










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSAMJ: South African Medical Journal
versión On-line ISSN 2078-5135
versión impresa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.106 no.6 Pretoria jun. 2016
http://dx.doi.org/10.7196/samj.2016.v106i6.9863
RESEARCH
A meta-analysis of the efficacy of preoperative surgical safety checklists to improve perioperative outcomes
B M BiccardI; R N RodsethII, III; L CronjeIV; P AgabaV; E ChikumbaVI; L du ToitVII; Z FarinaVIII, IX; S FischerX; P D GopalanXI; K GovenderXII; J KanjeeXIII; A C KingwillXIV; F MadzimbamutoXV; D MashavaXVI; B MraraXVII; M MudelyXVIII; E NiniseXIX; J SwanevelderXX; A WabuleXXI
IPhD; Department of Anaesthesia and Perioperative Medicine, Faculty of Health Sciences, University of Cape Town, South Africa
IIPhD; Perioperative Research Group, Discipline of Anaesthesiology and Critical Care, School of Clinical Medicine, College of Health Sciences, Nelson R Mandela School of Medicine, University of KwaZulu-Natal, Durban, South Africa
IIIPhD; Clinical Department, Anaesthesia, Grey's Hospital, Pietermaritzburg, South Africa
IVFCA (SA); Perioperative Research Group, Discipline of Anaesthesiology and Critical Care, School of Clinical Medicine, College of Health Sciences, Nelson R Mandela School of Medicine, University of KwaZulu-Natal, Durban, South Africa
VMMed (Anaesth); Department of Anaesthesia and Critical Care, School of Medicine, College of Health Sciences, Faculty of Medicine, Makerere University, Uganda
VIMMed (Anaesth); Department of Anaesthesia and Critical Care Medicine, College of Health Sciences, Faculty of Medicine, University of Zimbabwe
VIIMB ChB; Department of Anaesthesia and Perioperative Medicine, Faculty of Health Sciences, University of Cape Town, South Africa
VIIIFCA (SA); Perioperative Research Group, Discipline of Anaesthesiology and Critical Care, School of Clinical Medicine, College of Health Sciences, Nelson R Mandela School of Medicine, University of KwaZulu-Natal, Durban, South Africa
IXFCA (SA); Clinical Department, Anaesthesia, Grey's Hospital, Pietermaritzburg, South Africa
XFCA (SA); Dunkeld Anaesthetic Practice, Johannesburg, South Africa
XIFCA (SA);Perioperative Research Group, Discipline of Anaesthesiology and Critical Care, School of Clinical Medicine, College of Health Sciences, Nelson R Mandela School of Medicine, University of KwaZulu-Natal, Durban, South Africa
XIIMMed (Anaesth); Perioperative Research Group, Discipline of Anaesthesiology and Critical Care, School of Clinical Medicine, College of Health Sciences, Nelson R Mandela School of Medicine, University of KwaZulu-Natal, Durban, South Africa
XIIIFCA (SA); Perioperative Research Group, Discipline of Anaesthesiology and Critical Care, School of Clinical Medicine, College of Health Sciences, Nelson R Mandela School of Medicine, University of KwaZulu-Natal, Durban, South Africa
XIVMB ChB; Department of Anaesthesiology, Faculty of Health Sciences, University of the Free State, Bloemfontein, South Africa
XVFCAECSA; Department of Anaesthesia and Critical Care Medicine, College of Health Sciences, Faculty of Medicine, University of Zimbabwe
XVIMMed (Anaesth); Private Practice, Avenues Clinic, Harare, Zimbabwe
XVIIFCA (SA); Department of Anaesthesiology, Faculty of Medicine, Walter Sisulu University, Mthatha, Eastern Cape, South Africa
XVIIIFCA (SA); Perioperative Research Group, Discipline of Anaesthesiology and Critical Care, School of Clinical Medicine, College of Health Sciences, Nelson R Mandela School of Medicine, University of KwaZulu-Natal, Durban, South Africa
XIXMB ChB; Department of Anaesthesiology, Faculty of Medicine, Walter Sisulu University, Mthatha, Eastern Cape, South Africa
XXFRCA; Department of Anaesthesia and Perioperative Medicine, Faculty of Health Sciences, University of Cape Town, South Africa
XXIMMed (Anaesth); Department of Anaesthesia and Critical Care, School of Medicine, College of Health Sciences, Faculty of Medicine, Makerere University, Uganda
ABSTRACT
BACKGROUND. Meta-analyses of the implementation of a surgical safety checklist (SSC) in observational studies have shown a significant decrease in mortality and surgical complications.
OBJECTIVE. To determine the efficacy of the SSC using data from randomised controlled trials (RCTs).
METHODS. This meta-analysis followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines and was registered with PROSPERO (CRD42015017546). A comprehensive search of six databases was conducted using the OvidSP search engine.
RESULTS. Four hundred and sixty-four citations revealed three eligible trials conducted in tertiary hospitals and a community hospital, with a total of 6 060 patients. All trials had allocation concealment bias and a lack of blinding of participants and personnel. A single trial that contributed 5 295 of the 6 060 patients to the meta-analysis had no detection, attrition or reporting biases. The SSC was associated with significantly decreased mortality (risk ratio (RR) 0.59, 95% confidence interval (CI) 0.42 - 0.85; p=0.0004; I2=0%) and surgical complications (RR 0.64, 95% CI 0.57 - 0.71; p<0.00001; I2=0%). The efficacy of the SSC on specific surgical complications was as follows: respiratory complications RR 0.59, 95% CI 0.21 - 1.70; p=0.33, cardiac complications RR 0.74, 95% CI 0.28 - 1.95; p=0.54, infectious complications RR 0.61, 95% CI 0.29 - 1.27; p=0.18, and perioperative bleeding RR 0.36, 95% CI 0.23 - 0.56; p<0.00001.
CONCLUSIONS. There is sufficient RCT evidence to suggest that SSCs decrease hospital mortality and surgical outcomes in tertiary and community hospitals. However, randomised evidence of the efficacy of the SSC at rural hospital level is absent.
Meta-analyses of the implementation of a surgical safety checklist (SSC) in observational studies have shown a significant decrease in mortality[1,2] and surgical complications.[1-4] The importance of these findings is difficult to interpret, however,[1] as these meta-analyses contain little randomised evidence,[1,3,4] with a single randomised trial of 65 patients[5] included in some of the meta-analyses. There are currently no meta-analyses of the efficacy of the SSC from randomised controlled trials (RCTs).
Despite the compelling observational data supporting SSCs, and national policy directives mandating the use of an SSC, the uptake and implementation of SSCs has been poor.[6] Improving implementation of the SSC requires local checklist champions, staff checklist training, and improving feedback to reduce checklist redundancies.[7,8] A higher level of evidence supporting SSCs, such as that from a large RCT or a meta-analysis of RCTs, may be necessary before SSCs are actively championed and successfully implemented.[8] This is important, as data suggest that correct implementation with checklist completion is more successful than partial checklist completion at reducing surgical complications.[9]
Objective
The objective of this meta-analysis was to determine the efficacy of the SSC in RCTs. Using the participants, interventions, comparisons, outcomes and study design (PICOS) method,[10] we described the participants as all categories of surgical patients, the intervention as the use of an SSC, and the comparison as the usual (or standard) operating room management. The primary outcome was mortality. Secondary outcomes included perioperative complications, which were defined as surgical complications, anaesthetic complications, length of stay and cost.
Methods
We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines[10] in conducting this meta-analysis.
Protocol and registration
A full protocol was not developed for this meta-analysis. The meta-analysis was registered with PROSPERO (CRD42015017546).
Eligibility criteria
We considered all publications of RCTs of surgical patients randomised to either an SSC or usual operating room management. There was no limit on the trial follow-up period. We accepted all publications in any language, with a comprehensive search from 1946 to 2015.
Information sources
The database searches were conducted on 6 March 2015 using the OvidSP search engine (Ovid Technologies Inc., USA) for the following databases:
• Embase, 1974 to 5 March 2015 (Scopus)
• Ovid Healthstar, 1966 to November 2014
• Ovid MEDLINE(R) In-Process and Other Non-Indexed Citations, Ovid MEDLINE(R) Daily and Ovid MEDLINE(R), 1946 to present
• Cochrane Library, March 2015
• ProQuest Dissertations and Theses A&I, March 2015.
This search was updated on 7 March 2016, and the clinicaltrials.gov database was added to this updated search.
Search
We used the following expanded search terms: 'surgery or surgical procedure operative or operating rooms or preoperative care and checklist or guideline adherence. The search was limited to RCTs. The search terms and an example of the full electronic search strategy for Ovid are shown in Appendix 1.
Study selection
The title and abstract of each citation was independently screened by two reviewers (JK and KG) to identify potentially eligible trials following the first search, and by two reviewers (BMB and RNR) following the updated search. If either reviewer considered that the citation might contain a relevant trial, the article was retrieved to undergo full text evaluation. Full texts of all citations identified as potentially relevant were then independently evaluated by all the authors to determine eligibility. Chance-corrected inter-observer agreement for trial eligibility following abstract screening was tested using kappa statistics.
Trials were deemed eligible and included in this review if they were conducted on surgical patients comparing an operating room SSC with standard or routine surgical care. There was no requirement to report any of the prespecified outcomes in the publication for inclusion in this meta-analysis, as the intention was to contact authors for any missing outcome data.
Data collection process
Data were extracted into a standardised data extraction sheet. Data extraction was conducted at a workshop. As a result, the delegates were allocated to three groups of six authors (one group per included trial) for data extraction, with any disagreements resolved by consensus following consultation with BMB (the moderator of the workshop). The authors were emailed for resolution of data queries.
Data items
For each eligible trial, the data extracted included author, year of publication, surgical group studied, number of subjects, type of SSC used, age of patients, level of hospital, country and duration of follow-up. Outcome data extracted included mortality, surgical complications, anaesthetic complications and length of stay. The study definitions for each outcome were also extracted. Authors were contacted for clarification of any missing data if necessary.
Risk of bias in individual studies
Trials were assessed using the Cochrane Collaboration risk-of-bias tool.[11] This tool assesses selection bias, allocation bias, performance bias, detection bias, attrition bias and other bias. All assessments of bias in individual studies were conducted by a group of six authors per included trial, with disagreements resolved through consensus following consultation with BMB.
Summary measures
Study characteristics were analysed using GraphPad QuickCalcs.[12] Meta-analysis was conducted using a random-effects model in Review Manager version 5.3.5 (Nordic Cochrane Centre, Denmark; Cochrane Collaboration, 2014). All analyses were based on the intention-to-treat principle.
Synthesis of results
Heterogeneity was assessed using I2and χ2 analysis. Pooled dichotomous outcomes were reported as risk ratios (RRs) and 95% confidence intervals (CIs). Continuous outcomes were reported as mean differences and 95% CIs.
Risk of bias across studies
A funnel plot to assess for the possibility of publication bias would only be presented if there were sufficient trials to warrant this. In order to exclude selective reporting by the authors, we contacted them where necessary to determine whether they had collected data on any of the outcomes of interest that were not reported in the original publication.
Additional analysis
No additional analyses were conducted.
Results
Study selection
We identified 464 citations from the combined initial and updated searches, with five selected for full-text evaluation (Fig. 1). From these, we identified three eligible RCTs that included 6 060 patients.[5,13,14] Inter-observer agreement for trial eligibility was excellent (kappa = 1.00).

Study characteristics
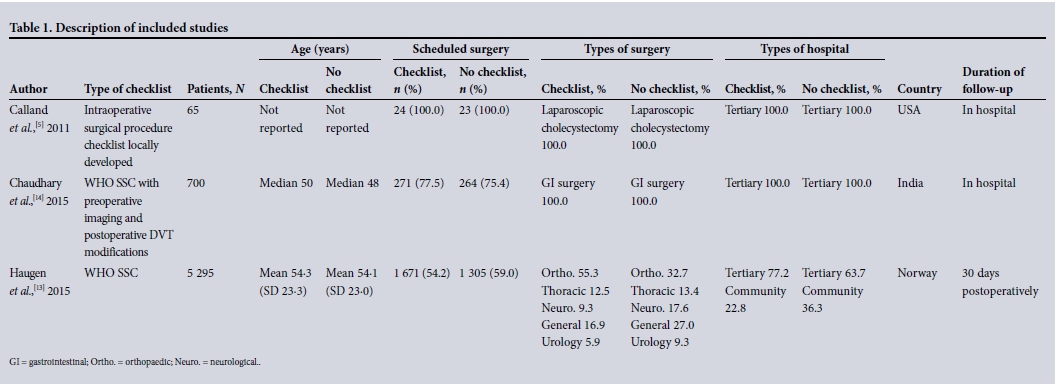
The study characteristics are presented in Table 1. Of the recruited patients, 4 554 were from tertiary hospitals[5,13,14] and 1 506 from a community hospital.[13] Two of the three trials were conducted in high-income country surgical environments, Norway and the USA,[5,13] and a single trial was conducted in a middle-income country, India.[14] There was a significant six-fold difference in mortality (p<0.0001) between the control groups of one high-income country (Norwegian) trial (1.6%; 95% CI 0.9 - 1.8%)[13] and the middle-income country (Indian) trial (10.2%; 95% CI 8.0 - 12.4%).[14]
The SSCs differed between the trials, including a 'surgeon's procedural checklist',[5] the World Health Organization (WHO) SSC,[13] and a modification of the WHO SSC which included preoperative imaging consultation with a radiologist and postoperative deep-vein thrombosis (DVT) prophylaxis.[14]
The control groups included either no checklist[5,13] or a preexisting preoperative checklist that included nine of the WHO SSC items and was only administered among the nursing team (as opposed to the entire perioperative team).[14]
Trial follow-up was either in hospital,[5] in hospital censored at 30 days,[14] or 30 days.[13]
Risk of bias within studies
The risk-of-bias table is shown in Fig. 2. The study by Calland et al.[5] was a high-bias study. As a group, none of the studies controlled for allocation concealment, and blinding of participants and personnel was not possible with administration of an SSC. The stepped-wedge cluster randomisation method used in the trial by Haugen et al.[13] introduced selection bias, as the control group always preceded the intervention group. It is likely that there was detection bias in the study by Chaudhary et al.[14] A single study contributing 5 295 of the 6 060 patients to the meta-analysis was adjudicated to have no detection, attrition or reporting biases.[13]

Unfortunately, we were unable to clarify any data queries with the authors from the trial by Chaudhary et al.,[14] so all the data presented here were extracted from the publication only.
Results of individual studies
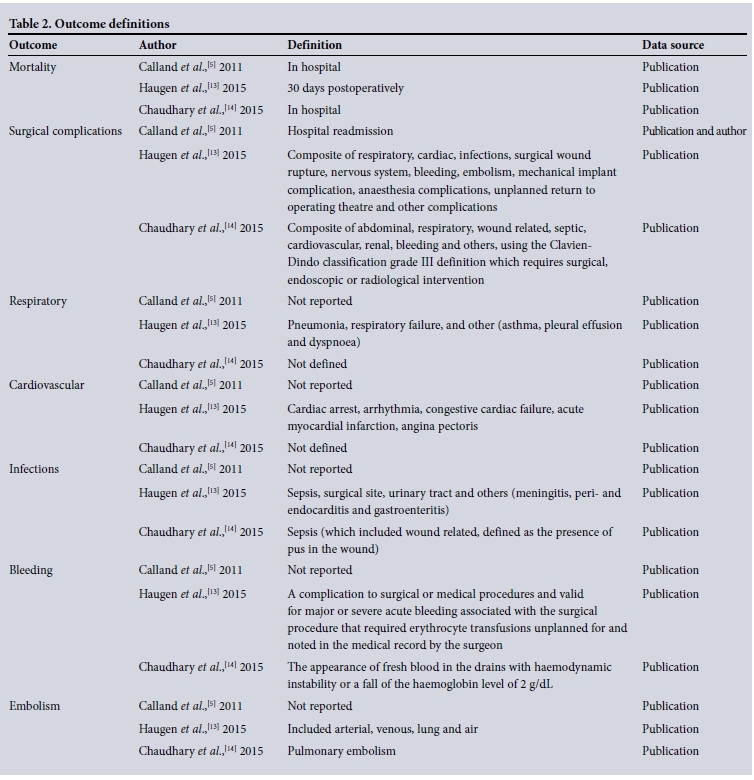
The study outcome definitions are shown in Table 2. The individual study results were mixed. In the small study of laparoscopic cholecystectomies, the surgical checklist did not result in a difference in surgical outcomes (it was not powered for clinically important major adverse outcomes), although there were significantly more safety-related team behaviours.[5] In the large high-income country (Norwegian) study, surgical complications decreased significantly (absolute risk reduction (ARR) 8.4%, 95% CI 6.3 - 10.5), as did mean length of hospital stay (-0.8 days; 95% CI 0.11 - 1.43 days).[13] In-hospital mortality was not significantly decreased.[13] While all the included studies provided data on outcomes in tertiary hospitals, this was the only study that provided data on the efficacy of an SSC in a community-level hospital (1 506 of the 5 295 patients in this study),[13] and the SSC was associated with a significant decrease in mortality in the community hospital subgroup (p=0.02).
In the trial of the efficacy of the SSC in a middle-income country, mortality was decreased in the SSC group, but surgical complications were only significantly reduced for the higher-grade surgical complications group (grades 3 and 4 of the Clavien-Dindo classification),[15] and not across all surgical complication grades. Length of hospital stay was not reduced.[14]
Synthesis of results
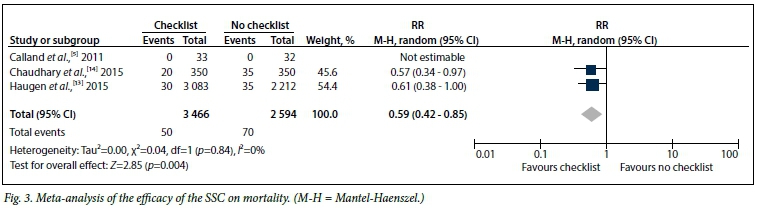
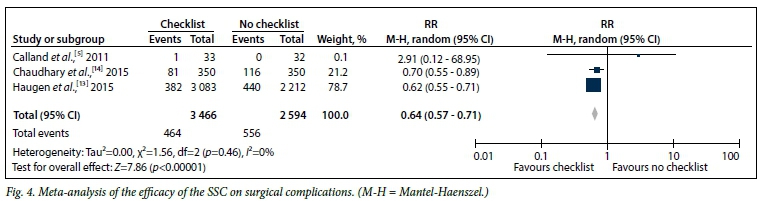
The meta-analyses for mortality and surgical complications are shown in Figs 3 and 4, respectively. For the primary outcome, the SSC was associated with significantly decreased mortality (risk ratio (RR) 0.59, 95% CI 0.42 - 0.85). The secondary outcome of surgical complications was also significantly decreased (odds ratio (OR) 0.64, 95% CI 0.57 - 0.71). There was little heterogeneity for these outcomes (I2=0%), and relative risk reductions between the two large trials were similar despite the large differences in ARR between the two trials.
A meta-analysis of the individual components of the surgical complications, revealed the following associations with the SSC: respiratory complications RR 0.59, 95% CI 0.21 - 1.70, p=0.33; cardiac complications RR 0.74, 95% CI 0.28 - 1.95, p=0.54; infectious complications RR 0.61, 95% CI 0.29 - 1.27, p=0.18; and perioperative bleeding RR 0.36, 95% CI 0.23 - 0.56, p<0.00001.
It was not possible to conduct a meta-analysis for the other prespecified secondary outcomes. Anaesthesia complications were reported in a single trial, with no difference between the groups (p=0.772), although the incidence was low (0.3% in the control group and 0.2% in the SSC group).[13] Length of stay was significantly decreased in one trial[13] and not in another.[14] We could not obtain length-of-stay data from the authors of two of the trials in order to conduct a meta-analysis for length of stay.[5,14] There were no cost analyses presented in any of the included trials.
Risk of bias across studies
There may be attrition bias associated with the definition of surgical complications in the study by Calland et al.[5] (and hence selective reporting), as there was no formal surveillance for hospital readmission for surgical complications (author communication). However, removal of these data from the meta-analysis does not alter the results of the meta-analysis presented in Fig. 4.
Removal of Chaudhary et al.'s[14] data due to detection bias resulted in loss of survival benefit associated with an SSC in the meta-analysis (RR 0.61, 95% CI 0.38 - 1.00; p=0.05), but no change in the significant reduction of surgical complications (RR 0.62, 95% CI 0.55 - 0.71; p<0.00001).
With only three clinical trials, no funnel plot analyses were conducted.
Additional analysis
No additional analyses were conducted.
Discussion
Summary of evidence
This meta-analysis of RCTs showed that the use of an SSC was associated with a significant decrease in short-term mortality and surgical complications in a tertiary and community hospital environment. There was little heterogeneity associated with these findings. Previous meta-analyses of observational cohort studies,[1-4] and now this meta-analysis of RCTs, provide compelling evidence for policy-makers to ensure that SSC becomes mandatory health policy where this situation does not yet exist, and that healthcare providers champion the use of SSCs and ensure that they are implemented correctly and consistently.
This meta-analysis is important because as more countries adopt a national policy mandating SSCs, it becomes difficult to conduct further RCTs. These data suggest that there is sufficient randomised evidence to adopt SSCs in tertiary and community hospital environments. Clinicians should now focus on the correct implementation of SSCs to maximise benefit,[16] especially as compliance is low[1] and complete implementation is associated with better outcomes.[9] Indeed, in the two large studies included in this meta-analysis, it is likely that compliance was overestimated based on the self-reporting of the administering clinicians,[17] and as such, outcomes may even exceed those presented in this meta-analysis.
Study limitations
Study-level limitations may increase bias. Readmission as a marker of surgical complications in the study by Calland et al.[5] may have been associated with attrition bias, as there was no formal monitoring for readmission. The use of a stepped-wedge cluster randomisation process,[13] as routine implementation was mandated by policy, increases selection bias. However, this will inevitably be a limitation of implementing the SSC in any setting. Our priority now should be to sustain the benefit shown by this meta-analysis by focusing on sustained change management. The addition of DVT prophylaxis to the SSC may have added benefit to the checklist group;[14] however, DVT prophylaxis alone would not explain the total benefit associated with the SSC in that trial or in the meta-analysis. Appropriate modifications to the checklist, such as the addition of DVT prophylaxis, are acceptable and may further improve the utility and effectiveness of surgical safety checklists.
The use of the Clavien-Dindo classification[15] to determine surgical complications that at grade 1 level are defined as minor risk events not requiring treatment potentially introduces significant reporting bias, which is important considering the possibility of detection bias in this study.[14] For this reason, we only included the higher-grade Clavien-Dindo complications in the meta-analysis, as they were less likely to suffer from reporting bias.
At the review level, the major limitation of this meta-analysis was the lack of comprehensiveness of the review in answering the question of the efficacy of the SSC in all environments, especially as there are no randomised data from rural-level hospitals. It is therefore impossible to determine the impact of SSCs on outcomes at a rural level. Furthermore, there was detection bias associated with two trials.[5,14] However, removing these trials still suggested a significant reduction in surgical complications warranting implementation of an SSC. Although no subgroup analyses were conducted, the individual trials suggest benefit of implementation of the SSC in middle-and high-income countries, and in tertiary as well as community hospitals. The SSC therefore appears to have wide applicability.
Conclusions
There appears to be sufficient RCT evidence to suggest that SSCs decrease hospital mortality and improve surgical outcomes in both high-income and middle-income countries and in both tertiary and community hospitals. We therefore recommend that no further randomised trials of the efficacy of SSCs be conducted in tertiary and community hospitals. Rather, implementation of SSCs should be considered a global priority at the tertiary and community hospital level, and further research should focus on the ideal components of an SSC, and strategies to ensure successful implementation.[8] Implementation of the SSC at rural hospital level would be encouraged despite a lack of randomised evidence, although a stepped-wedge approach would be recommended to ensure adequate documentation of benefit.
Funding. This article was funded by the departmental resources of the Perioperative Research Group, Discipline of Anaesthesiology and Critical Care, School of Clinical Medicine, University of KwaZulu-Natal, South Africa. There was no external funding for this research.
Authors' contributors. BMB was responsible for the conception or design of the work. All authors were participants in a meta-analysis workshop where they all made a substantial contribution to the acquisition, analysis or interpretation of data for the work, revising the work critically for important intellectual content, and final approval of the version to be published. Also, they are in agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. The first draft of the article was written by BMB. The article was redrafted by BMB following critical review by all authors.
Acknowledgements. We thank Dr J F Calland for clarification of data questions from his trial.
References
1. Borchard A, Schwappach DL, Barbir A, Bezzola P. A systematic review of the effectiveness, compliance, and critical factors for implementation of safety checklists in surgery. Ann Surg 2012;256(6):925-933. DOI:10.1097/SLA.0b013e3182682f27 [ Links ]
2. Lyons VE, Popejoy LL. Meta-analysis of surgical safety checklist effects on teamwork, communication, morbidity, mortality, and safety. West J Nurs Res 2014;36(2):245-261. DOI:10.1177/0193945913505782 [ Links ]
3. Gillespie BM, Chaboyer W, Thalib L, John M, Fairweather N, Slater K. Effect of using a safety checklist on patient complications after surgery: A systematic review and meta-analysis. Anesthesiology 2014;120(6):1380-1389. DOI:10.1097/ALN.0000000000000232 [ Links ]
4. Bergs J, Hellings J, Cleemput I, et al. Systematic review and meta-analysis of the effect of the World Health Organization surgical safety checklist on postoperative complications. Br J Surg 2014;101(3):150-158. DOI:10.1002/bjs.9381 [ Links ]
5. Calland JF, Turrentine FE, Guerlain S, et al. The surgical safety checklist: Lessons learned during implementation. Am Surg 2011;77(9):1131-1137. [ Links ]
6. Pickering SP, Robertson ER, Griffin D, et al. Compliance and use of the World Health Organization checklist in U.K. operating theatres. Br J Surg 2013;100(12):1664-1670. DOI:10.1002/bjs.9305 [ Links ]
7. Treadwell JR, Lucas S, Tsou AY. Surgical checklists: A systematic review of impacts and implementation. BMJ Qual Saf 2014;23(4):299-318. DOI:10.1136/bmjqs-2012-001797 [ Links ]
8. Aveling EL, McCulloch P, Dixon-Woods M. A qualitative study comparing experiences of the surgical safety checklist in hospitals in high-income and low-income countries. BMJ Open 2013;3(8):e003039. DOI:10.1136/bmjopen-2013-003039 [ Links ]
9. Mayer EK, Sevdalis N, Rout S, et al. Surgical Checklist Implementation Project: The impact ofvariable WHO checklist compliance on risk-adjusted clinical outcomes after national implementation: A longitudinal study. Ann Surg 2015:263(1):58-63. DOI:10.1097/SLA.0000000000001185 [ Links ]
10. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA statement. BMJ 2009;339:b2535. DOI:10.1136/bmj.b2535 [ Links ]
11. Cochrane Collaboration. Cochrane Handbook for Systematic Reviews of Interventions. Chapter 8: Assessing risk of bias in included studies. http://handbook.cochrane.org/chapter_8/8_assessing_risk_of_bias_in_included_studies.html (accessed 8 March 2016). [ Links ]
12. GraphPad Software. http://www.http://graphpad.com/quickcalcs/ (accessed 8 March 2016). [ Links ]
13. Haugen AS, Softeland E, Almeland SK, et al. Effect of the World Health Organization Checklist on Patient Outcomes: A stepped wedge cluster randomized controlled trial. Ann Surg 2015:261(5):821- 828. DOI:10.1097/SLA.0000000000000716 [ Links ]
14. Chaudhary N, Varma V, Kapoor S, Mehta N, Kumaran V, Nundy S. Implementation of a surgical safety checklist and postoperative outcomes: A prospective randomized controlled study. J Gastrointest Surg 2015:19(5):935-942. DOI:10.1007/s11605-015-2772-9 [ Links ]
15. Dindo D, Demartines N, Clavien PA. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 2004;240(2):205-213. DOI:10.1097/01.sla.0000133083.54934.ae [ Links ]
16. Russ SJ, Sevdalis N, Moorthy K, et al. A qualitative evaluation of the barriers and facilitators toward implementation of the WHO surgical safety checklist across hospitals in England: Lessons from the 'Surgical Checklist Implementation Project'. Ann Surg 2015;261(1):81-91. DOI:10.1097/SLA.0000000000000793 [ Links ]
17. Levy SM, Senter CE, Hawkins RB, et al. Implementing a surgical checklist: More than checking a box. Surgery 2012;152(3):331-336. DOI:10.1016/j.surg.2012.05.034 [ Links ]
 Correspondence:
Correspondence:
B M Biccard
bruce.biccard@uct.ac.za
Accepted 29 March 2016.



{kind=link}
{kind=link}
{kind=link}
{kind=link}