










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSAMJ: South African Medical Journal
versão On-line ISSN 2078-5135
versão impressa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.106 no.3 Pretoria Mar. 2016
http://dx.doi.org/10.7196/samj.2016.v106i3.10278
IN PRACTICE
HEALTHCARE DELIVERY
The value of internal medicine outreach in rural KwaZulu-Natal, South Africa
R I CaldwellI; B GaedeII; C AldousIII
IBSc(Med), MB ChB, FCP (SA), FRCP (Lond); Spent more than 25 years in private practice as a specialist physician in Pietermaritzburg, South Africa, and then took up a post at Grey's Hospital as outreach physician for internal medicine. The outreach contract has come to an end, but he has a part-time position with the School of Clinical Medicine, University of KwaZulu-Natal (UKZN), as undergraduate liaison between Pietermaritzburg and Durban
IIMB BCh, MMed (Fam Med), PhD;Was recently appointed Head of the Department of Family Medicine at UKZN. Prior to this he was Director of the Centre for Rural Health at UKZN for 4 years after working for more than a decade at Emmaus Hospital in the Drakensberg. His areas of interest and research have included the healthcare system, community-level care (including home-based care and traditional medicine), human rights and medical anthropology. Recent interests include education of health professionals and establishment of a decentralised teaching platform
IIIPhD; Academic Leader for Research at the School of Clinical Medicine at UKZN. She is a medical scientist with a PhD in science education and is involved in postgraduate research mentorship across several medical disciplines including surgery, orthopaedics, dermatology, paediatrics, ophthalmology, general medicine and psychology. Her own research interest is human genetics
ABSTRACT
BACKGROUND: Sustainable multifaceted outreach is crucial when equity between specialist services available to different sections of South Africa (SA)'s population is addressed. The healthcare disadvantage for rural compared with urban populations is exemplified in KwaZulu-Natal (KZN). Outreach to rural hospitals has reduced the need for patients to undergo journeys to regional or tertiary hospitals for specialist care.
OBJECTIVES: Multifaceted outreach visits to seven district hospitals in western KZN by a specialist in the Pietermaritzburg Department of Internal Medicine were analysed for the period 2013 - 2014.
METHODS: Church of Scotland, Vryheid, Dundee, Charles Johnson Memorial, Rietvlei, Estcourt and Greytown hospitals were visited. During each visit, data were collected on data collection forms, including patient numbers, gender and age, whether out- or inpatient, whether referred, and diagnostic categories.
RESULTS: During 113 visits, of 1 377 contacts made, 631 were outpatients and 746 were inpatients. Females formed the majority overall, but for inpatients males outnumbered females. The majority of patients were aged >40 years, but over half of inpatients seen were aged <40 years. A modest 15% of patients seen were referred to hospitals with specialist services. Overall, cardiovascular disease, predominantly among outpatients, was the biggest diagnostic category. Infectious diseases followed, primarily among inpatients, and then general medicine. No other category reached 10%.
CONCLUSIONS: The analysis showed differences between diagnostic categories, especially when outpatients and inpatients were separated out. Referral patterns, age-distribution and gender distinctions were made. The value of a good database was confirmed. The multifaceted outreach may have suggested useful outcomes as well as output. The vulnerability v. sustainability of outreach programmes was emphasised.
Sustainable multifaceted outreach is a necessity if access to specialist services for different sections of the population in South Africa is to be addressed. The disadvantage in terms of healthcare for rural compared with urban populations is starkly exemplified in KwaZulu-Natal (KZN).
Outreach programmes are a means of increasing access to specialist care by rural populations, who are in many cases impoverished and therefore unable to reach centralised services provided in cities.[1-3] The World Health Organization defines outreach as '... any type of health service that mobilises health workers to provide services to the population or to other health workers, away from the location where they usually work and live'.[4] In southern African terms, specialist outreach to rural hospitals has reduced the need for patients in distant and disadvantaged areas and communities to undergo demanding journeys to regional or tertiary hospitals in order to obtain standard specialist care.[5-7]
It is suggested that although simple outreach (specialist outpatient (OP) clinics that are merely displaced from the central to a peripheral hospital) can increase output in terms of patient care, multifaceted outreach is required in order to improve overall outcomes by including inservice training for doctors permanently stationed in rural areas.[1,6,7] Multifaceted outreach may be defined as including two or more discrete interventions, such as liaison with medical staff, 'problem' ward rounds, formal teaching and seminars and patient contact sessions.[8]
An important aspect of outreach is the perceived skills mix of the visiting consultant and the relationship built up with the relevant doctors at the receiving hospital. There needs to be a match, where the visiting hospitals feel they get the most support and value and where the visiting consultant gives the most input. The tension between being locally responsive and standardising the input is evident in the differences in the patterns of patients seen, as presented in this review. The success of this aspect may be difficult to quantify.
The Pietermaritzburg (PMB) Department of Internal Medicine outreach programme has documented outreach over the past 7.5 years (2007 - mid-2014), recording 680 hospital visits, 7 259 patient contacts and 4 497 personnel contacts.[7] The outreach was multifaceted in that it included problem ward rounds, OP clinics requiring the presence of the resident doctors, and formal teaching sessions.
The current study made use of a standard data collection form, recording gender and age details of patients, whether they were out- or inpatients (IPs) and whether or not they were referred. The patients were also categorised into broad diagnostic or subspecialty groups based on the 11 existing subspecialties in the PMB Department of Internal Medicine.
This analysis considered differences between OP and IP hospital populations when gender, age group, diagnostic category and referral pattern were compared. The chance similarity in the large numbers between the two groups, OP and IP, may have given additional validity to the study. The most important questions to be asked were whether this analysis added useful evidence to research on specialist outreach programmes, and ultimately whether it fulfilled its objective, namely to show the importance of multifaceted outreach and how vital it is to sustain such programmes.
Methods
As part of the ongoing review of the PMB Department of Internal Medicine outreach service, the database of visits to seven hospitals from January 2013 to December 2014 was analysed with regard to frequency of visits to each hospital, patient numbers, gender and age distribution of patients, whether patients were IPs or OPs, referral pattern and the diagnostic categories into which patients fell. These years rendered comprehensive and representative data, and the analysis was carried out by a single specialist, ensuring consistency of data capture.
The data were kept in duplicate at Red Cross Air Mercy Service (AMS)'s Durban base and in the Department of Internal Medicine at Grey's Hospital, PMB. Permission for access to the database had been granted by the AMS. The identity of patients was not disclosed, and ethics approval previously obtained from the University of KwaZulu-Natal was revised and extended.
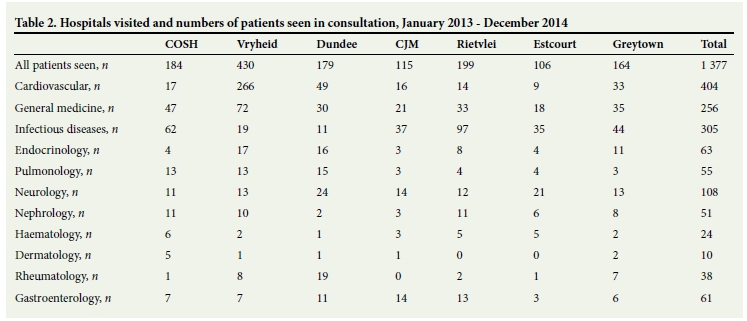
The seven hospitals visited included Church of Scotland Hospital (COSH) in Tugela Ferry, Vryheid Hospital, Dundee Hospital, Charles Johnson Memorial Hospital (CJM) in Nqutu, Rietvlei Hospital near Umzimkulu, Estcourt Hospital and Greytown Hospital. The diagnostic categories were cardiovascular diseases, general medicine, infectious diseases, endocrinology, pulmonology, neurology, nephrology, haema-tology, dermatology, rheumatology and gastroenterology.
Results
In summary, seven hospitals were visited and 113 visits analysed, with an average of 16 visits per hospital (range 13 - 20). A total of 1 377 patients were seen in consultation, of whom 631 were OPs and 746 IPs. In comparing the pattern of the visits it was found that at Vryheid and Dundee hospitals, visits were predominantly for OPs; of the 609 patients seen, all but 45 were OPs. In contrast, at COSH, CJM, Rietvlei and Estcourt hospitals, visits were predominantly for IPs; of 604 patients seen, only one was an OP. Greytown (164 patient contacts) was the only hospital where both IPs (n=98) and OPs (n=66) were regularly seen (Table 1).
Gender and age range of patients seen
Overall, 638 (46%) patients seen were male, and 739 (54%) were female. Females formed the majority in OP-dominated visits: 369/609 (61%) v. males 240/609 (39%), whereas in IP-dominance, males outnumbered females: 330/604 (55%) v. 274/604 (45%).
Overall, 57% of patients seen were >40 years old; this proportion rose to 70% for OP-dominated visits and fell to 44% for IP-dominated visits, where 41% of patients fell into the 25 - 40-year-old group. Over half (57%) of patients seen in IP-dominated hospitals were aged <40 years.
Referrals to regional or tertiary hospitals
A modest proportion of patients seen (204/1 377) were referred to hospitals with specialist services (15%). For OP-dominated hospital visits, 103/609 patients (17%) seen were referred. For IP-dominated visits, 73/604 (12%) were referred. For mixed IP and OP hospital visits (Greytown), 28/164 (17%) were referred (Table 1).
Within categories, 68/404 cardiovascular disease patients seen (17%) were referred, whereas only 4% of both infectious diseases patients (11/305) and general medicine patients (9/256) were referred. With OP dominance, cardiovascular disease referrals were 15%, and higher at 23% for IP-dominated referrals.
Diagnostic categories
Cardiovascular diseases was the biggest diagnostic category, with 404/1 377 (29%) patients. Infectious diseases patients followed with 305/1 377 (22%), then general medicine with 256/1 377 (19%). No other category reached 10% (Table 2).
There was a striking difference between diagnostic categories for OP v. IP dominance. Cardiovascular diseases represented 52% (315/609 patients seen) for the former, with only 9% (56/604) for the latter. In contrast, infectious diseases represented 38% for IP dominance (231/604), and only 5% (30/609) for OP dominance. General medicine provided 17% for OP-dominated and 20% for IP-dominated visits, and again the other diagnostic categories remained below 10% irrespective of OP or IP dominance.
Fig. 1 shows the comparison between the three major diagnostic categories for IPs, OPs and all patients.

Discussion
The outreach service to the hospitals under consideration was multifaceted in that it included interventions such as liaison with medical staff and teaching meetings as well as patient contact. Even on OP-dominated visits, the booked OP session required the presence and participation of medical officers employed at that hospital, and was therefore not simply a specialist OP clinic held in a peripheral hospital. The question is whether such specialist outreach was sustainable and of value to the recipient hospital.
Although female medical wards in KZN district hospitals regularly appear more fully occupied than male wards, gender predominance elsewhere in Africa is variable.[9-11] In this study, where the overall predominance in the wards and OP clinic was female, the opposite was noted for the IP-dominated group. However, this may be an artificial representation depending on the preparedness of a particular ward for the outreach visit. For example, at one of the hospitals (111:73 male/ female), the male medical ward was usually better prepared for the visit, and the male tuberculosis (TB) ward invariably added five or six patients per visit. At another, there were invariably additional patients in the male surgical ward with medical problems that were discussed. The gender pattern was therefore more likely to reflect the referral choice of the on-site doctors rather than the burden of disease or the population distribution in rural areas, for IPs at least.
With regard to age range, the data confirmed that IPs included a large proportion of young patients, <40 years old, with many under 25, because of communicable diseases. In constrast, a booked OP clinic which largely excluded communicable disease reflected the prominence of degenerative diseases and a preponderance of a population aged >40 years. Again, however, the bookings were determined by the local doctors and did not necessarily reflect the population distribution of diseases.
The pattern of referrals illustrated primarily that outreach facilitated the referral of patients to further specialist-level care. Overall, 15% of all patients seen were recommended for such referral. The variation in referral pattern between OP- and IP-dominant or diagnostic groups was small, ranging from 12% to 17%. There was also indication that it was only this minority of patients that was referred, so that the majority continued to be managed at the base hospital, with advice given as to further appropriate treatment.
This was of relevance to cardiology, since there was a preponderance of patients with cardiovascular disease seen, particularly in the OP setting. Only 17% of such patients required subspecialist referral, whereas without the outreach service many more of these patients might have been referred, resulting in overcrowding of the cardiology clinic at the receiving hospital. Therefore, even if only half of the patients seen by the outreach physician had otherwise been referred directly to cardiology, the outreach visit would have saved more than 40% of such referrals. Future studies to assess the outcomes of patients referred for further regional or tertiary care will be important in measuring the contribution of a competent specialist opinion towards overall patient care and health system functioning.
With regard to diagnostic categories, the data collection sheets used on each hospital visit were detailed enough to afford easy categorisation of patients according to subspecialty. The criterion used was to which subspecialty a patient would belong if referral were required. An option might arise where more than one such subspecialty was involved; here, the dominant symptoms might prevail, or such a patient could be categorised into the general medicine group. A subspecialty that may have received slight over-representation was cardiology, where less specific symptoms and signs, such as palpitations and hypertension, could result in allocation to the cardiovascular diseases category.
The results confirmed that there was a different patient population in a booked OP setting compared with those IPs seen as part of a 'problem' ward round. As expected, more than a third of the latter fell into the infectious diseases category, where HIV disease and TB predominated. Many other patients in the ward would also belong to the same category; the outreach physician was only seeing those perceived to be presenting management problems. The booked OP clinics, however, were probably little different from unselected medical OP clinics around the world: the cardiovascular category was highly represented,[12,13] and the infectious diseases category was barely represented - HIV-positive patients belonged to antiretroviral clinics, and HIV-TB management was not regarded as an outreach problem unless the patient was sick enough to be admitted.
The analysis showed the value of comprehensive documentation of each hospital visit, so that in addition to numbers of patient and personnel contacts made, the gender, age and diagnostic category of patients was recorded, as well as whether they were OPs or IPs and whether they were referred. The virtue of retaining such data consistently is appreciated; this enabled the detailed analysis in this study, and has provided a database of activities since 2007, with useful implications for further comparisons and research, including prospective studies. The design of the data collection forms may require modification in the light of this analysis.
The data collected did not quantify the outcomes of changes in behaviour by the recipient doctors or by the visiting consultant in response to the input. While this is an important component of a multifaceted outreach service (beyond offering a specialist service at a different location), it is much harder to measure and requires further investigation.
This study, like other SA studies, has attempted to show that multifaceted outreach may be beneficial for recipient hospitals, their patients and their personnel.[7,14] In KZN, a province that has a transport agreement between its Department of Health and the AMS, such specialist outreach would be at its most productive when conducted by as many disciplines as possible, in all its health areas, as part of routine health systems functioning.
However, outreach programmes are fragile. For example, if the transport contract in KZN were not to be renewed, the service would collapse. Studies have emphasised the need for sustainability of multifaceted outreach programmes in order for them to remain effective in the long term.[15] Regular visits with meticulous data recording and subsequent analysis may be an important contribution to such sustainability.
Conclusion
The study provided interesting comparisons between diagnostic categories, both overall and when OPs and IPs were separated out. Insight was obtained into referral patterns, and age-distribution and gender distinctions were also made. The value of a comprehensive and carefully maintained database was confirmed. As a result of internal medicine outreach, many rural patients received a specialist opinion and referrals were either facilitated or obviated, suggesting useful outcomes for these patients. Further investigations with follow-up on individual patient progress and referrals are required to understand the patient flows and outcomes more comprehensively.[14] The role of multifaceted outreach in increasing the access to specialist healthcare by impoverished rural populations and the ability to sustain such programmes is emphasised.
References
1. Gaede BM McKerrow NH. Outreach programme: Consultant visits to rural hospitals. CME 2011;29(2):57-58. [ Links ]
2. De Roodenbeke E, Lucas S, Rouzaut A, Bana F. Outreach Services as a Strategy to Increase Access to Health Workers in Remote and Rural Areas (Technical Report No. 2). Geneva: World Health Organization and International Hospital Federation, 2011. http://whqlibdoc.who.int/publications/2011/9789241501514_eng.pdf (accessed 3 June 2015). [ Links ]
3. Gruen RL, Bailie RS. Specialist clinics in remote Australian Aboriginal communities: Where rock art meets rocket science. J Health Serv Res Policy 2004;9(Suppl 2):61. [http://di.doi.org/10.1258/1355819042349844] [ Links ]
4. O'Sullivan BG, Joyce CM, McGrail MR. Adoption, implementation and prioritization of specialist outreach policy in Australia: A national perspective. Bull World Health Organ 2014;92(7):512-519. [http://dx.doi.org/10.2471/BLT.13.130385] [ Links ]
5. Schoevers J, Jenkins L. Factors influencing specialist outreach and support services to rural populations in the Eden and Central Karoo districts of the Western Cape. Afr J Prm Health Care Fam Med 2015;7(1):Art. No. 750. [http://dx.doi.org/10.4102/phcfm.v7i1.750] [ Links ]
6. Reid MJA, Kirk BL. Assessing the impact of airborne outreach to build clinical capacity in rural Botswana. J Public Health Africa 2013;(1):55-59. [http://dx.doi.org/10.4081/jphia.2013.e11] [ Links ]
7. Caldwell RI, Gaede BM, Aldous C. Description of an internal medicine outreach consultant appointment in western KwaZulu-Natal, South Africa, 2007 to mid-2014. S Afr Med J 2015;105(5):353-356. [http://dx.doi.org/10.7196/SAMJ.9173] [ Links ]
8. Gruen RL, Weeramanthri TS, Knight SE, Bailie RS. Specialist outreach clinics in primary care and rural hospital setting* Cochrane Database Syst Rev 2004;(1):CD003798. [http://dx.doi.org/10.1002/14651858.CD003798.pub2] [ Links ]
9. Okunola O, Akintunde A, Akinwusi PO. Some emerging issues in medical admission pattern in the tropics. Niger J Clin Pract 2012;15(1):51-54. [http://dx.doi.org/10.4103/1119-3077.94098] [ Links ]
10. Ogun SA, Adelowo OO, Familoni OB, Jaiyesimi AE, Fakoya EA. Pattern and outcome of medical admissions at the Ogun State University Teaching Hospital, Saganu - a three year review. West Afr J Med 2000;19(4):304-308. [ Links ]
11. Ike SO. The pattern of admissions into the medical wards of the University of Nigeria Teaching Hospital, Enugu (2). Niger J Clin Pract 2008;11(3):185-192. [ Links ]
12. Kadiri S. Tackling cardiovascular disease in Africa. BMJ 2005;331(7519):711-712. [http://dx.doi.org/10.1136/bmj.331.7519.711] [ Links ]
13. Mayosi BM, Flisher AJ, Lalloo UG, Sitas F, Tollman SM, Bradshaw D. The burden of non-communicable diseases in South Africa. Lancet 2009;374(9693):934-947. [http://dx.doi.org/10.1016/S0140-6736(09)61087-4] [ Links ]
14. Clarke DL, Aldous C. Surgical outreach in rural South Africa: Are we managing to impart surgical skills? S Afr Med J 2014;104(1):57-60. [http://dx.doi.org/10.7196/SAMJ.7252] [ Links ]
15. Gruen RL, Weeramanthri TS, Bailie RS. Outreach and improved access to specialist services for indigenous people in remote Australia: The requirements for sustainability. J Epidemiol Community Health 2002;56(7):517-521. [http://dx.doi.org/10.1136/jech.56.7.517] [ Links ]
 Correspondence:
Correspondence:
RI Caldwell
ric@caldwells.co.za
Accepted 9 November 2015.


{kind=link}
{kind=link}