










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSAMJ: South African Medical Journal
versión On-line ISSN 2078-5135
versión impresa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.106 no.9 Pretoria sep. 2016
http://dx.doi.org/10.7196/samj.2016.v106i9.10572
RESEARCH
The PAWPER tape and the Mercy method outperform other methods of weight estimation in children at a public hospital in South Africa
V G GeorgoulasI; M WellsII
IMB BCh; Division of Emergency Medicine, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IIMB BCh, MSc (Med) (Emergency Medicine), FCEM (SA), Dip PEC (SA); Division of Emergency Medicine, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
ABSTRACT
BACKGROUND: A rapid, accurate weight-estimation method is essential in paediatric emergency care, when it may not be possible to weigh a child, as drug dose calculations cannot be completed without weight.
OBJECTIVES: To determine and compare the performance of the Broselow tape, PAWPER (Paediatric Advanced Weight Prediction in the Emergency Room) tape, Mercy method, Wozniak method and three age-based formulae in estimating the weight of children. A secondary objective was to assess whether the addition of a figural rating scale to assess body habitus improved the performance of the PAWPER tape.
METHODS: We estimated the weights of children between the ages of 1 month and 12 years using the Broselow tape, PAWPER tape, Mercy method and Wozniak method. The performance of the four methods was evaluated, and they were compared with one another and with three aged-based formulae.
RESULTS: Three hundred children were enrolled in the study. The PAWPER tape and Mercy method performed the best, estimating weight within 10% of actual weight (PW10) in 88% and 80% of cases, respectively. The Broselow tape and Wozniak method fared significantly worse (PW10 54% for Broselow, 71% for the ulna length method and 63% for the tibia length method). The use of a figural rating scale to assess body habitus did not significantly improve the overall performance of the PAWPER tape. The age-based formulae performed poorly.
CONCLUSIONS: The PAWPER tape and Mercy method outperformed the Wozniak method and Broselow tape in estimating weight of children. The Broselow tape and the age-based formulae were very poor weight-estimation methods and should no longer be used, given the availability of better methods.
During paediatric resuscitation, most interventions are based on the weight of the child. These include dosing of medications, volumes of resuscitation fluids, cardioversion/defibrillation joules and the choice of equipment sizes.[1] If possible, all children should be weighed on a scale to obtain their actual weight. However, this is often impossible or impractical in an emergency setting, and an accurate, rapid weight-estimation method is essential in these situations.[1]
Over the past three decades, many different weight-estimation methods have been used, each with its own advantages and limitations. The most commonly used methods include guesses or estimations by parents or healthcare workers, age-based formulae and length-based methods. Parental estimates of weight have been shown to be better than some age-based formulae, but are still not very accurate.[2] Age-based formulae are easy to use, but perform poorly.[1,3-5] The old Advanced Paediatric Life Support (APLS) formula (now called the European Life Support (EPLS) formula) has been shown to lack desirable accuracy and to underestimate children's weights.[1-4] The new APLS formula, developed in 2011, is more complex with three separate formulae for three age categories, but still underestimates weight in populations with a high prevalence of obesity.[3,5] The Best Guess formula, developed in Australia, has a tendency to overestimate weight and is inaccurate in all weight categories.[5,6]
Length-based methods are the most widely used today. The most well-known system is the Broselow tape, which was originally developed in 1988 and has been updated periodically. Although still commonly used, it does not take into consideration the child's body habitus and usually underestimates weight, especially in obese children.[7] It has also been shown to overestimate children's weights in undeveloped countries.[8]
Newer dual length- and habitus-based (two-dimensional) systems, namely the Mercy method, the PAWPER (Paediatric Advanced Weight Prediction in the Emergency Room) tape and the Wozniak method, have been developed in the past few years and have been shown to be superior to traditional weight-estimation systems. The Mercy method is a weight-estimation strategy developed in Missouri, USA, in 2009. The method uses surrogates of total body length (humeral length) and habitus (mid-arm circumference (MAC)) to estimate weight.[9] The humeral length and MAC provide 'segmental weights' read off a table, which are then added together to obtain an estimated weight.[9] The method proved to be superior to 13 other weight-estimation strategies in preliminary testing and performed well across a wide range of ages and weights.[9] It has been externally validated in the USA,[10] as well as in two undeveloped countries, namely Mali[11] and India.[12] The PAWPER tape was developed in 2007 in South Africa (SA) as a low-cost, single-use tape that uses a two-step process to estimate weight. In the first step, a baseline weight estimation is made by measuring supine length. The second step involves modification of this weight up or down according to a child's body habitus. It has been shown to estimate weight very accurately, far outperforming the Broselow tape,[13] but needs further validation. The Wozniak method was developed in a study in Gaborone, Botswana, in a predominantly HIV-positive sample of children. The method uses the MAC and tibia length, or MAC and ulna length, in a regression formula to estimate children's weights. It was shown to be very accurate, and outperformed the Broselow tape, the MAC formula, and the APLS, Luscombe and Theron age-based formulae.[14] Although the method showed quite promising results, it has not yet been validated in any other populations.
Objectives
To evaluate the above three two-dimensional methods of weight estimation, plus three age-based formulae, in a population of children from a background of low socioeconomic status, where malnutrition is common. We aimed to see which method was the most accurate in this population, and over which age or weight ranges each method worked best in estimating weight. A secondary objective was to determine whether a figural rating scale system improved the accuracy of habitus assessment for the PAWPER tape.
Methods
The study was approved by the Health Research Ethics Committee of the University of the Witwatersrand, Johannesburg, SA.
Study design. A prospective, cross-sectional, hospital-based study.
Study setting. Rahima Moosa Mother and Child Hospital, a public hospital in Johannesburg serving a community of mostly low socioeconomic status. This study was conducted in the paediatric outpatient department and admission ward of the hospital from August 2014 to January 2015.
Study population. Children between the ages of 1 month and 12 years, who were not in need of emergency medical treatment, were included in the study. Children with congenital conditions such as dwarfism, or whose length could not be assessed for any reason, e.g. due to contractures, were excluded from the study. A non-consecutive convenience sample of 300 children was used.
Study procedure
Once consent had been obtained, each study participant was dressed in a hospital gown in a private cubicle. The child's body habitus was assessed using the original PAWPER tape method and then with the aid of a figural rating scale (modified from Collins figural images),[15] and assigned a habitus score (HS). Using these HSs, the weight was estimated using the PAWPER tape. The child's weight was then estimated using the 2011 Broselow (edition A) tape. The child's supine length was measured with a measuring tape. Measurements were then taken of the child's humeral length, MAC, ulna length and tibia length. Using these values, the weight was estimated using the Mercy and Wozniak methods. The child's actual weight was then measured on a scale and recorded to the nearest 0.1 kg. Weight estimations were generated from the age-based formulae, as follows:

Statistical analysis
The performances of the weight-estimation systems were evaluated by comparing them with actual measured weight, and with one another. Three major outcomes were evaluated for the whole population, as well as for subgroups of age (<2 years, 2 - 5 years and >5 years), weight (<12 kg, 12.1 - 20 kg and >20 kg) and body HS categories: (i) mean percentage error (MPE) was calculated for each method, which gave a measure of the overall estimation bias; (ii) limits of agreement of the MPE and the root mean squared percentage error (RMSPE) were calculated, which gave a measure of estimation precision; and ( iii) the percentage of estimations that fell within specific weight-estimation error categories was determined for each method, which provided a measure of overall accuracy.
Modified Bland-Altman plots were constructed to further assess the agreement between each of the estimation methods and the actual weight.
Results
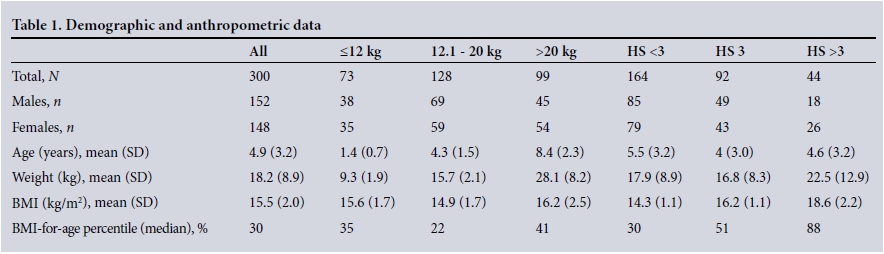
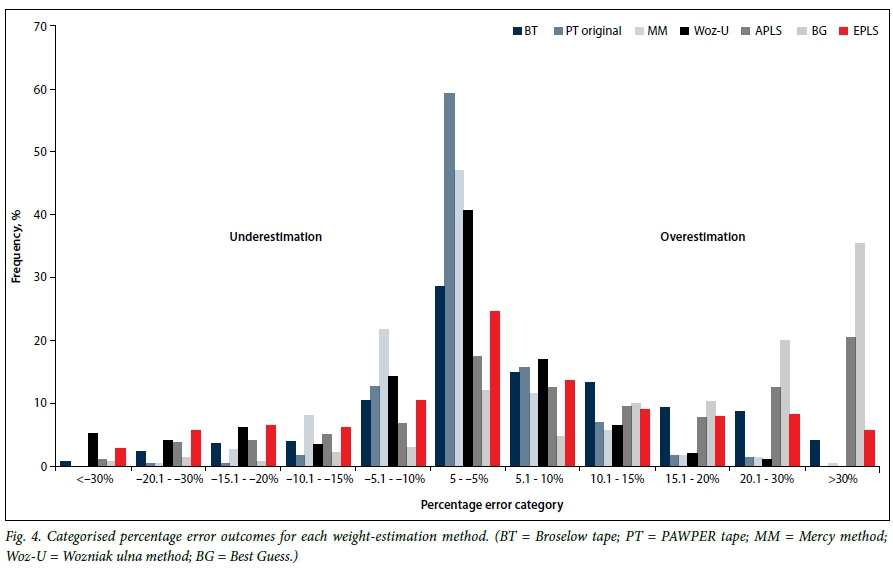
A total of 300 children were enrolled in the study. The participants were equally distributed by sex (50.7% male, 49.3% female), and had a mean age, weight and body mass index (BMI) of 4.9 years, 18.2 kg and 15.5 kg/m2, respectively. Selected demographic and anthropometric parameters are summarised in Table 1. The distribution of HSs assigned to the sample of children in the study is shown in Fig. 1, the majority of children having an HS of 2 (38.0%) or 3 (30.7%), and the figural rating scale in Fig. 2. Table 2 shows the data for all methods of weight estimation, indicating their measures of bias, precision and accuracy for the entire population and for each weight, age and HS category. The PAWPER tape and Mercy method had the least bias and best precision, while the Best Guess method had the most bias and was the least precise. Modified Bland-Altman plots (Fig. 3) illustrate the agreement between each of the estimation methods and the actual weight. Fig. 4 shows the categorised percentage error outcomes for each of the weight-estimation systems, demonstrating both the degree and direction (over- or underestimation) of weight-estimation errors. The Broselow tape significantly overestimated weight. The PAWPER tape also overestimated weight, but far less than the Broselow tape. The overall absolute accuracy of each of the methods by PW10 and PW20 is shown in Fig. 5. The PAWPER tape and Mercy methods were within 10% of actual weight in >80% of the weight estimations, and far outperformed any of the other methods. All three of the age-based formulae had a PW10 of <50%.



In some cases, weight could not be estimated at all, as the child's measurements exceeded the restrictions of various methods. In the tape-based methods, 15 (5.0%) and 6 (2.0%) children had lengths that exceeded the lengths of the Broselow tape and the PAWPER tape, respectively. For the Wozniak method, 5 children (1.7%) had measurements that were off the MAC-ulna chart and 17 (5.7%) were off the MAC-tibia chart, and so an estimate of weight was impossible. The Mercy method was able to estimate weight in all cases.
Discussion
Demographics
The 300 children enrolled in this study were taken from the outpatient department and admission ward of a public hospital, which mainly serves a population of lower socioeconomic status.
The median BMI-for-age centile was 30, which differs from the private hospital population used in the original PAWPER tape study, where the median BMI-for-age centile was 50.[13] This difference is mirrored by the HSs, which in this study were predominantly 2 (38.0%) and 3 (30.7%) whereas in the original PAWPER tape study, where the children came from a higher socioeconomic group, HSs were assigned as 3 in 51.4% of cases and 4 in 22.3%.[13] The population in this study was, however, similar to the population used in the development of the Wozniak method.[14]
The Mercy method was developed from the National Health and Nutrition Examination Survey (1999 - 2008), and initially validated in the USA on a cohort of healthy children.[9,10] It has since been validated in Mali and India in populations with a high prevalence of low weight for age, similar to the population in this study.[11,12]
Comparison of the performance of the weight-estimation methods
The PAWPER tape and Mercy method performed best in our study population. They had the most neutral bias, and better precision and accuracy than the other methods. The Mercy method had the least bias and slightly underestimated weight (as reflected by an MPE of -0.9%), whereas the Broselow tape had the most bias and substantially overestimated weight (MPE 5.5%). There was only a small difference in bias between the PAWPER tape and the Mercy method (paired f-test, p<0.0001). The PAWPER tape was the most precise (RMSPE 5.3), followed by the Mercy method and then the Wozniak method (paired f-test, p<0.0001). The precision of the Broselow tape was significantly worse than all the two-dimensional methods, with an RMPSE of 11.4 (paired f-test, p<0.0001).
The PAWPER tape was significantly more accurate than all the other methods. It had a PW10 of 88% and 85% for the original and figural-assisted modified methods, respectively, compared with 54% for the Broselow tape (McNemar test, p<0.0001). This is similar to the PAWPER tape validation study, in which the PAWPER tape had a PW10 of 89.2% and the Broselow tape a PW10 of 63.6%.[13] The PAWPER tape was slightly less accurate in the <12 kg group, in children aged <2 years and in those with an HS of <3. It was more accurate than the Broselow tape in all weight categories.
The Broselow tape performed the worst of all the methods, with the exception of the age-based formulae, with a PW10 of 54% overall. Its accuracy decreased with increasing age and weight. It was most accurate in the 2 - 5-year age group and in the HS 3 subgroup, which is not surprising considering that body habitus is not taken into account in its estimation process and these are the children of average weight for height. The Broselow tape overestimated weight in all age and weight subgroups, in contrast to previous studies in developed countries, where the Broselow tape was found to underestimate weight.[1,7] This was probably partly due to the high level of low weight for age in this population as well as the changes in the Broselow 2011 edition A to reduce underestimation of weight. The Mercy method estimated weight very well in this population. It had a low bias, high precision and very good accuracy. It had a PW10 of 80%, slightly better even than in its original and validation studies.[9-11,16] It performed generally well over all subgroups of age, weight and body habitus, but slightly worse in the smallest and youngest children, and children in the HS 3 subgroup.
The Wozniak method consists of two methods of weight estimation, one of which uses MAC plus ulna length and the other MAC plus tibia length in a formula to calculate weight. Both variations performed moderately overall, with PW10s of 71% and 63%, respectively. This is somewhat worse than the results in the original Wozniak study, where the corresponding results were 78.8% and 81.5%, respectively.[14] In Wozniak's study, the derivation sample only included children aged >18 months and the results were poorest for children weighing <10 kg and >40 kg, and best for children weighing between 25 and 30 kg.[14] In our population the Wozniak systems were extremely inaccurate and imprecise in children weighing <12 kg and those aged <2 years, and best in the >20 kg and age >5 years subgroups. Overall, and in all weight, age and HS subgroups, the MAC-ulna method performed better than the MAC-tibia method. Both methods underestimated weight overall.
Both the Mercy and Wozniak methods use two-step processes. They require the surrogate length and the MAC measurements, followed by calculations or values read off a table. In an emergency situation, this would take some time to work out and provide opportunities for mistakes to be made, especially for people not familiar with the methods. From a practical point of view, they are therefore more difficult and complex to use than tape-based methods and have yet to be evaluated in studies with real or simulated emergencies.
The EPLS (old APLS) formula performed very poorly in this study. In all age categories and in children weighing <20 kg, it overestimated weight. In the >20 kg weight category and in children assessed as HS >3, it underestimated weight. In a previous study in the UK, the formula was shown to underestimate weight across all ages.[4]
The new APLS formula, which was shown to perform better than the old one in previous studies,[3,5] performed significantly worse in our study. Of all the formulae evaluated in this study, the Best Guess formula performed the worst. It had PW10s of 13.7%, 23.4% and 19.2% in the <12 kg, 12.1 - 20 kg and >20 kg weight categories, respectively. It performed far worse than in previous studies done in Australia[6] and in SA,[1] but similarly to in another Australian study.[5] In all weight and age categories, it overestimated weight. The use of these very inaccurate formulae could lead to significant medication errors and potential patient harm.
Cases where methods could not be used
Some children's measurements fell outside the restrictions of the various methods for the Broselow tape, the Wozniak methods and the PAWPER tape. The Mercy method could be used for all children's measurements, which is an advantage compared with all the other methods.
PAWPER tape original v. figural-assisted method of HS assessment
One of the secondary objectives of this study was to see whether a figural-assisted assessment of HS would improve the accuracy of weight estimation compared with the original gestalt method of 'eye-balling' a child in order to assign an HS. The Devised Weight Estimating Method, which also estimates weight based on an assigned HS, has been shown to perform well in estimating children's weights, but is not often used. The figural-assisted method functioned slightly, but not significantly, worse than the original method overall. This was solely a consequence of a poorer result in infants and younger children, where HS was overestimated more than with the gestalt method. The figural-assisted method performed better than the gestalt method in older and heavier children (although not statistically significantly; McNemar test, p=0.12). Perhaps the images used as reference look thinner than the children of that HS, and should be modified in order to improve their accuracy.
In this study only one person assigned the scores and took measurements, and may have had an improved ability to do this after many assessments. The figural-assisted method may prove to be useful for a person who is not experienced in assessing body habitus and may also make the HS assessments more standardised.
Study limitations
Only children who were not in need of emergency care were included in this study. There may potentially be some bias, as critically ill children may be different to clinically well children in terms of their body habitus appearance and weights. The researcher assessed and measured the children in a non-emergency, calm environment. Measurements in a stressful emergency situation may be more rushed and therefore possibly less accurate. Only one person took the measurements, so no comparison of interobserver variability was possible. Finally, the researcher's assessment of the HS was based on her own perception of 'average', which may differ from that of other healthcare providers.
Conclusions
The dual length- and habitus-based systems were the most accurate methods in this study population, with the Mercy method and the PAWPER tape best overall. All methods were weakest in infants and toddlers, but the Wozniak method was potentially dangerously inaccurate in this subgroup.
The Broselow tape was very poor at estimating weight in children from a background of lower socioeconomic status and should no longer be used for this purpose, as it may also cause significant medication errors.
Age-based formulae were extremely inaccurate, as has been demonstrated previously, and their role in emergency care should be abandoned.
References
1. Geduld H, Hodkinson PW, Wallis LA. Validation of weight estimation by age and length based methods in the Western Cape, South Africa population. Emerg Med J 2011;28(10):856-860. DOI:10.1136/emj.2010.098640 [ Links ]
2. Krieser D, Nguyen K, Kerr D, Jolley D, Clooney M, Kelly A-M. Parental weight estimation of their child's weight is more accurate than other weight estimation methods for determining children's weight in an emergency department? Emerg Med J 2007;24(11):756-759. DOI:10.1136/emj.2007.047993 [ Links ]
3. Seddon C, Lockitt L, Dhanjal S, Eisenhut M. Validation of Advanced Paediatric Life Support formulas for weight calculation in a multiethnic population. ISRN Pediatr 2012;2012:1-4. DOI:10.5402/2012/869634 [ Links ]
4. Luscombe MD, Owens BD, Burke D. Weight estimation in paediatrics: A comparison of the APLS formula and the formula Weight=3(age)+7'. Emerg Med J 2011;28(7):590-593. DOI:10.1136/emj.2009.087288 [ Links ]
5. Graves L, Chayen G, Peat J, O'Leary F. A comparison of actual to estimated weights in Australian children attending a tertiary children's hospital, using the original and updated APLS, Luscombe and Owens, Best Guess formulae and the Broselow tape. Resuscitation 2014;85(3):392-396. DOI:10.1016/j.resuscitation.2013.11.024 [ Links ]
6. Thompson MT, Reading MJ, Acworth JP. Best Guess method for age-based weight estimation in paediatric emergencies: Validation and comparison with current methods. Emerg Med Australas 2007;19(6):535-542. DOI:10.1111/j.1742-6723.2007.01031.x [ Links ]
7. DuBois D, Baldwin S, King WD. Accuracy of weight estimation methods for children. Pediatr Emerg Care 2007;23(4):227-230. DOI:10.1097/PEC.0b013e31803f5aca [ Links ]
8. Clark MC, Lewis RJ, Fleischman RJ, Ogunniyi AA, Patel DS, Donaldson RI. Accuracy of the Broselow tape in South Sudan, 'The hungriest place on earth'. Acad Emerg Med 2016;23(1):21-28. DOI:10.1111/acem.12854 [ Links ]
9. Abdel-Rahman SM, Ridge AL. An improved pediatric weight estimation strategy. Open Med Dev J 2012;4:87-97. DOI:10.2174/1875181401204010087 [ Links ]
10. Abdel-Rahman SM, Ahlers N, Holmes A, et al. Validation of an improved pediatric weight estimation strategy. J Pediatr Pharmacol Ther 2013;18(2):112-121. DOI:10.5863/1551-6776-18.2.112 [ Links ]
11. Dicko A, Alhousseini ML, Sidibé B, Traoré M, Abdel-Rahman SM. Evaluation of the Mercy weight estimation method in Ouelessebougou, Mali. BMC Public Health 2014;14:270. DOI:10.1186/1471-2458-14-270 [ Links ]
12. Batmanabane G, Jena PK, Dikshit R, Abdel-Rahman S. Using the Mercy Method for weight estimation in Indian children. Global Pediatr Health 2015;2:1-7. DOI:10.1177/2333794X14566625 [ Links ]
13. Wells M, Coovadia A, Kramer E, Goldstein L. The PAWPER tape: A new concept tape-based device that increases the accuracy of weight estimation in children through the inclusion of a modifier based on body habitus. Resuscitation 2013;84(2):227-232. DOI:10.1016/j.resuscitation.2012.05.028 [ Links ]
14. Wozniak R. The evaluation of potential weight-estimation methods in a primarily HIV positive cohort in Botswana for use in resource limited settings. Open Collections, UBC Theses and Dissertations, University of British Columbia, 2013. DOI:10.14288/1.0073523 [ Links ]
15. Abdel-Rahman SM, Paul IM, James LP, Lewandowski A. Evaluation of the Mercy TAPE: Performance against the standard for pediatric weight estimation. Ann Emerg Med 2013;62(4):332-339. DOI:10.1016/j.annemergmed.2013.02.021 [ Links ]
 Correspondence:
Correspondence:
V G Georgoulas
vanessa.greyling@gmail.com
Accepted 31 January 2016.


{kind=link}
{kind=link}
{kind=link}
{kind=link}