










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSAMJ: South African Medical Journal
versão On-line ISSN 2078-5135
versão impressa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.106 no.5 Pretoria Mai. 2016
http://dx.doi.org/10.7196/samj.2016.v106i5.10821
REVIEW
Maternal deaths from bleeding associated with caesarean delivery: A national emergency (A review)
S FawcusI; R C PattinsonII; J MoodleyIII; N F MoranIV, V; M G SchoonVI; R E MhlangaVII; S BaloyiVIII; E BekkerIX; G S GebhardtX; National Committee on Confidential Enquiries into Maternal Deaths
IMB BCh, FRCOG. Department of Obstetrics and Gynaecology, Faculty of Health Sciences, University of Cape Town, South Africa, and Deputy Chairperson, National Committee on Confidential Enquiries into Maternal Deaths, South Africa
IIBSc, MB BCh, FRCOG, MD, FCOG (SA), MMed (O&G) ; South African Medical Research Council Maternal and Infant Health Care Strategies Unit and Department of Obstetrics and Gynaecology, Faculty of Health Sciences, University of Pretoria, South Africa
IIIMB ChB, FCOG, FRCOG, MD; Department of Obstetrics and Gynaecology, School of Clinical Medicine, College of Health Sciences, Nelson R Mandela School of Medicine, University of KwaZulu-Natal, Durban, South Africa
IVMB BCh, MA, FCOG Department of Obstetrics and Gynaecology, School of Clinical Medicine, College of Health Sciences, Nelson R Mandela School of Medicine, University of KwaZulu-Natal, Durban, South Africa
VMB BCh, MA, FCOG Department of Health, KwaZulu-Natal, South Africa
VIMMed (O&G), PhD; Department of Health, Free State, South Africa
VIIMB ChB, DMCH, FCOG (SA), MPH; Department of Health, Mpumalanga, South Africa
VIIIMB ChB, CML (Law), CRIA (Theology), Dip Obst, FMAS, Dip MAS, PG Dip Fam Med, MMed (O et G), FCOG (SA); Department of Health, Limpopo, South Africa
IXBSocSc (Nursing), Dip Nursing Education, MSocSc (Advanced Midwifery and Neonatology);School of Nursing, Faculty of Health Sciences, University of the Free State, Bloemfontein, South Africa, and Society of Midwives of South Africa
XMB ChB, MSc (Med Sci), MMed (O&G), FCOG (SA)Department of Obstetrics and Gynaecology, Faculty of Medicine and Health Sciences, Stellenbosch University and Tygerberg Hospital, Tygerberg, Cape Town, South Africa
ABSTRACT
Maternal deaths associated with caesarean deliveries (CDs) have been increasing in South Africa over the past decade. The objective of this report is to bring national attention to this increasing epidemic of maternal deaths due to bleeding associated with CD in the majority of provinces of the country. Individual chart reviews of women who died from bleeding at or after CD show that 71% had avoidable factors. Among the steps we can take are to improve surgical skills and experience, especially in rural hospitals; to improve clinical observations in the immediate postoperative period and in the postnatal wards; and to ensure that appropriate oxytocic agents are given to prevent postpartum haemorrhage. CEOs and medical managers of health facilities, district clinical specialists, heads of obstetrics and gynaecology, and midwifery training institutions must show leadership and accountability in providing an appropriate environment to ensure that women who require CD receive the procedure for the correct indications and in a safe manner to minimise risks.
As early as 2011, the National Committee on Confidential Enquiries into Maternal Deaths (NCCEMD) highlighted the concern of haemorrhage associated with caesarean delivery (CD) in an article published in the SAMJ entitled 'Haemorrhage associated with caesarean section in South Africa - be aware'.[1]
This article drew attention to the findings of the fourth triennial Saving Mothers report for 2005 - 2007,[2] which showed that bleeding associated with caesarean delivery (BLDACD) was the most common causal subcategory of haemorrhage-related maternal death, unlike the pattern in other countries. It also showed that these deaths were increasing over time and were mainly occurring at district and regional hospitals, where most of the CDs were performed. Of most concern, 85% were 'clearly avoidable. Multiple instances of health system failure and substandard care were identified as contributing to these preventable deaths from BLDACD. Practical algorithms for the clinical management of haemorrhage at and after CD were presented. The article exhorted the medical and obstetric community to pay attention to this serious problem.
Since 2010, there have been several publications and interventions directed to this problem:
• The next two triennial reports (2008 - 2010[3] and 2011 - 2013[4]) of the NCCEMD showed further increases in the problem of deaths from BLDACD and described associated avoidable factors.
• Since 2008, the Essential Steps in Managing Obstetric Emergencies (ESMOE) training programme[5] has taught practical modules on managing bleeding at CD. This was recently updated with the inclusion of training videos on the surgical management of postpartum haemorrhage (PPH).
• Two monographs (guideline pocketbooks) were produced by the NCCEMD on: (i) the management of PPH (2010), with algorithms for its prevention and management;[6] and (ii)caesarean section (CS) (2013), aimed at promoting safer CD.[7]
• A PPH training programme, including a lecture, accompanied dissemination of the PPH monograph throughout the country in 2011.
• A CME publication on this problem by the NCCEMD appeared in 2012.[8]
• A DVD lecture on PPH was developed by the Health Systems Trust in 2014 and circulated to district clinical specialist teams to use for teaching in all health districts.[9]
• Publications on maternal mortality and CD in SA[10] and controversies around the use of uterotonics at CD in SA[11] appeared in the SAMJ in 2015.
• Obstetrics & Gynaecology Forum published a special edition with all the articles on the theme of safe CD, including an NCCEMD statement on setting minimum standards for safe CD.[12]
However, despite the above attempts to raise awareness of the problem, the distribution of training materials and the training programmes, the situation has deteriorated. This is in the context of an overall 12.6% reduction in the institutional maternal mortality rate (MMR) in SA in 2011 - 2013 compared with 2008 - 2010, mostly due to a marked reduction in HIV-related mortality, as shown in the sixth triennial Saving Mothers report.[4]
Trends in maternal mortality due to BLDACD in SA
The sixth Saving Mothers report on maternal deaths in SA for 2011 -2013 identified 221 deaths due to BLDACD.[4] Fig. 1 shows that this is an increase from 180 during 2008 - 2010, 141 in 2005 - 2007 and 78 in 2002 - 2004. In the two earlier triennia (2002 - 2004 and 2005 - 2007) these numbers may be overestimates, since for those two reports BLDACD deaths were included in a category of 'uterine trauma' that included cervical and vaginal trauma in addition to BLDACD. The overall increase in numbers of BLDACD deaths may therefore be even greater. The majority of these deaths (98%) were in the public sector.
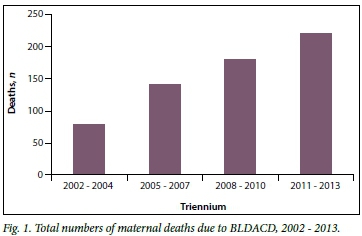
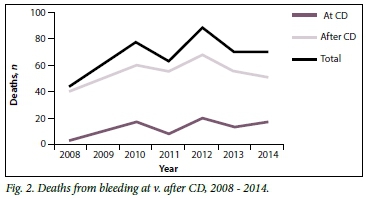
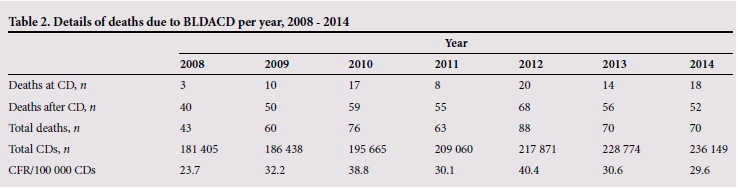
Fig. 2 gives a yearly breakdown of deaths due to BLDACD from 2008 to 2014 and divides them into those specified to be due to bleeding at CD and to bleeding after CD.
These numbers of deaths due to BLDACD over the years obviously need to be viewed in the context of total numbers of CDs performed in SA over the same period (Tables 1 and 2).
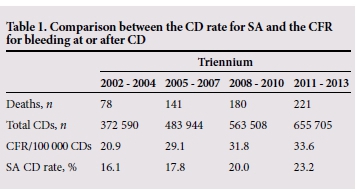
Total numbers of CDs in the public sector (according to District Health Information System statistics) have shown a steady increase from 372 590 (2002 - 2004) to 655 705 (2011 - 2013). This corresponds to an increase in the CD rate (CDR) from 16.1% to 23.2% between 2002 and 2013. In a recent publication, based on a review of country trends in maternal/newborn mortality rates and CDRs,[13] the World Health Organization (WHO) stated that CDRs above 10 - 15% did not confer benefit in terms of reduction in mortality.[14] However, in the same publication the WHO stated that 'every effort should be made to provide caesarean sections to women in need, rather than striving to achieve a specific rate' and 'Caesarean sections should ideally only be undertaken when medically necessary'. The publication also cited the problem of CD-associated complications. This was quantified in the results of an earlier WHO global survey on maternal and perinatal health which showed that maternal mortality after CD without medical indications is three times higher than after vaginal delivery.[15]
If consideration is given to the role of CD in reducing maternal and newborn morbidity (as well as mortality), population CD rates approaching 20 - 25% may be acceptable. The CDR in the private sector in SA is >67%, a level far above that which is necessary to reduce morbidity and mortality.[4]
Although numbers of CDs and the CDR have increased in SA, the increase in BLDACD deaths is not merely explained by the increase in the CDR. Table 1 shows that there has been an increase in the case fatality rate (CFR) for CD (maternal deaths from BLDACD x 100 000/total number of CDs performed) from 20.9/100 000 CDs in 2002 - 2004 to 33.6/100 000 in 2011 - 2013.
The CFR for CD increased by one-third between 2002 and 2013. This is a finding of major concern, showing that the risk of dying from BLDACD has shown a real increase in SA.
This serious finding is illustrated graphically in Fig. 3.
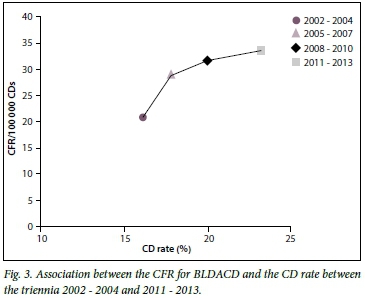
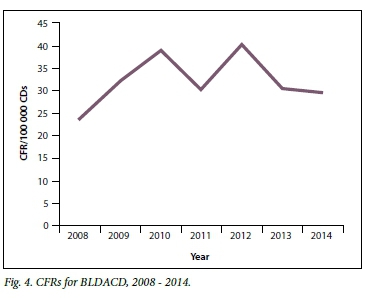
Table 2 sets out annual trends of deaths due to BLDACD and CFRs for CDs since 2008. These data come from the two most recent triennial reports[3,4] and the interim report for 2014.[16] It is possible that both indices have stabilised, and that they may have fallen from 2013, but the numbers and rates are still above acceptable levels. Fig. 4 shows CFRs graphically by year from 2008 to 2014.
The sixth Saving Mothers report for 2011 - 2013[4] showed that CFRs for CD were higher in provinces where CDs were less frequently done. When the CD rate for each province is compared with its CFR from BLDACD, it is quite striking that more mothers died from BLDACD in the provinces where there was a low overall CD rate. The provinces with a CD rate >23% (e.g. Western Cape, KwaZulu-Natal) had a BLDACD CFR of <20, and those with a CD rate of <17% (e.g. Mpumulanga, Limpopo) had CFRs of >30. This could be due to a variety of reasons, including lack of easy access to safe CD in some provinces, and better retention of skills when a reasonable CD rate is maintained.
Why are deaths from BLDACD occurring and increasing?
There are two aspects to this question: (i) what are the causes of the excessive BLDACD that leads to death? and (ii)why are women dying from BLDACD?
What are the causes of the excessive BLDACD that leads to death?
Near-miss audits or monitoring of severe maternal morbidity in SA, although done in a few tertiary centres, is not widespread in SA. This means that accurate statistics on rates of severe morbidity from BLDACD, or the mortality index from this condition, are not available for SA or for different settings and levels of care.
Excessive blood loss at CD is defined as blood loss in excess of 1 000 mL. Routine estimation of blood loss at CD is inaccurate and is done by weighing swabs and measuring blood in suction bottles. However, soaking of theatre/bedlinen and contamination with amniotic fluid makes this inaccurate, and it is well known that blood loss at CD is frequently underestimated. Women who die from BLDACD would be expected to have lost more than 2 500 mL blood. Loss of less blood can be fatal if the woman has severe or moderately severe anaemia at the start of the procedure. With blood loss over 2 000 mL, adjunctive coagulopathy occurs to compound the bleeding problem.
At the pathological level, the causes of excessive bleeding at CD are uterine atony (commonly after prolonged labour), uterine trauma (excessive bleeding from uterine incision or additional tears laterally into the broad ligament or vertically down the lower segment) and placental site bleeding (associated with placenta praevia, previous CD and/or morbidly adherent placenta). A rare but frequently fatal cause of mortality due to BLDACD is amniotic fluid embolus-induced coagulopathy.
The NCCEMD process involves provincial assessors and the specific topic chapter writer analysing all maternal deaths in SA to determine both the cause and avoidable factors. This means that a detailed folder review has been done for all maternal deaths due to BLDACD. The analysis in the sixth Saving Mothers report,[4] also illustrated in Fig. 2 and Table 2 in this article, found that the majority of deaths were reported as due to BLDACD after CD (179 deaths, 81%) as opposed to at CD (42 deaths, 19%).
Unfortunately, in many cases these retrospective folder reviews of deaths could not identify the underlying reason why the woman had BLDACD. The doctor's theatre notes on the CD were frequently of such poor quality that it was not possible to ascertain estimated blood loss, whether the surgeon had found uterine atony, uterine tears or placental site bleeding, what uterotonics were given, whether vaginal bleeding from uterine atony was looked for before wound closure, or the skill of the operator. In many cases the CD was documented as 'uneventful' and had been done very quickly. Nevertheless, it is likely that some pathological event at the operation was responsible for bleeding after the CD, e.g. uterine atony not recognised, uterine angle bleeding not recognised, or bleeding not recognised intraoperatively because of spinal anaesthesia-related hypotension.
However, the folder review identified some concerning factors related to BLDACD:
• In several cases the CD was not indicated (only early decelerations on the cardiotocograph) or actually contraindicated (abruptio placentae with intrauterine death).
• In several cases the CD was done in the second stage of labour because there was insufficient skill to perform assisted vaginal delivery, and in some hospitals assisted deliveries were 'not done'. A second-stage CD is known to have an increased PPH complication rate.
• In several cases the CD was done too late, when labour was obstructed and sepsis had developed.
Why are women dying from BLDACD?
BLDACD is a serious problem, but there are definitive medical and surgical treatments for it, so these women need not die.
Whereas the NCCEMD folder review cannot answer question (i)above very well because of insufficient notes about the CD, it can provide better answers for question (ii), which relates to the quality of management of the BLDACD. The following themes emerged from folder review of deaths due to BLDACD in the sixth Saving Mothers report:[4]
• Seventy-one percent of the deaths were possibly or probably avoidable.
• Use of uterotonics was inadequate and poorly documented. It is essential that oxytocin is given at CD for prevention of PPH, and there are clear national guidelines both for the dosages required for its use in prophylaxis and for therapeutic use of oxytocin and other uterotonic agents such as ergometrine, syntometrine, misoprostol and prostaglandin F2-alpha.[6,7,11] Owing to fear of hypotension caused by large intravenous boluses of oxytocin, the doctors providing the anaesthetics appear to be reluctant to give sufficient uterotonics at CD, and this could have contributed to the increasing mortality from BLDACD. In addition, maintaining an oxytocin infusion for 4 - 6 hours after delivery can ensure sustained uterine contraction. If an intravenous infusion cannot be maintained, intramuscular syntometrine or ergometrine can be given postoperatively, provided there are no contraindications. Research on the use of carbetocin as a long-acting oxytocin is awaited, as is research on the use of prophylactic tranexamic acid for the reduction of blood loss at CD.
• Surgical skills and experience for CD were insufficient, especially in rural district hospitals.
• There was delay in calling for any help in the event of ongoing bleeding (telephonic or consultant on call).
• There was insufficient recourse to additional surgical measures such as uterine compression sutures, and balloon tamponade, which can be therapeutic and obviate the need for hysterectomy; delay in performing hysterectomy where skill was available; and failure to use a uterine tourniquet as a temporising measure during patient transfer.
• There was delay in and insufficient resuscitation, and lack of skill of the doctor providing the anaesthetic.
• Patients were inappropriately discharged from the theatre recovery area while still in hypovolaemic shock.
• Poor monitoring in the postnatal ward resulted in late detection of haemorrhage, or delayed action in response to deteriorating vital signs.
• There was failure to recognise internal post-CD bleeding.
• Doctors at district hospitals were reluctant to reoperate when bleeding was detected after CD, patients instead being transferred to the regional hospital in an unstable condition and dying en route.
• Staffing/supplies issues included emergency blood not available, freeze-dried plasma not stocked, and insufficient staff available for monitoring or to cope with a catastrophic emergency such as massive PPH.
NB: Underlying health system factors related to lack of leadership, lack of clinical governance and inequitable distribution of human resources (doctors/midwives) are likely to be important determinants of the above problems.
Solutions
There is an urgent need for this epidemic of deaths due to BLDACD in SA to be dealt with. These are mostly young women and 'mothers to be' who die from preventable causes.
New global goals are for every country to reduce its MMR by two-thirds by 2030. This means that SA should reduce its MMR from 140 to <50 deaths per 100 000 live births. This will not be achievable unless deaths from BLDACD are reduced.
The solutions are multifactorial and must address the following aspects:
• Health systems issues: ensuring safety of CD in appropriately designated sites according to the document on setting minimum standards for safe CD.[12]
• Ensuring access to surgical or anaesthetic skills through reliable and timeous interfacility transport.[17]
• Ensuring equitable distribution of appropriately skilled staff to all levels of care, districts and provinces.
• Clinical governance and outreach mechanisms to support district doctors and midwives.
• Training and skills development to be ongoing for midwives and doctors with the continuation of regular ESMOE/Emergency Obstetric Simulation Training (EOST). This has resulted in a 30% reduction of deaths from obstetric haemorrhage in eight priority districts.[18]
• Improved training of health professionals in assisted vaginal delivery.
• Surgical skills for CD/complicated CD need to be taught by ESMOE and by 'hands-on' supervision. Surgical competence of junior doctors needs to accredited by a senior doctor before they are allowed to operate independently.[12]
• Adherence to protocols and algorithms.[5,8]
• Monitoring of BLDACD in all facilities conducting CDs needs to be routinely performed, with monthly review of data by senior staff including CEOs and district clinical specialist teams (DCSTs). Charts that monitor trends in BLDACD should be posted on all obstetric theatre noticeboards to ensure a team approach to reducing it and to ensure accountability. (This also requires improved documentation of surgical details at CD.)
• Obstetricians in the private sector to be requested to assist the public sector, performing CD lists and assisting with CD skills training.
Description of a maternal death from bleeding associated with CD at a district hospital
• Emergency CD in para 1 for cephalopelvic disproprtion. No documentation of prophylactic oxytocin.
• PPH in recovery, sent to postnatal ward (PNW) despite low blood pressure and tachycardia. PPH in PNW. Low BP and tachycardia >120/min continued.
• Well monitored but no response by nurse to signs of shock.
• After 2 hours, doctor was called and gave telephonic advice to give oxytocin 20 IU as an intravenous bolus and 30 IU as an infusion.
• Doctor called again when no improvement, and came to see patient. Decided to refer rather than do relaparotomy.
• Patient died in lift on way to ambulance.
Comment
Oxytocin prophylaxis should always be given at CD. The patient should not have been allowed to leave the recovery area with signs of hypovolaemic shock. Despite good monitoring there was a delayed response by the nurse in calling the doctor. The doctor did not assess the patient, and telephonically prescribed an incorrect dose of oxytocin. On subsequent assessment, the doctor decided to refer the patient without performing any definitive treatment.
Immediate administration of further uterotonics and a relook laparotomy should have been done before the patient left the recovery area.
These same recommendations have been listed before in previous publications and guidelines.[1-11] Now is the time for more focused implementation, leadership and accountability. Involvement of CEOs, DCSTs, heads of obstetrics and gynaecology and midwifery at training institutions, and clinical managers is essential for this.
The paradox in SA is that there is an over 67% CD rate in private facilities. These procedures, many without medical indications, are done in well-resourced facilities by skilled surgeons, whereas in the public sector the CD rate is 23%, the majority of CSs are performed for medical indications only, and most are done in district hospitals with limited human resources, skills and other essential resources.
This paradox in our health system today is well illustrated by a comment by Julian Tudor-Hart in 1971[19] suggesting the 'inverse care law' for healthcare provision: 'The inverse care law is the principle that the availability of good medical or social care tends to vary inversely with the need of the population served.'
Urgent activities needed to reduce deaths from bleeding at CD
• Prevention. Ensure that CDs are only done for appropriate indications. Indications for CD should be discussed at district meetings or with senior doctors, and audited using Robson's classification as recommended in the WHO Statement on Caesarean Section.[14]Improve skills of doctors and midwives in assisted vaginal delivery.
• Early recognition. Ensure routine post-CD monitoring with early warning charts, and immediate assessment when BLDACD is suspected.
• Immediate resuscitation. Implement algorithms for resuscitation, and ensure availability of fluids, giving sets, blood and freeze-dried plasma.
• Immediate medical and surgical treatment to stop the bleeding.
Ensure that skills are available, display PPH posters, follow protocols, strengthen teamwork and perform EOST drills.
• Emergency transport. Ensure that on-site transport for interfacility transfer is available from level 1 after applying temporary measures to deal with the BLDACD.
• Leadership. CEOs and clinical managers to take responsibility for the above activities by ensuring accountability, supplies and staffing, functioning referral systems, regular auditing of BLDACD, and compliance with protocols.
To achieve the above, facilities and provinces need to prioritise maternal care and step up their governance and accountability processes and prioritise to ensure CD safety.
Suggested key actions to be implemented immediately
• All hospitals conducting CDs must ensure that they comply with the minimum standards for safe CD in SA. Hospitals that currently do not comply must be supported by their provincial health departments to make the necessary changes to ensure compliance as a matter of urgency.
• All hospitals conducting CDs must have on-site ESMOE trainers, who run a regular programme of ESMOE training for all doctors at the hospital involved in CDs (this includes sessional doctors and midwives working in the maternity section). The ESMOE training must cover the management of obstetric haemorrhage and surgical skills, incorporating EOST (emergency drills) training
• District clinical specialist teams and specialists at regional or tertiary centres should prioritise training in CD technique (through direct supervision in theatre) for medical officers, registrars and interns, ensuring that it is a regular key activity in their monthly schedule.
• Every facility performing CD must monitor and audit BLDACD by recording the numbers of women who bleed more than 1 000 mL at CD and/or require additional surgical measures/ blood transfusion after CD. Findings to be discussed at facility maternal mortality and morbidity meetings.
Caesarean sections were introduced in obstetrics to save lives, not to cause additional mortality. They need to be done for appropriate indications and safely for all women, including those who are poor.
Women's lives matter!
References
1. Fawcus S, Moodley J, for the National Committee on Confidential Enquiries into Maternal Deaths. Haemorrhage associated with caesarean section in South Africa - be aware. S Afr Med J 2011;101(5):306-309. [ Links ]
2. Pattinson RC, ed. Saving Mothers: Fourth Report on Confidential Enquiries into Maternal Deaths in South Africa, 2005-2007. Pretoria: National Department of Health, 2010. [ Links ]
3. Pattinson RC, ed. Saving Mothers: Fifth report on Confidential Enquiries into Maternal Deaths in South Africa 2008-2010. Pretoria: National Department of Health, 2012. [ Links ]
4. Pattinson RC, ed. Saving Mothers 2011-2013: The Sixth Report of the National Committee for Confidential Enquiries into Maternal Deaths in South Africa. Pretoria: Government Printer, 2014. [ Links ]
5. Pattinson RC, ed. Essential Steps in Managing Obstetric Emergencies (ESMOE) training policy. January 2009. www.ESMOE.co.za (accessed 8 April 2016). [ Links ]
6. National Committee on Confidential Enquiries into Maternal Deaths. A Monograph of the Management of Postpartum Haemorrhage. Pretoria: National Department of Health, 2010. [ Links ]
7. National Committee on Confidential Enquiries into Maternal Deaths. A Monograph on Caesarean Section. Pretoria: National Department of Health, 2013. [ Links ]
8. Fawcus S, Moodley J, for the National Committee on Confidential Enquiries into Maternal Deaths. Prevention and management of blood loss at caesarean section. CME 2012;30(4):138-142. [ Links ]
9. Health Systems Trust. Management of postpartum haemorrhage training videos, Part I and Part II, 2014. http://www.hst.org.za/projects/reducing-maternal-and-child-mortality-through-strengthening-primary-healthcare-rmch (accessed 22 March 2016). [ Links ]
10. Gebhardt GS, Fawcus S, Moodley J, Farina Z. Maternal death and caesarean section in South Africa: Results from the 2011 - 2013 Saving Mothers Report of the National Committee for Confidential Enquiries into Maternal Deaths. S Afr Med J 2015;105(4):287-291. DOI:10.7196/SAMJ.9531 [ Links ]
11. Farina Z, Fawcus S. Management of obstetric haemorrhage. Oxytocin ensuring appropriate use and balancing efficacy with safety. S Afr Med J 2015;105(4):271-274. DOI:10.7196/SAMJ.9179 [ Links ]
12. Moran N, for the NCCEMD. Setting minimum standards for caesarean delivery in South Africa. Obstetrics & Gynaecology Forum 2015;25(3):41-44. [ Links ]
13. Ye J, Betran AP, Velo MG, Souza JP, Zhang J. Searching for the optimal rate of medically necessary caesarean delivery. Birth 2014;41(3):237-244. DOI:10.1186%2Fs12978-015-0043-6 [ Links ]
14. World Health Organization. WHO Statement on Caesarean Section: Executive Summary. Geneva: WHO, 2015. http://www.who.int/reproductivehealth/publications/maternal_perinatal_health/cs-statement/en/ (accessed 22 March 2016). [ Links ]
15. Souza JP, Gulmezoglu AM, Lumbiganon P, et al., for the WHO Global Survey on Maternal and Perinatal Health Research Group. Caesarean section without medical indication is associated with an increased risk of adverse short-term maternal outcomes: The 2004-2008 WHO Global Survey on Maternal and Perinatal Health. BMC Med 2010;8:71. [ Links ]
16. National Committee on Confidential Enquiries into Maternal Deaths. Saving Mothers, 2014: Interim Report. Pretoria: Department of Health, 2014. [ Links ]
17. Schoon MG. Impact of inter-facility transport on maternal mortality in the Free State Province. S Afr Med J 2013;103(8):534-537. DOI:10.7196/SAMJ.6828 [ Links ]
18. Pattinson RC. ESMOE-EOST scale up programme: Interim report on impact. Presented at the 35th Priorities in Perinatal Care Conference, Bela Bela, South Africa, 8 - 11 March 2016. [ Links ]
19. Tudor-Hart J. The inverse care law. Lancet 1971;297(7696):405-412. DOI:10.1016/S0140-6736(71)92410-X [ Links ]
 Correspondence:
Correspondence:
J Moodley
jmog@ukzn.ac.za
Accepted 31 March 2016.


{kind=link}