










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSAMJ: South African Medical Journal
versão On-line ISSN 2078-5135
versão impressa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.107 no.2 Pretoria Fev. 2017
http://dx.doi.org/10.7196/samj.2017.v107i2.11162
RESEARCH
Is it possible to differentiate tuberculous and cryptococcal meningitis in HIV-infected patients using only clinical and basic cerebrospinal fluid characteristics?
J E VidalI, II, III; E J F Peixoto de MirandaIV; J GerhardtV; M CrodaV; D R BoulwareVI
IMD, PhD; Department of Neurology, Emílio Ribas Institute of Infectious Diseases, São Paulo, Brazil
IIMD, PhD; Division of Infectious Diseases, University Hospital, School of Medicine, University of São Paulo, Brazil
IIIMD, PhD; Institute of Tropical Medicine, University Hospital, School of Medicine, University of São Paulo, Brazil
IVMD; Division of Internal Medicine, University Hospital, School of Medicine, University of São Paulo, Brazil
VMD; Department of Infectious Diseases, Emílio Ribas Institute of Infectious Diseases, São Paulo, Brazil
VIMD, MPH, C Trop Med; Division of Infectious Diseases and International Medicine, University of Minnesota, Minn., USA
ABSTRACT
BACKGROUND. Tuberculous and cryptococcal meningitis (TBM and CM) are the most common causes of opportunistic meningitis in HIV-infected patients from resource-limited settings, and the differential diagnosis is challenging.
OBJECTIVE. To compare clinical and basic cerebrospinal fluid (CSF) characteristics between TBM and CM in HIV-infected patients.
METHODS. A retrospective analysis was conducted of clinical, radiological and laboratory records of 108 and 98 HIV-infected patients with culture-proven diagnosis of TBM and CM, respectively. The patients were admitted at a tertiary centre in São Paulo, Brazil. A logistic regression model was used to distinguish TBM from CM and derive a diagnostic index based on the adjusted odds ratio (OR) to differentiate these two diseases.
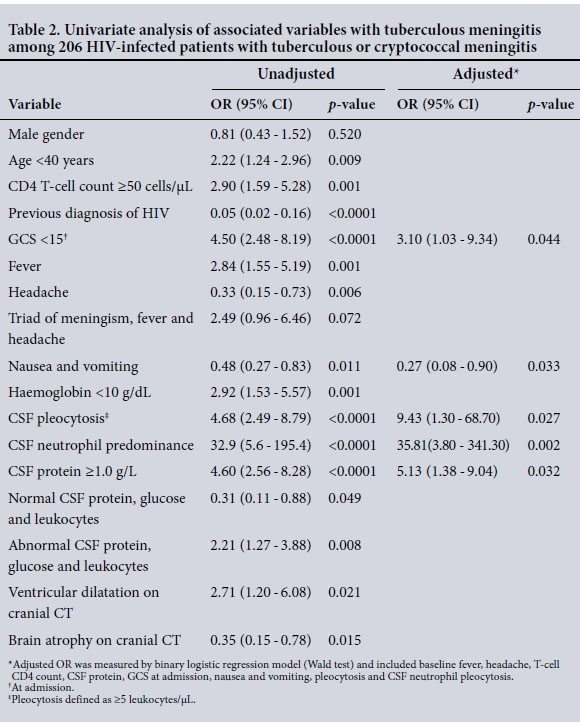
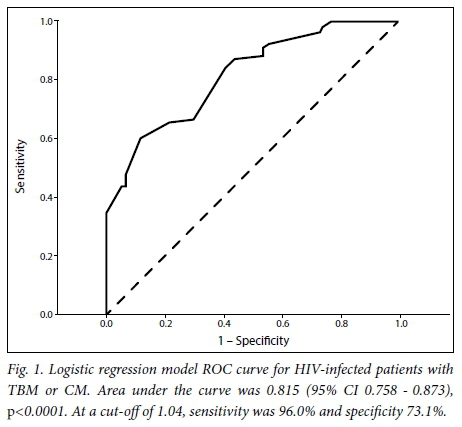
RESULTS. In multivariate analysis, TBM was independently associated with: CSF with neutrophil predominance (odds ratio (OR) 35.81, 95% confidence interval (CI) 3.80 - 341.30, p=0.002), CSF pleocytosis (OR 9.43, 95% CI 1.30 - 68.70, p=0.027), CSF protein >1.0 g/L (OR 5.13, 95% CI 1.38 - 19.04, p=0.032) and Glasgow Coma Scale <15 (OR 3.10, 95% CI 1.03 - 9.34, p=0.044). Nausea and vomiting (OR 0.27, 95% CI 0.08 - 0.90, p=0.033) were associated with CM. Algorithm-related area under the receiver operating characteristics curve was 0.815 (95% CI 0.758 - 0.873, p<0.0001), but an accurate cut-off was not derived.
CONCLUSION. Although some clinical and basic CSF characteristics appear useful in the differential diagnosis of TBM and CM in HIV-infected patients, an accurate algorithm was not identified. Optimised access to rapid, sensitive and specific laboratory tests is essential.
Tuberculous and cryptococcal meningitis (TBM and CM) are the most common causes of opportunistic meningitis in HIV-infected patients.[1-5] TBM and CM share similar clinical and laboratory features, resulting in delays to diagnosis and poorer outcomes, particularly in settings where confirmatory diagnosis is not possible.[6] Clinical algorithms have been proposed to simplify the diagnosis and treatment of these neurological infections,[6-8] but a lack of sensitivity and specificity precludes their implementation in clinical practice.
The objective of this study was to compare clinical and laboratory findings of TBM and CM in HIV-infected patients to propose an algorithm to differentiate these diseases.
Methods
We retrospectively analysed data from the clinical records of 108 and 98 HIV-infected patients with a culture-proven diagnosis of TBM or CM, respectively. The patients were admitted between March 1999 and June 2008 at the Emílio Ribas Institute of Infectious Diseases, São Paulo, Brazil. This hospital is a 250-bed tertiary teaching centre and the main referral institution for HIV-infected patients in São Paulo State. HIV infection was diagnosed by ELISA and confirmed by Western blot. We evaluated demographic, clinical, radiological and laboratory information. The study was approved by the ethical and scientific boards of the institution.
Cerebrospinal fluid (CSF) was obtained by lumbar puncture at hospital admission. Pleocytosis was defined as a leukocyte count >5 cells/μΚ The normal range of lumbar CSF glucose is >2.22 mmol/L (40 mg/dL) and CSF protein <0.45 g/L (45 mg/dL). Neutrophil pleocytosis was defined as >50% CSF leukocytes.
The comparison between groups (TBM v. CM) was performed using the Mann-Whitney U-test for numeric variables and Yates corrected χ2 or Fisher's exact test as appropriate for categorical variables. Odds ratio (OR) and 95% confidence interval (CI) were adjusted using a binary logistic regression model (Wald test) and included diagnosis of TBM v. CM as the dependent variable. Covariates and factors associated with TBM (v. CM) in univariate analysis were included to derive a diagnostic index based on clinical, laboratory and radiological findings. A receiver operating characteristics (ROC) curve was derived to calculate the accuracy of the logistic model. An estimation of cut-off for the diagnosis index was made to distinguish between TBM and CM. Statistical significance was defined as p<0.05, and SPSS 20.0 (IBM Corp., USA) software was used for statistical analysis.
Results
Table 1 shows a comparison of the clinical, radiological and laboratory characteristics of HIV-infected patients with TBM and CM. CSF with three abnormal parameters (pleocytosis, protein elevation and depressed glucose) was observed in 55.6% and 36.1% of patients with TBM and CM, respectively (p=0.002). The inhospital case-fatality rate was similar between the groups (TBM 29% v. CM 29%, p=0.578).
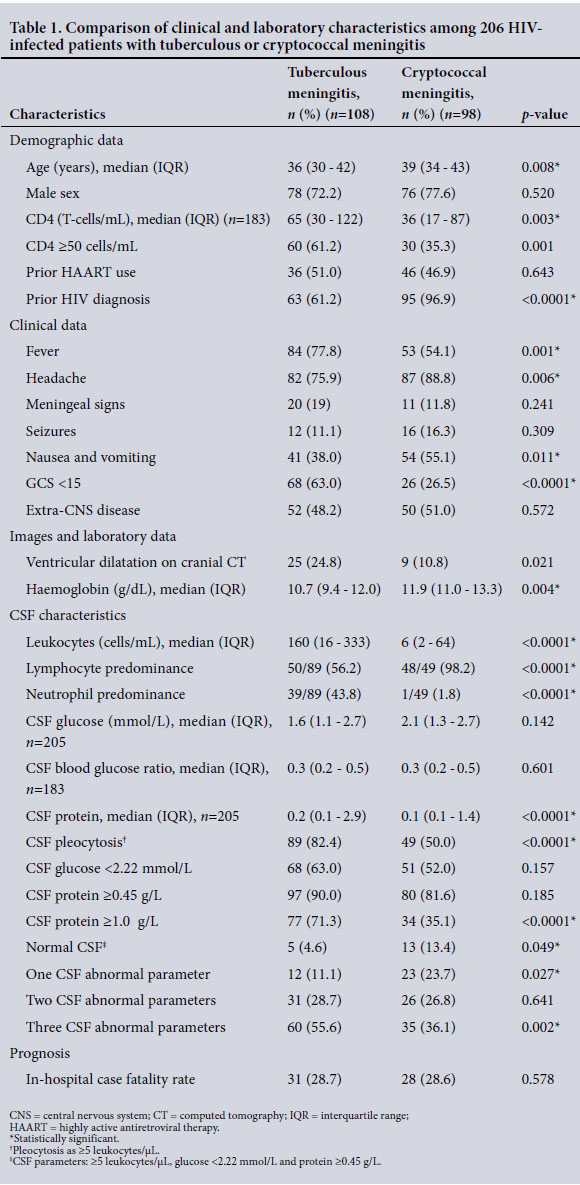
Microscopy was of limited value. Among TBM patients, Ziehl-Neelsen staining of CSF showed acid-fast bacilli (AFB) in only 5.5% (6/108) of cases. Among cryptococcal patients, India ink staining of CSF showed yeast compatible with Cryptococcus spp. in 84% (82/98) of cases. A cryptococcal antigen latex agglutination test of CSF was positive in only 82% (80/98) of cases.
Tables 2 and 3 show the results of univari-ate and multivariate modelling to identify variables associated with TBM.

A diagnostic index was derived using a multivariate model as follows: 1.635 x (protein >1.0 g/L) + 1.132 χ (Glasgow Coma Scale (GCS) <15) - 1.296 x (nausea and vomiting) + 3.578 x (CSF with polymorphs predominance) + 2.244 x (pleocytosis).
The parameters in parenthesis were coded 1 if present or 0 if absent. We excluded the value of the constant in the calculation of the index. The diagnostic index was a number that varied from -1.296 to 8.589, and negative values favoured a diagnosis of CM, while positive values favoured a diagnosis of TBM. The area under the ROC curve was 0.815 (95% CI 0.758 - 0.873; p<0.0001). At a cut-off of 1.04, sensitivity was 96.0% and specificity 73.1%. Values >1.04 presented a remarkable fall in the level of sensitivity - a cut-off of 5.33 presented a specificity of 100% but a sensitivity of 34.7% - while values <1.04, such as -0.73, presented higher sensitivity (100%) but lower specificity (3.2%). Fig. 1 shows the ROC curve of the logistic model.
Discussion
To the best of our knowledge this is the largest study comparing culture-proven CM and TBM in HIV-infected patients. Although some clinical and CSF characteristics appear useful to the discrimination of these two diseases, a diagnostic index could not be derived because of a lack of sensitivity and specificity, similar to that reported in a previous study,[6] which derived an area under the ROC curve very close to ours in spite of the smaller number of patients in the groups. A highly accurate logistic model did not result in an index with a cut-off sufficiently sensitive and specific to distinguish TBM and CM using clinical and laboratory features.
In the current study, CSF protein >1.0 g/L, GCS <15, absence of nausea and vomiting, neutrophil pleocytosis and CSF pleocytosis were independently associated with TBM diagnosis. There are few studies with a heterogeneous design comparing TBM and CM. Similar to our findings, GCS <15,[6] pleocytosis,[6] and neutrophil pleocytosis[9] have been found related to TBM. Fever,[6, 10] neck stiffness,[6] brain CT abnormalities,[10, 11] and extrameningeal disease[10] have been reported more frequently in TBM in other studies than in our study. In these studies, the variables of headache,[11] vomiting,'[1] altered sensorium,[11] high opening pres-sure,[6] low CSF white blood cell count[6] and advanced immunosupression[9,11] were more frequent in patients with CM. These results indicate that some clinical and laboratory characteristics seem useful in the differential diagnosis of TBM and CM; however, in clinical practice, they do not usually allow for sufficient discrimination between these two diseases.
Culture is the mainstay for diagnosis of TBM and CM, but alternative tests are evolving to provide more rapid and reliable diagnosis. In clinical practice, the India ink microscopy stain is usually available for cryptococcal diagnosis in resource-limited settings. Yet, in referral centres in Africa, India ink has only ~85% sensitivity,[12] similar to the sensitivity in our study. The use of India ink can be particularly problematic for early and/or low-burden infections, with sensitivity only 40% for quantitative cultures <1 000 colony-forming U/mL of CSF.[12] Thus, cryptococcal antigen (CrAg) tests could be necessary in at least 15% of patients with CM and negative India ink microscopy. In people with AIDS who have a negative India ink microscopy, the most common cause of meningitis is Cryptococcus in high-burden regions.[12] Recently, the World Health Organization included the CSF latex CrAg agglutination or lateral flow immunochro-matographic assay (LFA) as the preferred diagnostic approach for CM.
In our study, the sensitivity of CSF CrAg latex agglutination was only 82%, lower than usually reported for this test (93 - 100%).[13] CSF CrAg LFA (Immuno-Mycologics, USA) has a reported sensitivity of 99.3%, specificity of 99.1%, positive predictive value of 99.5% and negative predictive value of 98.7%.[12] CRAg LFA is a 'dipstick' test that requires only a drop of CSF and is relatively inexpensive, quick and easy to interpret. Unlike traditional latex agglutination, CrAg LFA does not require laboratory infrastructure or cold-chain transport.[13]
Unfortunately, rapid diagnosis of TBM is more complicated. Detection of AFB in patient samples using Ziehl-Neelsen staining is widely employed for diagnosis of TBM. AFB microscopy is, however, insensitive in TBM, with sensitivity rates of <10 - 20%.[14] The sensitivity of AFB microscopy in our study was only 5%. The sensitivity of smear microscopy in TBM can be maximised by examination of large-volume CSF samples (>6 mL) using several CSF specimens collected over a few days and prolonged slide examination (>30 min).[15] However, these criteria are rarely achieved in practice. Recent modifications to the Ziehl-Neelsen stain have shown optimistic results,[16] but replication in other sites is required. Over several decades, nucleic acid amplification tests (NAATs) of Mycobacterium tuberculosis have been evaluated for the diagnosis of TBM. A recent systematic review and meta-analysis of commercial NAATs with a CSF of M. tuberculosis culture-positive gold standard found a sensitivity of 64% and a specificity of 98%.[17] Despite suboptimal sensitivity, the rapid turnaround time of NAATs compared with culture enhances their role in the early accurate diagnosis of TBM. However, NAATs are unavailable for most resource-limited laboratories. Yet, the availability of automated NAATs via the GeneXpert system (Cepheid, USA) is increasing, but testing a large volume of centrifuged CSF remains essential.
In terms of the current status of meningitis diagnosis in HIV-infected patients, we would recommend a cryptococcal antigen assay (ideally LFA) as an initial approach.[18] Following a negative test in an adequate clinical and CSF context, empiric treatment for TBM should strongly be considered. However, it is important to consider bacteria (e.g. Streptococcus pneumoniae, Neisseria meningitidis, Listeria mono-cytogenes) and syphilitic meningitis in the differential diagnosis of meningitis in HIV-infected patients. More-rare aetiologies include other fungal pathogens (i.e. Histoplasma capsulatum, Candida, Cocci-dioides) and viruses (i.e. herpes virus, enterovirus).[19,20]
This study has limitations. We did not have CSF opening pressure available for the whole population. We included only culture-proven cases and not culture-negative cases, tested with techniques such as NAAT. Therefore, we did not compare clinical and laboratory differences between culture-positive and culture-negative cases. However, we did include a reasonable number of cases, all of which were culture proven, allowing rigorous case definition.
In conclusion, although some clinical and basic CSF characteristics appear useful in the differential diagnosis of TBM and CM in HIV- infected patients, an accurate algorithm was not identified. In this scenario, optimised access to more rapid, sensitive and specific laboratory tests is essential.
REFERENCES
1. Bergemann A, Karstaedt AS. The spectrum of meningitis in a population with high prevalence of HIV disease. QJM 1996;89(7):499-504. http://dx.doi.org/10.1093/qjmed/89.7.499 [ Links ]
2. Hakim JG, Gangaidzo IT, Heyderman RS, et al. Impact of HIV infection on meningitis in Harare, Zimbabwe: A prospective study of 406 predominantly adult patients. AIDS 2000;14(10):1401-1407. http://dx.doi.org/10.1097/00002030-200007070-00013 [ Links ]
3. Békondi C, Bernede C, Passone N, Minssart P, et al. Primary and opportunistic pathogens associated with meningitis in adults in Bangui, Central African Republic, in relation to human immunodeficiency virus serostatus. Int J Infect Dis 2006;10(5):387-395. http://dx.doi.org/10.1016/j.ijid2005.07.004 [ Links ]
4. Rizal Ganiem A, Parwati I, Wisaksana R, et al. The effect of HIV infection on adult meningitis in Indonesia: A prospective cohort study. AIDS 2009;23(17):2309-2316. http://dx.doi.org/10.1097/qad.0b01-3e3283320de8 [ Links ]
5. Jarvis JN, Meintjes G, Williams A, Brown Y, Crede T, Harrison TS. Adult meningitis in a setting of high HIV and TB prevalence: Findings from 4 961 suspected cases. BMC Infect Dis 2010;10(1):67. http://dx.doi.org/10.1186/1471-2334-10-67 [ Links ]
6. Cohen DB, Zijlstra EE, Mukaka M, et al. Diagnosis of cryptococcal and tuberculous meningitis in a resource-limited African setting. Trop Med Int Health 2010;15(8):910-917. http://dx.doi.org/10.1111/j.1365-3156.2010.02565.x [ Links ]
7. Marais S, Thwaites G, Schoeman JF, et al. Tuberculous meningitis: A uniform case definition for use in clinical research. Lancet Infect Dis 2010;10(11):803-812. http://dx.doi.org/10.1016/s1473-3099(10)70138-9 [ Links ]
8. Trachtenberg JD, Kambugu AD, McKellar M, et al. The medical management of central nervous system infections in Uganda and the potential impact of an algorithm-based approach to improve outcomes. Int J Infect Dis 2007;11(6):524-530. http://dx.doi.org/10.1016/j.ijid.2007.01.014 [ Links ]
9. Sánchez-Portocarrero J, Pérez-Cecilia E, Jiménez-Escrig A, et al. Tuberculous meningitis. Clinical characteristics and comparison with cryptococcal meningitis in patients with human immunodeficiency virus infection. Arch Neurol 1996;53(7):671-676. http://dx.doi.org/10.1001/archneur.1996.00550070109018 [ Links ]
10. Lan SH, Chang WN, Lu CH, Lui CC, Chang HW. Cerebral infarction in chronic meningitis: A comparison of tuberculous meningitis and cryptococcal meningitis. QJM 2001;94(5):247-253. http://dx.doi.org/10.1093/qjmed/94.5.247 [ Links ]
11. Satishchandra P, Nalini A, Gourie-Devi M, et al. Profile of neurologic disorders associated with HIV/ AIDS from Bangalore, south India (1989-96). Indian J Med Res 2000;111:14-23. [ Links ]
12. Boulware DR, Rolfes MA, Rajasingham R, et al. Multisite validation of cryptococcal antigen lateral flow assay and quantification by laser thermal contrast. Emerg Infect Dis 2014;20(1):45-53. http://dx.doi.org/10.3201/eid2001.130906 [ Links ]
13. Makadzange AT, McHugh G. New approaches to the diagnosis and treatment of cryptococcal meningitis. Semin Neurol 2014;34(1):47-60. http://dx.doi.org/10.1055/s-0034-1372342 [ Links ]
14. Thwaites G, Chau TTH, Mai NTH, Drobniewski F, McAdam K, Farrar J. Tuberculous meningitis. J Neurol Neurosurg Psychiatry 2000;68(3):289-299. [ Links ]
15. Thwaites GE, Chau TTH, Farrar J. Improving the bacteriological diagnosis of tuberculous meningitis. J Clin Microbiol 2004;42(1):378-379. http://dx.doi.org/10.1128/jcm.42.L378-379.2004 [ Links ]
16. Chen P, Shi M, Feng GD, et al. A highly efficient Ziehl-Neelsen stain: Identifying de novo intracellular Mycobacterium tuberculosis and improving detection of extracellular M. tuberculosis in cerebrospinal fluid. J Clin Microbiol 2012;50(4):1166-1170. http://dx.doi.org/10.1128/jcm.05756-11 [ Links ]
17. Solomons RS, van Elsland SL, Visser DH, et al. Nucleic acid amplification tests in tuberculous meningitis - a meta-analysis. Diag Microb Infect Dis 2014;78(4):398-403. http://dx.doi.org/10.1016/j.diagmicrobio.2014.01.002 [ Links ]
18. Bahr NC, Boulware DR. Methods of rapid diagnosis for the etiology of meningitis in adults. Biomark Med 2014;8(9):1085-1103. http://dx.doi.org/10.2217/bmm.14.67 [ Links ]
19. Veltman JA, Bristow CC, Klausner JD. Meningitis in HIV-positive patients in sub-Saharan Africa: A review. J Int AIDS Soc 2014;17(1):19184. http://dx.doi.org/10.7448/ias.17.L19184 [ Links ]
20. Lorber B. Listeriosis. Clin Infect Dis 199734(11):1-11. http://dx.doi.org/10.1093/dinids/24.L1 [ Links ]
 Correspondence:
Correspondence:
J E Vidal
josevibe@gmail.com
Accepted 6 October 2016

