










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.106 n.7 Pretoria 2016
http://dx.doi.org/10.7196/samj.2016.v106i7.9861
IN PRACTICE
CASE REPORT
Resolution of a periodontoid rheumatoid pannus mass in an elderly patient treated with a rigid cervical collar: A case report and literature review
A OseniI, III; G KakavasII; M ScholzII; A PetridisII
I,MD, MSc; Division of Neurosurgery, Department of Surgery, Lagos University Teaching Hospital, Nigeria
IIMD; Department of Neurosurgery, Sana Kliniken Duisburg, Duisburg, Germany
ABSTRACT
In patients with C2 rheumatoid pannus with spinal cord compression the treatment of choice is extensive surgery either through a transoral resection of the dens axis or a dorsal stabilisation, or both. We present a case of an 11 -mm rheumatoid pannus with significant compression of the spinal cord, which failed surgical treatment with respect to dorsal stabilisation. Therefore, rigid cervical collar for 8 weeks followed by soft collar for another 4 weeks was chosen as a treatment option. During the follow-up period of 1 year, the pannus reduced significantly and the spinal cord decompressed. In cases where surgery is not an option or is technically very demanding, the alternative of cervical collar immobilisation is a satisfying option.
Rheumatoid arthritis (RA) is a multisystemic, chronic inflammatory disease that afflicts the metacarpophalangeal and metatarsophalan-geal joints. The primary pathology involves the synovium, which is thickened as a result of chronic inflammatory cell proliferation and surface cell hyperplasia. With progression of the disease, articular cartilage and bone destruction follow. This invariably manifests clinically as symmetrical peripheral polyarthritis. Involvement of the cervical spine is a highly characteristic component of RA as well as other chronic inflammatory rheumatic diseases.[1]
Cervical spine involvement is common in advanced RA.[1,2] Anterior atlantoaxial subluxation and atlantoaxial impaction are the most characteristic cervical spine disease in RA, occurring in 13 - 70% and 4 - 35% of patients, respectively, worldwide.[2] The spinal cord compression caused by the subluxation at the craniocervical junction may lead to the formation of periodontoid pannus, compromising the anteroposterior diameter of the spinal canal and causing neurological deficits.[3] Cervical spine involvement, although characteristic, is often missed by the treating physician because of problems related to the hands and feet. Non-infectious, non-tumorous retro-odontoid masses are rare, and have not been reported to compress the spinal cord extensively.[4]
Transoral transpharyngeal excision of the pannus is sometimes feasible for anterior decompression of the spinal cord; however, posterior fusion and instrumentation have been known to result in spontaneous regression of the pannus mass and symptomatic relief.[3,5] This case report illustrates that severe atlantoaxial vertical subluxation and posterior subluxation of the axis associated with RA can be managed satisfactorily with minimal surgical manipulation and prolonged immobilisation with a rigid cervical collar, thus avoiding extensive surgery in high-risk patients.
Case report
A 73-year-old woman was referred to the Department of Neurosurgery, Sana Kliniken with an already non-operative treated pannus behind C2 with seronegative polyarthritis, and clinical and radiological signs of myelopathy. She had a history of long-term cortisone use due to chronic obstructive pulmonary disease (COPD). Her symptoms dated back 2 years prior to presentation, with mild headaches, nuchalgia and burning paraesthesias in both arms - right more than left - with no associated dermatome. Paraesthesias were also noted in the upper body down to the mammary region, with no further neurological deficits.
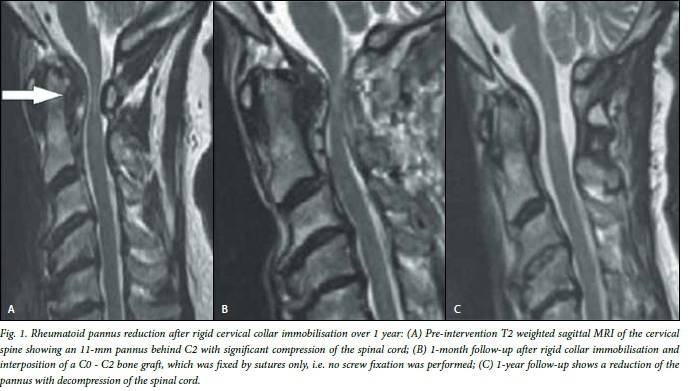
Initial care was given by our rheumatologists, owing to chronic neck pain syndrome around a crowded dens and seronegative polyarthritis. The initial visit to neurosurgical outpatient clinic confirmed the clinical findings, with radiological findings of a 11-mm pannus behind the dens, with associated compression of the medulla and a syrinx (Fig. 1). The patient was prepared for surgical decompression with preoperative planning for a C1 laminectomy and dorsal C1/C2 fusion. She underwent cervical decompression C1 laminectomy, but the planned C1/C2 fusion was not feasible due to weak pedicle bone substance found intraoperatively. Transarticular screw fixation, i.e. Magerl technique, was considered but also dropped owing to prominent vertebral artery curvature elongation and the risk of injury to the artery. With the intraoperative difficulties, it was decided to make a bone graft transplant from the dorsal iliac crest directly between C2 and the nuchal area. Fixation was achieved with non-resorbable material around C2.
Immediate postoperative computed tomography (CT) scan of the cervical spine showed a well-fixed bone graft still located at the point of fixation. According to the patient, the pain subsided, and a rigid cervical collar was applied to be maintained for 8 weeks, day and night, whereupon the patient was discharged. In the subsequent months, the patient reported every month to the outpatient clinics. She had CT scans performed every month in order to follow the progress or dislocation of the bone graft. After 8 weeks, the rigid cervical collar was changed to a soft neck brace, which allowed certain but minimal range of motion. This was maintained for 4 weeks, whereafter it was removed and the patient was allowed free range of motion. The CT scan at this point showed the bone graft no longer attached to C2, suspected to be owing to bone absorption. No dislocation was measured. A C2-to-nuchal-area distance of 5 mm was evident in all consecutive CTs. A significant decrease in the size of the pannus was noticed, from 11 mm to 5 mm, with associated reduced pain according to the patient. In subsequent CT scans, the medulla reached a normal width and myelopathy signs subsided; the patient still had burning sensation in both arms but with no measurable neurological deficit (at follow-up after 1 year). There was improved neck motion, with a postoperative rotation of 15°.
Discussion
The erosion of the ligamentous support for the odontoid peg due to rheumatoid synovitis causes atlantoaxial instability leading to compression of the upper cervical cord and brainstem. Pannus is located ventrally to the bulbomedullary junction, and can produce a severe myelopathy and even sudden death.[6] According to some studies, this is an inflammatory granulation process, whereas in others this tissue is a reactive fibrous tissue secondary to the mechanical stress, rather than secondary to an inflammatory process.[1,2,6]
The instability leads to forward subluxation, producing neurological damage. Patients with rheumatoid cervical spine involvement may have no symptoms, but more often have some nonspecific neck pain or C2 neuralgia and stiffness.[6] The symptoms of nuchal pain, and lancinating sensation with loss of power of upper and lower limb muscles indicate atlantoaxial joint disease with bursitis and subluxation of joint due to RA.[1,6]
Transoral transpharyngeal excision of the pannus is thought necessary for anterior decompression of the spinal cord by some authors;[3,5,7] however, occasional reports of spontaneous resolution of the periodontoid pannus after posterior atlantoaxial fusion and fixation have been documented.[3] Evidence suggests that atlantoaxial instability is the de facto reason for the formation of periodontoid pannus,[1,3,4,7] and as such, interventions to reduce the instability lead to spontaneous resolution of the pannus mass.[3,6,8]
Posterior atlantoaxial fixation is a viable option especially in older patients with significant myelopathy from soft-tissue compression, and may prevent the need for removal of the panus through the transoral route. However, there are no reports of strictly conservative treatment with only cervical collar immobilisation showing such a significant reduction of the pannus, as in the present case report. In cases were surgery is not an option or is technically very demanding, the alternative of cervical collar immobilisation with a rigid collar for 8 weeks followed by a soft collar for another 4 weeks is a satisfying option. Monthly follow-up with CT scanning every month for the first 3 months and thereafter every 2 months for the first year should also be done.
References
1. Prakash P, Srivastava S, Sharma SC, et al. Cervical complications of rheumatoid arthritis. JIACM 2006;7(2):161-164. [ Links ]
2. Daoud L, Kochbati S. Magnetic resonance imaging evaluation of the cervical spine in patients with rheumatoid arthritis. Report of 30 cases. La Tunisie Medi (6):375-379. [ Links ]
3. Lu K, Lee TC. Spontaneous regression of periodontoid pannus mass in psoriatic atlantoaxial subluxation. Case report. Spine 1999;15;24(6):578-581. [ Links ]
4. Takuechi M, Yasuda M, Takahashi E. A large retro-odontoid cystic mass caused by transverse ligament degeneration with atlantoaxial subluxation leading to granuloma formation and chronic recurrent microbleeding. Case report. Spine J 2011;11(12):1152-1156. DOI:10.1016/j.spinee.2011.11.007 [ Links ]
5. Jun BY. Complete reduction of retro-odontoid soft tissue mass in os odontoideum following the posterior C1-C2 transarticular screw fixation. Spine 1999;15:24(18);1961-1964. [ Links ]
6. Lagares A, Arrese I, Pascual B, et al. Pannus resolution after occipitocervical fusion in a non-rheumatoid atlanto-axial instability. Eur Spine J 2006;15(3):366-369. DOI:10.1007/s00586-005-0969-4 [ Links ]
7. Isono M, Ishii K, Kamida T, et al. Retro-odontoid soft tissue mass associated with atlantoaxial subluxation in an elderly patient: A case report. Surg Neurol 2001;55(4):223-227. [ Links ]
8. Sasaki T, Miyamoto K, Hosoe H, Shimizu K. Transoral anterior approach for extensive anterior decompression at the C3 vertebra level in a patient with severe atlantoaxial vertical subluxation and rheumatoid arthritis. Spinal Cord 2006;44(1):52-55. [ Links ]
 Correspondence:
Correspondence:
A Oseni
oseniabidemi@yahoo.com
Accepted 4 May 2016.


{kind=link}