










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.106 n.9 Pretoria Sep. 2016
http://dx.doi.org/10.7196/samj.2016.v106i9.11028
IN PRACTICE
CLINICAL ALERT
Invasive carbapenem-resistant Enterobacteriaceae infection at a paediatric hospital: A case series
O O MalandeI; A du PlessisII; D RipIII, IV; C BamfordV, VI; B EleyVII
IMB ChB, MMed (Paed), Cert ID (SA) Paed; Paediatric Infectious Diseases Unit, Red Cross War Memorial Children's Hospital, Cape Town, and Department of Paediatrics and Child Health, Faculty of Health Sciences, University of Cape Town, South Africa
IIBPharm; Main Pharmacy, Red Cross War Memorial Children's Hospital, Cape Town, South Africa
IIIPhD (Biotechnol); National Health Laboratory Service, Microbiology Laboratory, Groote Schuur Hospital, Cape Town, South Africa
IVPhD (Biotechnol); Division of Medical Microbiology, Department of Pathology, Faculty of Health Sciences, University of Cape Town, South Africa
VMB ChB, DCH (SA), MPhil (Mat Child Health), FCPath (Microbiol), MMed (Med Microbiol); National Health Laboratory Service, Microbiology Laboratory, Groote Schuur Hospital, Cape Town, South Africa
VIMB ChB, DCH (SA), MPhil (Mat Child Health), FCPath (Microbiol), MMed (Med Microbiol); Division of Medical Microbiology, Department of Pathology, Faculty of Health Sciences, University of Cape Town, South Africa
VIIMB ChB, FCPaed (SA), BSc Hons; Paediatric Infectious Diseases Unit, Red Cross War Memorial Children's Hospital, Cape Town, and Department of Paediatrics and Child Health, Faculty of Health Sciences, University of Cape Town, South Africa
ABSTRACT
BACKGROUND: There are no paediatric reports of invasive infection caused by carbapenem-resistant Enterobacteriaceae (CRE) from Africa.
OBJECTIVES: To document a series of cases of CRE infections at a tertiary children's hospital in Cape Town, South Africa, describing the clinical and microbiological findings in these children.
METHODS: A retrospective, descriptive study was completed using data from a series of children with invasive CRE infection between 2010 and 2015, sourced from their clinical notes and microbiology results.
RESULTS: The first of 10 invasive CRE infections during the study period occurred in November 2012. Nine CRE infections were caused by Klebsiella pneumoniae, and one by both K. pneumoniae and Escherichia coli. The median age was 25 months (interquartile range (IQR) 5 - 60). All 10 CRE infections were hospital acquired. The median length of hospitalisation before CRE infection was 28.5 days (IQR 20 -44). Eight of the children were exposed to carbapenems during the 12-month period prior to invasive CRE infection. Six were treated with colistin and carbapenem combination therapy, of whom 2 died, including 1 of a non-CRE event. The other 4 children received colistin monotherapy. All these children died, including 2 from non-CRE events.
CONCLUSIONS: Children with invasive CRE infection and severe underlying disease must be treated with combination antibiotic therapy. Strict infection control practice and antibiotic stewardship are necessary to contain the spread of CRE and limit the number of new infections.
Invasive infection caused by carbapenem-resistant Enterobacteriaceae (CRE), first documented in the late 1990s, has become a serious global public health problem.[1] Resistance to carbapenems may result from several mechanisms, including alteration of outer membrane permeability due to loss of porins, upregulation of efflux systems together with extended-spectrum β-lactamases (ESBLs), or commonly the production of carbapenemases.[2] A large number of carbapenemases belonging to all four classes of β-lactamases have been described. However, clinically relevant carbapenemases belong to three of these classes, namely class A β-lactamases such as Klebsiella pneumoniae carbapenemase (KPC) and Guiana extended-spectrum carbapenemase (GES), class B metallo-β-lactamases such as Verona integron-mediated metallo-ß-lactamase (VIM), imipenemase (IMP) and New Delhi metallo-ß-lactamase (NDM), and class D ß-lactamases including oxacillinase (OXA) subtypes such as OXA-48. [3,4] The first CRE invasive infections in South Africa (SA) were reported in adult patients from Gauteng Province in 2011, caused by NDM-1- and KPC-2-expressing K. pneumoniae isolates.[5] Since then, invasive infections caused by CRE-carrying resistance genes of these three classes of ß-lactamases have been reported in SA.[6]
Publications from the USA, Europe, Asia and the Middle East have begun to describe CRE infection in children.'7-151 Age at presentation ranged from 0 to 18 years, and ~40% (32/79) were <12 months of age. The main types of infection were bloodstream infection, urinary tract infection and soft-tissue infection.'7-151 The crude case fatality rate was 7.4% (5/68).[13-15] A wide spectrum of potential risk factors for CRE infection was identified, including previous admission to an intensive care unit (ICU), hospitalisation for >48 hours, the presence of an indwelling device, underlying medical conditions, necrotising enterocolitis and/or short-bowel syndrome, solid organ or stem cell transplantation, exposure to immunosuppressants, previous exposure to antibiotics, including third-generation cephalosporins, fluoroquinolones or carbapenems, and previous infection by a multidrug-resistant organism.[13,15] None of these reports was from Africa.
Objectives
To describe a series of cases of CRE at a paediatric hospital and document the clinical and microbiological experience of children with invasive CRE infection in an SA context.
Methods
A retrospective study was completed at Red Cross War Memorial Children's Hospital (RCWMCH), a tertiary referral hospital in Cape Town that cares for sick children. Microbiology specimens from children treated at RCWMCH are processed at the central National Health Laboratory Service (NHLS) laboratory at Groote Schuur Hospital (GSH), Cape Town. The NHLS microbiology database at GSH was searched for minimum inhibitory concentration (MIC) breakpoints confirming the presence of phenotypic carbapenem resistance of Enterobacteriaceae isolates in patients hospitalised at RCWMCH during the period January 2010 -December 2015. The Clinical Laboratory Standards Institute (CLSI) MIC breakpoints used to establish carbapenem susceptibility or resistance in Enterobacteriaceae isolates are summarised in the next section.[16]
Microbiological evaluation
All testing was completed at the NHLS microbiology laboratory, GSH. Identification and susceptibility testing of Enterobacteriaceae was carried out primarily with the Vitek 2 system (bioMèrieux, France) using the GN and N133 cards, respectively, supplemented where necessary with E-test (bioMérieux) to confirm the MICs of ertapenem, imipenem and meropenem.
The susceptibility of bacterial isolates was evaluated for the following antibiotics: ampicillin, amoxicillin plus clavulanic acid, piperacillin-tazobactam, cefuroxime, cefoxitin, ceftriaxone, ceftazidime, cefepime, ertapenem, meropenem, imipenem, ciprofloxacin, gentamicin, ami-kacin, co-trimoxazole, tigecycline and colistin.
Carbapenem susceptibility tests were conducted and interpreted according to the CLSI 2010 - 2015 criteria.[16] MIC breakpoints for Enterobacteriaceae were < 1 μg/mL (imipenem and meropenem) and < 0.5 μg/mL (ertapenem) for susceptible isolates, 2 μg/mL (imipenem and meropenem) and 1 μg/mL (ertapenem) for intermediately resistant isolates, and > 4 μg/mL (imipenem and meropenem) and >2 μg/mL (ertapenem) for resistant isolates.
Detection of specific carbapenemase genes was carried out by the Centre for Opportunistic, Tropical and Hospital Infections of the National Institute of Communicable Diseases, using in-house polymerase chain reaction assays. DNA was extracted from cultured isolates using the ZR-96 Fungal/Bacterial DNAkit (Zymo Research, Inqaba, SA). The following carbapenemase genes were targeted: blaNDM, blaVIM,blaIMP,blaKPC,blaGES and blaOXA-48-like
Case definitions
Invasive CRE infection was diagnosed when CRE was isolated from any given body site (other than rectal/faecal swab culture) that was associated with clinical manifestations of infection. Hospital-acquired infection was defined as CRE infection detected >48 hours after hospital admission and not incubating at the time of hospitalisation. Healthcare-associated infection was defined as CRE infection detected within 48 hours of hospitalisation in children who had contact with the healthcare service, including admission to an intermediate-care facility within the previous 12 months. Community-acquired infection was defined as CRE infection detected within 48 hours of hospital admission without previous contact with the healthcare service.[17]
Data collection
Clinical information was extracted from the hospital records of children with infection caused by CRE, including age, gender, clinical manifestations at the time of the CRE culture result, HIV status, and antibiotic use during the 12-month period preceding CRE infection, antibiotic treatment of the CRE infection and outcome of the CRE infection. Microbiological information on the CRE isolates cultured from children infected or colonised with CRE was extracted from the NHLS microbiology database and included genus and species, results of selective carbapenemase gene screening and the antibiotic sensitivity pattern. All data were entered on standardised datasheets.
Data analysis
Data were transferred anonymously to an Excel 2010 spreadsheet (Microsoft, USA) and analysed using descriptive statistical methods.
Ethical considerations
The study was approved by the Human Research Ethics Committee, Faculty of Health Sciences, University of Cape Town (reference number: HREC/REF 909/2014), and was conducted in accordance with the Declaration of Helsinki.
Results
The first invasive CRE infection at RCWMCH was recorded in November 2012. A further 9 children developed invasive infection caused by CRE during the study period, 1 in 2013, 3 in 2014 and 5 in 2015.
Clinical features of CRE infections
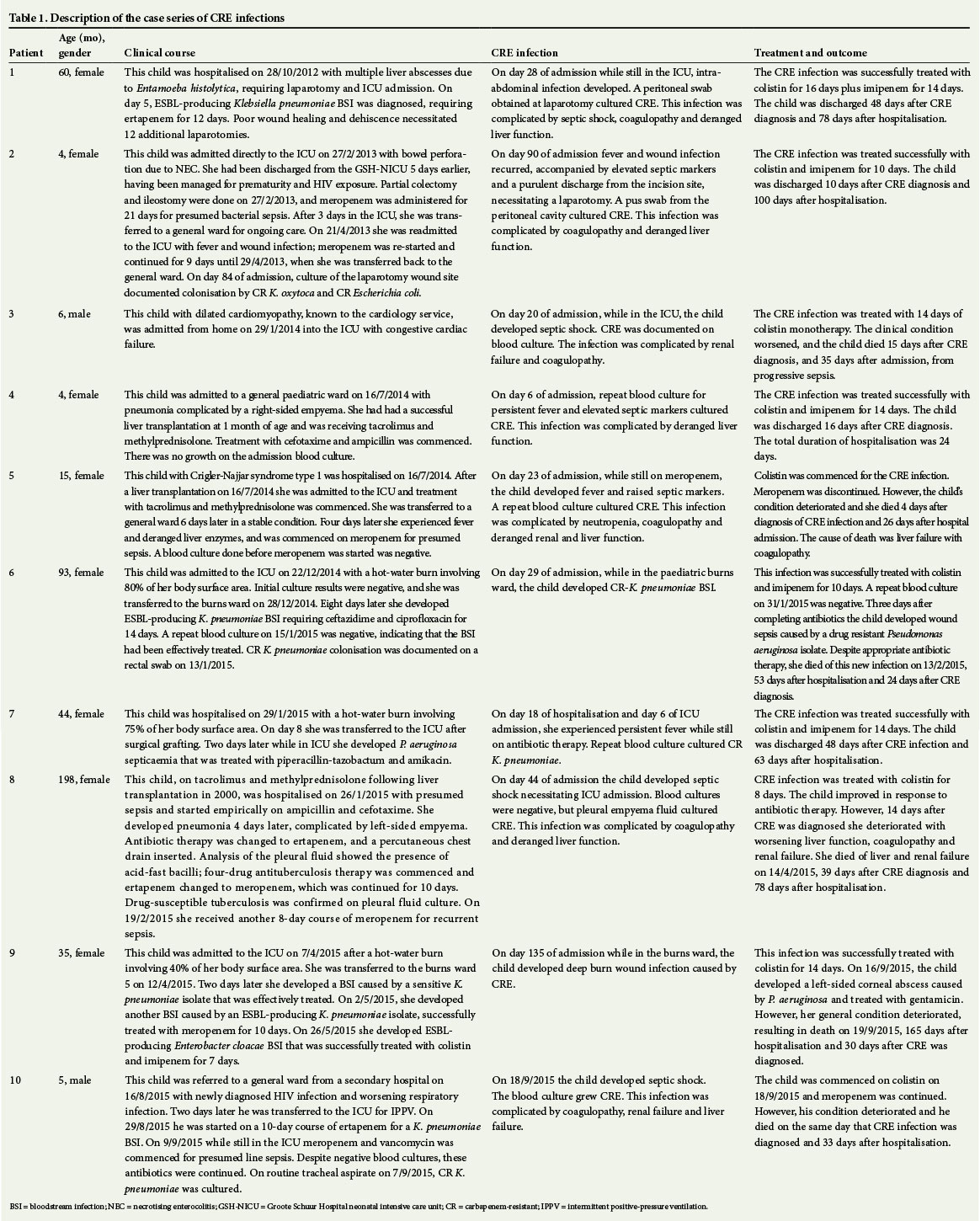
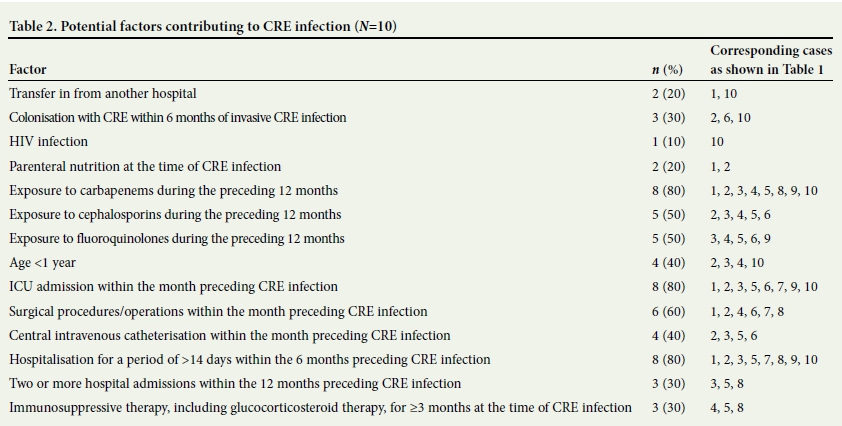
The 10 cases in this series are described in detail in Table 1. The median age was 25 months (interquartile range (IQR) 5 - 60). All 10 children were hospitalised for >48 hours before the onset of their CRE infection, implying that all 10 CRE infections were hospital acquired. The median length of hospitalisation before CRE infection was 28.5 days (IQR 20 - 44). Six of the children developed bloodstream infection, 2 manifested with intra-abdominal sepsis, 1 had sepsis and empyema and 1 had deep-seated burn wound infection (Table 1). Four of the 10 children developed CRE infection in the paediatric ICU. Table 2 summarises potential factors contributing to CRE infection.
Five children with CRE infection were treated with parenteral colistin (colistimethate sodium, Sanofi), hereafter referred to as colistin) and imipenem combination therapy, and 1 child with colistin and meropenem combination therapy. Of these 6 patients, 1 died of a non-CRE event and one from CRE infection. The remaining 4 children were treated with colistin monotherapy. All died, 2 from CRE infection (patients 3 and 5) and 2 from non-CRE events after treatment with colistin monotherapy (patients 8 and 9) (Table 1). According to the susceptibility profiles of the pathogens causing invasive CRE infection in these patients (Table 3), 1 might have benefited from colistin-carbapenem combination therapy (patient 5), and 2 from colistin-amikacin combination therapy (patients 3 and 8).
Microbiological characterisation of CRE isolates
Nine CRE infections were caused by K. pneumoniae, while the infection in patient 2 was caused by both K. pneumoniae and Escherichia coli (Table 3). Carbapenamase genes were identified in isolates from 4 of the 8 patients screened. Three and 5 of the
11 isolates were sensitive to meropenem and imipenem, respectively. None of the isolates was sensitive to ertapenem. Furthermore, 6/11 (54.5%) and 7/11 (63.6%) of the isolates had MICs < 4 μg/mL for meropenem and imipenem, respectively. All 11 isolates were susceptible to colistin and 5 were sensitive to amikacin.
CRE gastrointestinal colonisation
Between 18 May and 29 July 2013, 48 children who had been treated in the ward where patient 2 manifested with CRE were screened for CRE colonisation by rectal swab culture. Faecal colonisation with CRE isolates carrying the NDM gene was documented in 4/48 (8.3%). One was colonised by a K. oxytoca isolate, 1 by a K. pneumoniae isolate and 2 by E. coli isolates. Of the remaining 44 children, 1 was colonised by a carbapenem-resistant K. pneumoniae isolate carrying a GES gene, and another by a carbapenem-resistant E. coli isolate. This E. coli isolate was Hodge test-positive, suggesting that it produced a carbapenemase, but none of the six common carbapenemase genes was detected.
Discussion
This is one of the very first studies to report on the outcome of invasive CRE infection among children in an African setting. Since the first invasive CRE infection was diagnosed at our hospital in November 2012, there has been a steady increase in the annual number of cases. The emergence of CRE infection to some extent follows a change in the empirical antibiotic policy for hospital-acquired sepsis. At the beginning of 2012, because of escalating numbers of hospital-acquired infections caused by ESBL-producing Enterobacteriaceae, empirical antibiotic cover for hospital-acquired infections was changed from piperacillin-tazobactam plus amikacin to a carbapenem, usually ertapenem or, where appropriate, meropenem.[18,19] High carbapenem exposure during the 12-month period before the development of CRE infection in the 10 patients, together with a general increase in carbapenem use at our hospital over time (data not shown), probably contributed to the emergence of carbapenem-resistant isolates in the local microflora. Other contributory factors include exposure to other antibiotic classes, particularly cephalosporins and fluoroquinolones, prolonged hospitalisation (for > 4 weeks) before the development of CRE infection in 6 of the 10 children, prior faecal colonisation with CRE in 3 patients, and suboptimal infection control practice.[20]
Inadequate infection control practice was demonstrated during the investigation of contacts of patient 2. Of 48 children who were in contact with this patient, 4 were asymptomatically colonised with Enterobacteriaceae carrying the same carbapenemase gene as patient 2. We cannot be certain that colonisation occurred as a result of direct transfer from patient 2. However, it is likely that some were colonised through direct transfer, given that CRE is easily transmitted between humans if adequate containment measures are not implemented, and because these children were managed in close proximity to patient 2. [21] Colonisation of multidrug-resistant pathogens, including CRE, may persist for lengthy periods. In one study of 51 infants colonised with ESBL-producing K. pneumoniae, the median faecal carriage time was 12.5 months and carriage persisted for up to 24 months.[22] In another study, of adults in post-acute facilities, faecal carriage of carbapenem-resistant K. pneumoniae persisted for >10 months in 30% of colonised patients.[23] Persistent carriage is therefore an important reservoir for the spread of these organisms. Screening also identified 2 patients in contact with patient 2 who were colonised by CRE isolates unrelated to that of patient 2, indicating that asymptomatic faecal carriage among hospitalised children may be widespread, and may have contributed to the emergence of CRE infections at our hospital. Prolonged hospitalisation and previous admission to an ICU in most of our patients provided the opportunity for acquiring CRE from asymptomatic carriers.
In vitro studies have shown enhanced activity against CRE isolates with antibiotic combination therapy.[4] Observational studies have documented inconsistent outcomes following mono- or combined therapy. In one review of case reports and case series, polymyxin monotherapy was associated with higher treatment failure rates than combination therapy.'[24] However, a systematic review of 20 non-randomised studies showed a mortality rate of up to 67% among patients who received colistin-carbapenem combination therapy; among patients treated with monotherapy, the mortality rate was up to 57% for colistin and up to 80% for tigecycline.'[25] Observational studies suggest that combination therapy is superior in patients with severe infections caused by CRE.[4 ,26] Despite these inconsistencies, there is strong support for using combination therapy when treating invasive CRE infection. Various combinations have been used, including colistin plus a carbapenem, colistin plus tigecycline, colistin plus an aminoglycoside, or colistin plus a carbapenem plus tigecycline. When combining colistin with a carbapenem, an additive effect may be achieved if the carbapenem MIC is < 4 μg/mL and possibly if it is < 8 μg/mL.[4] Six of the children in the current case series were treated with combination therapy comprising colistin plus a carbapenem. In 5 of these, the MICs of the carbapenem-resistant isolates for imipenem and/or meropenem were < 4 μg/mL. The isolate of the remaining child (patient 6) had very high meropenem and imipenem MICs. This child's CRE infection was treated successfully, but she died of a subsequent Pseudomonas aeruginosa infection (Table 1). All 4 children who were treated with colistin monotherapy died. The antibiotic sensitivity profiles of their isolates (Table 3) showed that combination antibiotic options existed for 3 of these children. Why combination therapy was not prescribed is not clear from their clinical notes.
Six of the 10 children died, 3 from non-CRE-related events after the treatment of their CRE infections. The CRE-related mortality rate of 30% was higher than the crude mortality reported in recent paediatric studies, but lower than the mortality recorded in many adult studies.[4,13-15,25] Higher mortality in the present case series may be due to the small sample size, severe underlying illness, and the administration of colistin monotherapy to 40% of the children.
Conclusions
This study has provided useful insights about the patients who acquire CRE infection at our hospital and their response to treatment. Until randomised controlled trials define optimal treatment strategies, CRE infection manifesting in children with severe underlying disease such as those described in our case series must be treated with combination antibiotic therapy to optimise outcomes. Attention should be focused on improving infection control practice to contain the spread of CRE isolates, and intensifying antibiotic stewardship to reduce unnecessary antibiotic selection pressure and in so doing restrict the number of CRE infections.
Acknowledgements. The authors thank all the children in this study, their caregivers and the medical personnel who attended to them.
References
1. Yigit H, Queenan AM, Anderson GJ, et al. Novel carbapenem-hydrolyzing beta-lactamase, KPC-1, from a carbapenem-resistant strain of Klebsiella pneumoniae. Antimicrob Agents Chemother 2001;45(4):1151-1161. DOI:10.1128/AAC.45.4.1151-1161.2001 [ Links ]
2. Chen L, Mathema B, Chavda KD, et al. Carbapenemase-producing Klebsiella pneumoniae: Molecular and genetic decoding. Trends Microbiol 2014;22(12):686-696. DOI:10.1016/j.tim.2014.09.003 [ Links ]
3. Nordmann P, Naas T, Poirel L. Global spread of carbapenemase-producing Enterobacteriaceae. Emerg Infect Dis 2011;17(10):1791-1798. DOI:10.3201/eid1710.110655 [ Links ]
4. Tängdén T, Giske CG. Global dissemination of extensively drug-resistant carbapenemase-producing Enterobacteriaceae: Clinical perspectives on detection, treatment and infection control. J Intern Med 2015;277(5):501-512. DOI:10.1111/joim.12342 [ Links ]
5. Brink AJ, Coetzee J, Clay C, et al. Emergence of New Delhi metallo-beta-lactamase (NDM-1) and Klebsiella pneumoniae carbapenemase (KPC-2) in South Africa. J Clin Microbiol 2012;50(2):525-527. DOI:10.1128/JCM.05956-11 [ Links ]
6. Brink AJ, Coetzee J, Clay C, et al. The spread of carbapenem-resistant Enterobacteriaceae in South Africa: Risk factors for acquisition and prevention. S Afr Med J 2012;102(5):599-601. [ Links ]
7. Marchaim D, Navon-Venezia S, Schwaber MJ, et al. Isolation of imipenem-resistant Enterobacter species: Emergence of KPC-2 carbapenemase, molecular characterization, epidemiology, and outcomes. Antimicrob Agents Chemother 2008;52(4):1413-1418. DOI:10.1128/AAC.01103-07 [ Links ]
8. Cendejas E, Gómez-Gil R, Gómez-Sánchez P, et al. Detection and characterization of Enterobacteriaceae producing metallo-beta-lactamases in a tertiary-care hospital in Spain. Clin Microbiol Infect 2010;16(2):181-183. DOI:10.1111/j.1469-0691.2009.02888.x [ Links ]
9. Oteo J, Hernández-Almaraz JL, Gil-Antón J, et al. Outbreak of vim-1-carbapenemase-producing Enterobacter cloacae in a pediatric intensive care unit. Pediatr Infect Dis J 2010;29(12):1144-1146. DOI:10.1097/INF.0b013e3181efaa2d [ Links ]
10. Seema K, Ranjan Sen M, Upadhyay S, et al. Dissemination of the New Delhi metallo-ß-lactamase-1 (NDM-1) among Enterobacteriaceae in a tertiary referral hospital in north India. J Antimicrob Chemother 2011;66(7):1646-1647. DOI:10.1093/jac/dkr180 [ Links ]
11. Marchaim D, Chopra T, Perez F, et al. Outcomes and genetic relatedness of carbapenem-resistant entero- bacteriaceae at Detroit medical center. Infect Control Hosp Epidemiol 2011;32(9):861-871. DOI:10.1086/661597 [ Links ]
12. Little ML, Qin X, Zerr DM, et al. Molecular diversity in mechanisms of carbapenem resistance in paediatric Enterobacteriaceae. Int J Antimicrob Agents 2012;39(1):52-57. DOI:10.1016/j.ijantimicag.2011.09.01413. [ Links ]
13. Logan LK. Carbapenem-resistant Enterobacteriaceae: An emerging problem in children. Clin Infect Dis 2012;55(6):852-859. DOI:10.1093/cid/cis543 [ Links ]
14. Limbago BM, Rasheed JK, Anderson KF, et al. IMP-producing carbapenem-resistant Klebsiella pneumoniae in the United States. J Clin Microbiol 2011;49(12):4239-4245. DOI:10.1128/JCM.05297-11 [ Links ]
15. Dirajlal-Fargo S, DeBiasi R, Campos J, et al. Carbapenem-resistant Enterobacteriaceae in pediatric patients: Epidemiology and risk factors. Infect Control Hosp Epidemiol 2014;35(4):447-449. DOI:10.1086/675593 [ Links ]
16. Clinical Laboratory Standards Institute. Performance Standard for Antimicrobial Susceptibility Testing Twenty-Second Informational Supplement. CLSI document MI00-S22. Wayne, PA: CLSI, 2012. [ Links ]
17. Cardoso T, Almeida M, Friedman ND, et al. Classification of healthcare-associated infection: A systematic review 10 years after the first proposal. BMC Med 2014;12:40. DOI:10.1186/1741-7015-12-40 [ Links ]
18. Lochan H, Bamford C, Eley B. Blood cultures in sick children. S Afr Med J 2013;103(12):918-920. DOI:10.7196/SAMJ.6979 [ Links ]
19. Nuttall J, Whitelaw A. Red Cross War Memorial Children's Hospital (RCWMCH) antimicrobial recommendations. 2012. http://www.paediatrics.uct.ac.za/sites/default/files/image_tool/images/38/Antimicrobial_Recommendations_2012.pdf (accessed 12 December 2015). [ Links ]
20. Guh AY, Limbago BM, Kallen AJ. Epidemiology and prevention of carbapenem-resistant Enterobacteriaceae in the United States. Expert Rev Anti Infect Ther 2014;12(5):565-580. DOI: 1586/14787210.2014.902306 [ Links ]
21. Centers for Disease Control and Prevention. Facility Guidance for control of carbapenem-resistant Enterobacteriaceae (CRE). November 2015. http://www.cdc.gov/hai/pdfs/cre/CRE-guidance-508.pdf (accessed 10 December 2015). [ Links ]
22. Löhr IH, Rettedal S, Natas OB, et al. Long-term faecal carriage in infants and intra-household transmission of CTX-M-15-producing Klebsiella pneumoniae following a nosocomial outbreak. J Antimicrob Chemother 2013;68(5):1043-1048. DOI:10.1093/jac/dks502 [ Links ]
23. Ben-David D, Masarwa S, Navon-Venezia S, et al. Carbapenem-resistant Klebsiella pneumoniae in post-acute-care facilities in Israel. Infect Control Hosp Epidemiol 2011;32(9):845-853. DOI:10.1086/661279 [ Links ]
24. Lee GC, Burgess DS. Treatment of Klebsiella pneumoniae carbapenemase (KPC) infections: A review ofpublished case series and case reports. Ann Clin Microbiol Antimicrob 2012;11:32. DOI:10.1186/1476-0711-11-32 [ Links ]
25. Falagas ME, Lourida P, Poulikakos P, et al. Antibiotic treatment of infections due to carbapenem-resistant Enterobacteriaceae: Systematic evaluation of the available evidence. Antimicrob Agents Chemother 2014;58(2):654-663. DOI:10.1128/AAC.01222-13 [ Links ]
26. Qureshi ZA, Paterson DL, Potoski BA, et al. Treatment outcome of bacteremia due to KPC-producing Klebsiella pneumoniae: Superiority of combination antimicrobial regimens. Antimicrob Agents Chemother 2012;56(4):2108-2113. DOI:10.1128/AAC.06268-11 [ Links ]
 Correspondence:
Correspondence:
O O Malande
ombevaom@gmail.com
Accepted 11 May 2016.


{kind=link}
{kind=link}
{kind=link}