










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.106 n.6 Pretoria Jun. 2016
http://dx.doi.org/10.7196/samj.2016.v106i6.10340
RESEARCH
Clinical findings and genetic screening for copy number variation mutations in a cohort of South African patients with Parkinson's disease
A C MahneI; J A CarrII; S BardienIII; C-M SchutteIV
IMB ChB, MMed (Neurol); Department of Neurology, School of Medicine, Faculty of Health Sciences, University of Pretoria, South Africa
IIMB ChB, PhD; Division of Neurology, Faculty of Medicine and Health Sciences, Stellenbosch University, Tygerberg, Cape Town, South Africa
IIIPhD; Division of Molecular Biology and Human Genetics, Faculty of Medicine and Health Sciences, Stellenbosch University, Tygerberg, Cape Town, South Africa
IVMB ChB, MMed (Neurol), MD; Department of Neurology, School of Medicine, Faculty of Health Sciences, University of Pretoria, South Africa
ABSTRACT
BACKGROUND. Parkinson's disease (PD), with a prevalence of up to 4% in Western countries, appears to be less common in Africa, possibly in part because of genetic factors. African studies investigating the genetic causation of PD are limited.
OBJECTIVE. To describe the clinical and genetic findings in a group of black South African patients with PD.
METHODS. All black African patients with PD from a tertiary hospital neurology clinic were examined. Symptoms were scored according to the Unified Parkinson's Disease Rating Scale (UPDRS), and patients were classified according to motor features. Genomic DNA was extracted and multiplex ligation-dependent probe amplification was used for detection of copy number variation (CNV) mutations in the known PD-causing genes.
RESULTS. Sixteen patients were identified (ages 56 - 82 years). Three had a family history of PD. Classification into motor subtypes showed 44% mixed, 31% akinetic-rigid, and 25% tremor-dominant subtypes. UPDRS scores ranged from 7 to 88, with dementia in 20%. No patient had G2019S LRRK2 and A30P SNCA mutations, and all except one had no CNV mutations in the known PD-causing genes. A female patient (age of onset 50 years, no family history) had a parkin gene heterozygous deletion of exon 4. She had hyperreflexia, bilateral Hoffmann's reflexes, normal plantar responses and no dystonia.
CONCLUSION. This group of black African patients showed similar characteristics to patients in Western studies, possibly with a higher proportion having tremor-dominant disease. Genetic analysis showed one parkin gene mutation. The limited knowledge on PD-causing genes and mutations in black populations warrants further studies involving next-generation sequencing approaches.
Parkinson's disease (PD) is a chronic progressive neurodegenerative disorder characterised by bradykinesia, rigidity, resting tremor and postural instability resulting from a central nervous system dopamine deficiency. Worldwide it is a common disorder, affecting 1 - 2% of the population aged >60 years.[1] The prevalence may rise to 4% in higher age groups in Western countries, but the prevalence of the disease in Africa was reported to be much lower at 7 - 43/100 000.[2] This low prevalence in the black African population is supported by studies comparing the prevalence between an American population (341/100 000), a Nigerian population (67/100 000) and a Tanzanian population (40/100 000). The reasons for these observations are still unclear, but environmental factors, shorter life expectancy and undiagnosed disease may play a role.[3,4] Whereas no epidemiological studies on PD in South Africa (SA) are available, the impression among practising neurologists is certainly that PD is seen more commonly in the white population. The low prevalence in black populations may be related to genetic factors. During the past decade, increasing evidence that genetic factors play an essential role in the development of PD has emerged. About 10% of patients with PD show a Mendelian pattern of inheritance, with several genes being identified as having a causal relationship;[5] these include SNCA, parkin, DJ-1, PINK1, LRRK2, VPS35 and EIF4G1.
Studies from Africa that have looked at an association between PD and gene mutations are limited, and this report describes the clinical findings of a group of black SA patients with PD who were screened for copy number variation (CNV) mutations in the known PD-causing genes. Whole-exon deletions or duplications, primarily in the parkin gene, are a common cause of PD and have been found in both familial and sporadic forms of the disorder.[6]
Methods
All black African patients with a diagnosis of PD who were being followed up at the neurology clinic at Steve Biko Academic Hospital, Pretoria, SA, were included in the study. The patients were invited to participate in the study, and informed consent and ethical committee approval of the University of Pretoria (Ref. No. 128/2012) were obtained. The patients were evaluated by a clinician proficient in the neurological examination of patients with PD to confirm that they met the UK Parkinson's Disease Society Brain Bank clinical diagnostic criteria for PD. History and demographic data were obtained, and after a full neurological examination, symptoms were scored according to the Unified Parkinson's Disease Rating Scale (UPDRS). Atypical features were noted and patients were classified according to age at onset, cognitive functioning and motor features.
Venous blood (20 mL) was obtained and genomic DNA was extracted. The multiplex ligation-dependent probe amplification (MLPA) method was used for detection of CNV mutations. Specifically, the commercially available SALSA P051-D1 Parkinson kit (MRC-Holland, Netherlands) was used. This kit contains probes for all exons of genes in which PD-causing CNV mutations have previously been found, including parkin, PINK1, DJ-1 and SNCA. In addition, the kit contains probes for detection of two point mutations, G2019S in LRRK2 and A30P in SNCA. The MLPA experiments were performed according to the manufacturer's instructions and the amplified products were analysed on a 3130x1 Genetic Analyser (Applied Biosystems, USA). Coffalyser.Net software (v14072.1958, MRC-Holland, Netherlands) was used for copy number calculations.
Results
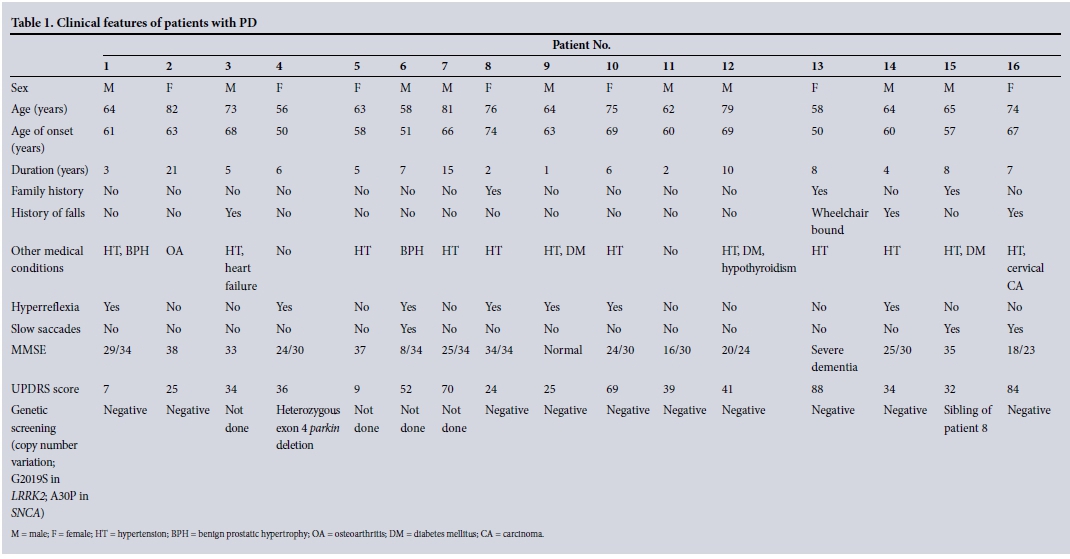
Sixteen black patients with PD were identified (9 males and 7 females), 2 of them siblings. Most patients were Sotho speakers (9/16), the rest speaking Zulu or Ndebele. Their ages ranged from 56 to 82 years (mean 68), disease duration from 1 to 21 years (mean 6.8) and age of onset of the disorder from 50 to 74 years; a family history of PD was obtained in 3 patients (19%), the 2 siblings and 1 other patient. Classification according to motor features showed 44% to be mixed, 31% akinetic-rigid and 25% tremor-dominant subtypes. UPDRS scores when on medication ranged from 7 to 88; tremor graded according to the UPDRS was scored as 1 (slight and infrequent) in 4 participants (25%), 2 (mild and impersistent) in 6 (38%), 3 (moderate and mostly present) in 4 (25%) and 4 (marked and mostly present) in 2 (13%). The rigidity score was 1 in 25%, 2 in 50% and 3 in 25%, and the bradykinesia score was 1 in 44%, 2 in 25%, 3 in 13% and 4 in 19%.
Cognitive screening using the mini-mental state examination (MMSE) showed normal cognition in 40% and minimal cognitive impairment in 40%, while 20% had dementia. Patients with cognitive impairment showed a greater mean rigidity score (2.33) as derived from the UPDRS than patients without dementia (1.5). Interestingly, hyperreflexia was found in 7/16 patients (44%), and slowing of saccadic eye movements was seen in 2. The clinical findings are set out in Table 1.
Genetic screening was performed on 11 unrelated patients for whom DNA was available. Importantly, both the G2019S LRRK2 and A30P SNCA mutations were excluded as a cause of the disorder in all the patients. In 10 patients, no CNV mutations were found; however, in one patient a heterozygous deletion of parkin exon 4 was identified. This patient (Table 1, patient 4) had an age of onset of 50 years with no family history of the disorder. In addition to the signs of PD, she was also noted to have hyperreflexia with bilateral Hoffmann's reflexes, but normal plantar responses. No dystonia was noted, and a computed tomography scan of the brain did not show any focal lesions.
Discussion
PD is one of the commonly occurring neurodegenerative disorders, yet little information about this disease in black African patients is available and clinical and genetic studies involving these patients are limited.
It is well known that PD is mainly seen in older individuals, with the incidence rising with every decade of age; worldwide, ~4 - 10% of patients have early-onset disease.[7] Compared with patients with PD from Zambia, in whom the mean age of onset was 54 years,[8] and a group of 18 black SA patients with PD with a mean age of onset of 52 years,[9] our patients' mean age of onset at 62.5 years was slightly older; it is, however, comparable to the average age of onset of 62 years in Western studies. There were no patients with young-onset (defined as <50 years) PD in our group, but this may be a reflection of the small sample size.
Clinical classifications of motor subtypes in PD in Western population studies show a mixed subtype of disease as the most common presentation (66%), followed by the akinetic-rigid subtype (26%) and lastly the tremor-dominant group (8%).[10] Our patients showed a similar pattern, but the tremor-dominant group was larger at 25%. This is comparable to a group of Nigerian patients with PD, 55% of whom had mixed disease, 32% tremor-dominant disease and 14% the akinetic-rigid form.[11] Eventually this may have prognostic implications, as some studies have shown that patients with tremor-dominant disease may have a more favourable course.[12]
Cognitive impairment and dementia may occur in patients with PD, especially after long disease duration. Generally, patients with PD have an almost six-fold increased risk of developing dementia, and up to 24 - 31% have cognitive impairment.[13] Of our group of patients, 20% had dementia; these patients all also had high UPDRS scores (>35). Severe motor disorders such as rigidity and gait instability have been linked to an increased probability of developing dementia, and this appeared to be the case in our patients, among whom the mean rigidity score was high in those who were cognitively impaired (2.33 v. 1.5 in non-demented patients), but larger numbers of patients need to be studied to confirm this association. An older age at disease onset was not found to be a risk factor for dementia in our study (ages 50, 60 and 51 years at disease onset in the patients with dementia). Disease duration, age of onset and motor symptom severity have been found to be risk factors in some studies, but others have not confirmed these associations.[14]
There is currently increasing evidence that genetic factors are important in the development of PD, and up to 10% of cases are believed to have a genetic cause. Genes associated with an autosomal dominant pattern of inheritance include SNCA and LRRK2, while autosomal recessively inherited gene abnormalities include parkin, DJ-1, PINK1 and ATP13A2.[5] Whereas SNCA and parkin mutations are usually associated with early-onset PD, LRRK2 mutations, specifically the G2019S mutation[15] (which was not found in our study), are the most frequent cause of late-onset familial and sporadic PD. A positive family history was found in up to 2.4% of black African patients in case series,[16] and one SA study of a mixed group of patients found an overall positive family history in approximately one-third of individuals with late-onset PD.[9]
Conclusion
Although the number of patients in our study was small, three reported a positive family history, and only one of the patients (who had reported no family history) had a pathogenic CNV mutation in the parkin gene. As parkin is associated with an autosomal recessive form of PD, further studies are warranted to possibly identify a second pathogenic mutation in this patient.
To date, only two black SA patients have been shown to harbour mutations in the parkin gene and none have had mutations in any of the other PD-causing genes.[17,18] These findings suggest that unravelling the genetics of PD is still only in the early stages, and further studies for new candidate genes are needed. Future studies will involve whole-exome sequencing of DNA from our patients to identify defects in potentially novel PD-causing genes.
Acknowledgments. We thank Genevie Borrageiro for performing the MLPA experiments and Prof. E Janse van Rensburg from the Department of Human Genetics, University of Pretoria, for extraction of the patients' DNA.
Conflicts of interest. None. SB has been awarded grants from the South African Medical Research Council and the National Research Foundation.
Author contributions. C-MS and ACM did the initial planning, conduct and reporting and writing up of the work, SB was in charge of the genetic part of the work and helped with the final drafting of the article, and JAC was involved in the final writing up and editing of the article. All the authors saw and approved the final article.
References
1. Tanner CM, Goldman SM. Epidemiology of Parkinson's disease. Neurol Clin 1996;14(2):317-335. [ Links ]
2. Okubadejo NU. An analysis of genetic studies of Parkinson's disease in Africa. Parkinsonism Relat Disord 2008;14(3):177-182. DOI:10.1016/j.parkreldis.2007.08.006 [ Links ]
3. Schoenberg BS, Osuntukun BO, Adeuja AO, et al. Comparison of the prevalence of Parkinson's disease in black populations in the rural United States and in rural Nigeria: Door-to-door community studies. Neurology 1988;38(4):645-646. [ Links ]
4. Dotchin C, Msuya O, Kissima J, et al. The prevalence of Parkinson's disease in rural Tanzania. Mov Disord 2008;23(11):1567-1572. DOI:10.1002/mds.21898 [ Links ]
5. Trinh J, Farrer M. Advances in the genetics of Parkinson disease. Nat Rev Neurol 2013;9(8):445-454. DOI:10.1038/nrneurol.2013.132 [ Links ]
6. Ambroziak W, Koziorowski D, Duszyc K, et al. Genomic instability in the PARK2 locus is associated with Parkinson's disease. J Appl Genet 2015;56(4):451-461. DOI:10.1007/s13353-015-0282-9 [ Links ]
7. Van den Eeden SK, Tanner CM, Bernstein AL, et al. Incidence of Parkinson's disease: Variation by age, gender, and race/ethnicity. Am J Epidemiol 2003;157(11):1015-1022. DOI:10.1093/aje/kwg068 [ Links ]
8. Atadzhanov M. Phenotypic characteristics of Zambian patients with Parkinson's disease. Med J Zambia 2010;37(3):160-165. [ Links ]
9. Van der Merwe C, Haylett W, Harvey J, Lombard D, Bardien S, Carr J. Factors influencing the development of early- or late-onset Parkinson's disease in a cohort of South African patients. S Afr Med J 2012;102(11):848-851. DOI:10.7196/SAMJ.5879 [ Links ]
10. Rajput AH, Voll A, Rajput ML, Robinson CA, Rajput A. Course in Parkinson disease subtypes: A 39-year clinicopathologic study. Neurology 2009;73(3):206-212._DOI:10.1212/WNL.0b013e3181ae7af1 [ Links ]
11. Okubadejo NU, Oluwadamilola OO, Olajumoke OO. Clinical profile of parkinsonism and Parkinson's disease in Lagos, southwestern Nigeria. BMC Neurol 2010;10:1. DOI:10.1186/1471-2377-10-1 [ Links ]
12. Eggers C, Pedrosa DJ, Kahraman D, et al. Parkinson subtypes progress differently in clinical course and imaging pattern. PLoS One 2012;7(10):e46813. DOI:10.1371/journal.pone.0046813 [ Links ]
13. Aarsland D, Anderson K, Larsen JP, et al. Risk of dementia in Parkinson's disease: A community-based, prospective study. Neurology 2001;56(6):730-736. DOI:10.1212/WNL.56.6.730 [ Links ]
14. Aarsland D, Kurz MW. The epidemiology of dementia associated with Parkinson's disease. Brain Pathol 2010;20(3):633-639. DOI:10.1111/j.1750-3639.2009.00369.x [ Links ]
15. Correia Guedes L, Ferreira JJ, Rosa MM, Coelho M, Bonifati V, Sampaio C. Worldwide frequency of G2019S LRRK2 mutation in Parkinson's disease: A systematic review. Parkinsonism Relat Disord 2010;16(4):237-242. DOI:10.1016/j.parkreldis.2009.11.004 [ Links ]
16. Osuntukun BO, Bademosi O. Parkinsonism in the Nigerian African: A prospective study of 217 patients. East Afr Med J 1979;56(11):597-607. [ Links ]
17. Haylett WL, Keyser RJ, du Plessis MC, et al. Mutations in the parkin gene are a minor cause of Parkinson's disease in the South African population. Parkinsonism Relat Disord 2012;18(1):89-92. DOI:10.1016/j.parkreldis.2011.09.022 [ Links ]
18. Blanckenberg J, Bardien S, Glanzmann B, Okubadejo NU, Carr JA. The prevalence and genetics of Parkinson's disease in sub-Saharan Africans. J Neurol Sci 2013;335(1-2):22-25. DOI:10.1016/j.jns.2013.09.010 [ Links ]
 Correspondence:
Correspondence:
C-M Schutte
cschutte@medic.up.ac.za, clara.schutte@up.ac.za
Accepted 23 February 2016.


{kind=link}