SSP study - 11% compared with 29% in this study. This could be due to different methodologies; the SSP study was based on phone calls, while in this study facilities were visited and there were physical inspections of vaccines.
Shortages appear to have become more of a challenge since the introduction of the newer vaccines Pentaxim, PCV and RV, in keeping with findings of Zaffran et al.[7] Zaffran et al. point out that the new vaccines are expensive, and packed in bulky pre-packed single dose presentations. This study also found that the newer vaccines were likely to have a longer duration of stock-out than other vaccines, 1 - 2 weeks or more in duration. This may be in keeping with the observation that these vaccines take up too much cold chain space, overwhelm the supply chains and lead to stock-outs.[7,8]
By contrast, the measles vaccine was out of stock in only five clinics, and the hepatitis B vaccine was out of stock in 16 clinics, despite the national shortages of hepatitis B and measles vaccines that were announced by the national suppliers about 3 or 4 months before the study was conducted (personal communication with National Department of Health).
Apart from the new vaccines and their demand on the cold chain, many other factors play a role in the shortages of vaccines. There seems to be no single factor that causes vaccine stock-outs. Rodewald et al.[9] came to a similar conclusion in ascertaining the causes of vaccine supply problems in the USA. This also applies to stock-outs of drugs in general, as highlighted by a study on drug shortages in the USA. [10] Furthermore, there may be an issue with the cost of the newer vaccines, which this study did not investigate.
Management issues are significant, and relate to: supervision that fails to anticipate and address stock-outs; stock management and timing of stock orders; the district depot being out of stock and reducing orders; delays in delivery; ineffective emergency ordering systems; and human resources for pharmaceuticals. These causes of vaccine shortages are not limited to EPI, and nor are they limited to facility level or a specific facility. The SSP survey had similar findings, as it found shortages of essential drugs. This points to weaknesses of the health system that undermine efforts aimed at effective service delivery.
There are different levels of challenges; clinics have challenges of poor stock management indicated by zero balances in the stock card, stock cards that are not up to date and failure to produce stock cards. At district and subdistrict levels, challenges include: supervision; delays in delivery of stock; cutting down on quantities ordered, which may not take into account head counts at facilities; and ineffective emergency-ordering systems. An emergency-ordering system that takes up to a week or more is a cause for concern. Supervision does not achieve what it should; although conducted monthly in over 74% of clinics, it still fails to address basic challenges such as vaccine shortages. This is in keeping with the findings of the Health Systems Trust in the District Health Barometer 2008/2009.[11]
Human resources for the management of pharmaceuticals at facility level are also a concern. Enrolled nurses assigned the responsibility for pharmaceuticals deeply resent this responsibility and do the absolute minimum. There is little support from the district depot, resulting in the neglect of pharmaceuticals. Further complications are that it takes longer for these facilities to realise that they have shortages, and they are unlikely to quickly address shortages by borrowing, which many other facilities do. The fact that they are not trained in vaccine stock management further compromises the situation.
The lack of effective mechanisms to pre-warn facilities on existing or expected shortages and to inform the users of healthcare facilities about the vaccine stock situation should be addressed. Effective communication can help to lessen the impact of shortages. The lack of communication, complicated by the inability to ascertain when stock is likely to be available, further impacts negatively on service delivery, and compromises clients, as it may result in repeated clinic visits and being turned away.
The use of stock cards for stock management at facility level deserves further consideration. This system is outdated and does not add value to the supply chain in the current era of technological advancement. Technology allows for the linking of the various levels of the supply chain and for tracing of products as to where they are in the supply chain, and can set up systems that generate automatic orders and can activate alarms when critical stock levels are reached. Stock cards do not allow for this kind of monitoring. One clinic used computer software to manage pharmaceutical stock, including vaccines.
It is therefore worth noting that the vaccine supply system has not been updated, and the different stages of the chain and location of depots remain as they were more than 20 - 30 years ago. A similar observation is made by Humphrey,[12] pointing out that the introduction of new vaccines has put unprecedented strain on the delivery and logistics systems that have remained the same and have not been upgraded over a number of decades.
With the recent changes in the EPI and the switch from Pentaxim to Hexaxim (a six-antigen-in-one vaccine, which includes hepatitis B) in 2015, and the changes in measles vaccine, concentrated efforts are required to ensure an uninterrupted supply of vaccines. Furthermore, the diphtheria outbreak in KwaZulu-Natal[13] might have been a result of shortages of Pentaxim, which is likely to have occurred over a period of time and resulted in many children being susceptible to previously controlled infections.
Study limitations
The study was limited to Tshwane government clinics. It did not focus on finances, and there was no specific focus on other consumables such as needles and syringes. Data were collected over a short period in December, and this timing could have had an effect on the results.
Conclusion and recommendations
Significant vaccine shortages occur in Tshwane government clinics and last for up to more than 2 weeks, and predominantly affect the availability of three relatively new vaccines.
The causes of vaccine shortages in clinics are many and relate to: (i) supply chain and challenges at higher levels; and (ii) factors at clinic level which include a lack of committed and supported officials. These findings point to management failure at district, subdistrict and facility levels.
Considering that vaccines are essential drugs, their shortages have serious implications for the functioning of the healthcare system. It is recommended that vaccine supply-chain issues and shortages should be treated as a priority at all levels of the healthcare system. A similar study at national level is urgently required to establish the situation with the availability of vaccines in health facilities and supplying depots.
Efforts to improve management of health facilities and systems should address the challenges identified, including: timely delivery of pharmaceuticals; handling of emergency orders; communication on expected stock shortages; effective supervision; and human resources for stock management at facility level.
It is critical that the stock management and information system be overhauled, and the system should link the district depot to each facility, taking into consideration head counts at facility level. Efforts should be made to improve communication with the users of healthcare facilities. Current initiatives such as the SSP should be supported, and the MomConnect initiative that has a reminder system for pregnant women to attend healthcare facilities could be linked to efforts aimed at monitoring and addressing vaccine shortages.
Tshwane district management would benefit from appointing a vaccine supply-chain logistician, whose responsibilities would include focused support of facilities.
Acknowledgements. None.
Funding. None.
Conflict of interest. None.
References
1. World Health Organization, United Nations International Children's Emergency Fund, World Bank. State of the World Vaccines and Immunization, 3rd ed. Geneva: World Health Organization, 2009. [ Links ]
2. National Department of Health, World Health Organization and United Nations International Children's Emergency Fund. Report on the Post Introduction Evaluation of New Vaccines in South Africa, NDOH, WHO and UNICEF: Pretoria, 2011. [ Links ]
3. Doctors Without Borders, the Rural Doctors Association of Southern Africa, the Rural Health Advocacy Project, the Treatment Action Campaign and the Southern African HIV Clinicians Society. Stop Stock Outs Project (SSP) Stockout National Survey, June 2016. www.groundup.org.za/media/uploads/documents/StopStockoutsSurvey2016.pdf (accessed 19 December 2016). [ Links ]
4. Naledi, T, Barron P, Schneider H. Primary health care in South Africa since 1994 and implications for the new vision of the PHC re-engineering. In: Paradath A, English R, eds. South African Health Review 2011. Durban: Health Systems Trust, 2011:21. [ Links ]
5. De Oliveira LH, Danovaro-Holliday MC, Matus CR, Andrus JK. Rotavirus introduction in the Americas: Progress and lessons learned. Expert Rev Vaccines 2008;7(3):343-353. http://dx.doi.org/10.1586/14760584.7.3.345 [ Links ]
6. The National Department of Health, Expanded Programme on Immunisation. The Vaccinator's Manual, Immunisation That Works. NDOH: Pretoria, 2012:13. [ Links ]
7. Zaffran M, Vandelaar J, Kristensen D, et al. The imperative for stronger vaccine supply and logistics systems. Vaccine 2013;31S:73-80. http://dx.doi.org/10.1016/j.vaccine.2012.11.036 [ Links ]
8. Lee BY, Assi TM, Rookkapan K, et al. Maintaining vaccine delivery following the introduction of the rotavirus and pneumococcal vaccines in Thailand. PLoS ONE 2001;6(9):e24673. http://dx.doi.org/10.1371/journal.pone.0024673 [ Links ]
9. Rodewald, LE, Orenstein, WA, Mason, D, Cochi, SL. Vaccine supply problems: A perspective of the Centers for Disease Control and Prevention. Clin Infec Disease 2006;42(Supp 3):104-10. http://dx.doi.org/10.1086/499587 [ Links ]
10. Gu A, Wertheimer AI, Brown B, Shaya AT. The drug shortages in the United States: Causes impact and management strategies. Innov Pharm 2011;2(4):740-757. http://pubs/lib.umn.edu/innovations/vol2/iss4/6 (accessed 12 October 2016). [ Links ]
11. Health Systems Trust. Clinic supervision rates. In: The District Health Barometer 2008/09. Durban: HST, 2009:41-45. [ Links ]
12. Humphrey G. Vaccination: Rattling the Supply Chain. Bull World Health Organ 2011;89:324-325. http://dx.doi.org/10.2471/BLT.11.030511 [ Links ]
13. National Institute for Communicable Diseases. Diphtheria: Update on Outbreak in KwaZulu-Natal Province. Communicable Diseases Communiqué. NICD, July 2015;14(8):4. [ Links ]
 Correspondence:
Correspondence:
N J Ngcobo
ntombenhle1m@gmail.com
Accepted 13 February 2017

