










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.106 n.3 Pretoria Mar. 2016
EDITOR'S CHOICE
Cardiovascular disease (CVD) accounts for approximately 30% of deaths worldwide, with 80% of this burden in developing countries. The epidemiological transition occurring in sub-Saharan Africa has had the consequence of economic and social transformation, resulting in dramatic shifts in disease spectrum from communicable diseases and malnutrition to CVD and cancer. South Africa (SA) is faced with the challenge of four colliding epidemics: (i) poor child and maternal health; (ii) high rates of interpersonal violence; (iii) infectious diseases, including HIV/AIDS and tuberculosis; and (iv) non-communicable diseases, including CVD. This outstanding series of articles spread across three issues of SAMJ/CME represents the collaborative effort of primary health/family physicians and cardiologists from around the country. The authors have synthesised and presented the most current, evidence-based and practical approaches to management of common CVDs. This final issue provides an evidence-based and pragmatic approach to acute coronary syndromes and chest pain, and suspected tachyarrhythmias in the emergency room.
Comorbidity of respiratory and cardiovascular diseases among the elderly living close to mine dumps in SA
As SA is a mining country, many of our people live close to mine dumps. In this study,[1] part of a larger project initiated by the Mine Health Safety Council of South Africa, elderly persons living in communities 1 - 2 km (exposed) and >5 km (unexposed) from five preselected mine dumps in Gauteng and North West provinces were surveyed for deleterious health effects. The crushed sand-like refuse material in these dumps is generated during extraction and milling of ground ore during the mining process. The material contains a complex mixture of heavy metals and trace elements such as gold, copper, lead, zinc, arsenic, cadmium and selenium. The major routes of entry upon exposure include contact with skin or eyes, inhalation and ingestion. Exposed communities are often elderly people and children of lower socioeconomic status living in government-funded houses, informal settlements and retirement homes. Elderly people are potentially highly susceptible to the effects of ambient air pollution as a result of normal and pathological ageing.
The results of this study, the first to have investigated the risk factors associated with comorbidity of respiratory and cardiovascular diseases among elderly people in exposed communities, suggest that living in exposed communities, age, smoking habits, occupational exposure to dust/chemical fumes and use of gas for cooking/ heating in the home were significant risk factors for comorbidity of respiratory and cardiovascular diseases.
Validation of the CoaguChek XS international normalised ratio point-of-care analyser
Point-of-care (POC) testing is the fastest growing segment of the diagnostic test repertoire of laboratories in the developed world. Laboratories have become increasingly involved in supporting testing at the bedside in order to improve the turnaround time and cost of healthcare delivery.
Measurement of the international normalised ratio (INR) is essential in the management of patients on long-term warfarin therapy. Warfarin has a narrow therapeutic range, and because it is subject to numerous drug and food interactions, frequent monitoring to maintain the target INR is vital. The target INR is 2.5 (range 2.0 -3.0) for most indications, including venous thromboembolic disease, non-valvular cardiac conditions including atrial fibrillation, left ventricular systolic dysfunction and mural thrombus, and in the first 3 months following anterior myocardial infarction.
Many POC devices are commercially available. The CoaguChek XS device (Roche Diagnostics, Switzerland) is a small bench-top instrument for INR analysis, suitable for use in anticoagulation clinics. This analyser measures the prothrombin time in seconds using an electrochemical method and shows good correlation with laboratory automated coagulation analysers up to INR values of 3.0.
In a study validating the CoaguChek XS INR POC analyser in patients at Charlotte Maxeke Johannesburg Academic Hospital,[2] the authors demonstrated excellent agreement between the CoaguChek XS and laboratory measurement with the STAGO analyser. In SA, the CoaguChek XS POC device could be implemented in peripheral clinics as a screening tool for patients on long-term warfarin therapy in an attempt to lessen the workload of central anticoagulation clinics. However, the capacity and infrastructure of such clinics would need to be assessed prior to installation of CoaguChek XS POC devices.
High prevalence of cardiovascular risk factors in Durban SA Indians
Previous studies have confirmed a high prevalence of cardiovascular risk factors in SA Asian Indians, with the emergence of premature coronary artery disease in young Indian subjects. Earlier epi-demiological studies showed that SA Indians have a high prevalence and incidence of diabetes mellitus. In a study[3] involving 1 378 subjects (1 001 women) whose mean age was 45.5 (standard deviation 13) years, there was a high prevalence of hypertension (47.5%), diabetes (20.1%), total body obesity (raised body mass index) (32.4%) and increased waist circumference (73.1%). In the youngest age group, there was a high prevalence of total body obesity (32.1%), increased waist circumference (31.3%) and insulin resistance (28.2%). Over half of males and 14.6 % of females were current smokers.
The authors conclude that, compared with Asian Indian subjects with similar risk factor exposure in previous studies, the magnitude of change in risk factor prevalence over the past two decades has been of epidemic proportions. The extremely high prevalence of risk factors explains the emergence of premature coronary heart disease in this community and calls for urgent and aggressive intervention measures aimed at diet, physical activity and cessation of smoking at schoolgoing level.
Amendments to the Sexual Offences Act: Implications for doctors and researchers
Bhamjee et al.[4]deal with the provisions in the new Criminal Law (Sexual Offences and Related Matters) Amendment Act concerning consensual underage sex and sexual activity, indicating how the law has changed from the previous position and exploring the impact that this will have for doctors, researchers and other service providers working with adolescents.
These issues came before the Constitutional Court in the Teddy Bear Clinic case when it considered whether consensual, underage sex and sexual activity violated the constitutional rights of children, as reported in the SAMJ in 2014.[5] The Constitutional Court has now concluded that adolescents have a right to engage in healthy sexual behaviour and that such acts are part and parcel of normative development from adolescence to adulthood. The court held further that criminalising consensual sex or sexual activity between adolescents aged 12 - 15 years violated their rights to privacy, bodily integrity and dignity and was also not in the best interests of the affected children.
Focus on genetics
Several genetics articles feature in this issue of SAMJ.
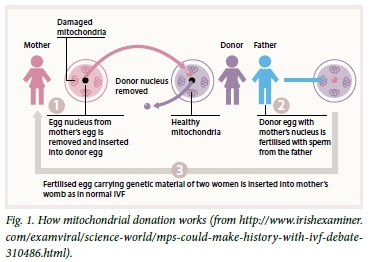
In 'Could we offer mitochondrial donation or similar assisted reproductive technology to South African patients with mitochondrial DNA disease?',[6]SA experts ponder the decision taken by the UK House of Commons last year, which sparked worldwide controversy and debate, to endorse the use of pioneering in vitro fertilisation (IVF) techniques to protect future generations from the risk of mitochondrial DNA (mtDNA) disease, which is known to occur in SA in all population groups. Although individually rare, as a group mitochondrial genetic disorders are thought to be responsible for a substantial proportion of inherited metabolic disease. While the prevalence of mitochondrial genetic disorders is still largely unknown in SA, an estimated prevalence of 1:5 000 - 1:10 000 has been reported in several developed nation populations. However, considering that there are <70 genetically confirmed cases in a country with a population of ~56 million (i.e. 1:900 000 compared with an estimated 1:5 000 worldwide), the authors assert that the number of undiagnosed cases in SA may be staggeringly high.
Adults with mtDNA disease may present with one of the characteristic mtDNA phenotypes such as mitochondrial encephalomyopathy, lactic acidosis and stroke-like episodes, whereas children tend to present early with severe, complex neurological manifestations, hepatopathy, renal tubulopathy, endocrinopathy or cardiomyopathy with rapid progression for which symptoms such as growth failure, deafness, epilepsy and muscle weakness are easily recognisable.
The declining cost of conducting whole-mtDNA sequencing will allow identification of mtDNA mutations and improve SA's capacity for accurate diagnosis and appropriate patient counselling and management, and now that strategies are being put in place to offer a basic but robust service for diagnosis of mtDNA diseases, it is time for this country to initiate a debate on the IVF technique that has been topical in the UK and elsewhere (Fig. 1).
In 'Breast cancer in high-risk Afrikaner families: Is BRCA founder mutation testing sufficient?',[7]Seymour et al. inform us of the presence of three founder mutations in the BRCA genes that occur in the Afrikaner population and lead to hereditary breast and ovarian cancer syndrome (HBOCS). Up to 10% of breast cancer cases are attributable to germline mutations in cancer susceptibility genes, leading to hereditary syndromes. HBOCS is the best described, and is an autosomal dominant inherited syndrome caused by the presence of heterozygous, pathogenic, germline mutations in either the BRCA1 or BRCA2 genes. Patients with a family history of breast and/or ovarian cancer, women <50 years of age with breast cancer, males with breast cancer and families with cancer from high-risk ethnic groups such as Afrikaners and Ashkenazi Jews should be referred for genetic counselling.
Regrettably, in 'Knowledge regarding basic concepts of hereditary cancers, and the available genetic counselling and testing services: A survey of general practitioners in Johannesburg, South Africa' ,[8]Van Wyk and colleagues show that while GPs tend to obtain some information on cancer family history from their patients, this is seldom sufficient to assess the risks. Only one-third of GPs surveyed referred patients to appropriate facilities for assessment and testing; half were aware of genetic testing services, but most were not familiar with the available genetic counselling facilities. Less than half knew about possible paternal inheritance, the low rate of hereditary mutations and their penetrance. Fortunately, the majority of GPs (87%) were interested in learning more about cancer genetics and available services, and they expected to play an increasing role in the field in the future. Appropriate education needs to be increased so that they are better equipped to identify and refer at-risk families.
Zika virus disease
Is SA at risk? The editorial by Jansen van Vuren et al.[9] is compulsory reading.
This will be the last edition of SAMJ that I shall have edited. I wish to thank most sincerely the colleagues who have contributed as authors, reviewers, guest editors and guest editors of CME during my tenure.
Janet Seggie
References
1. Nkosi V, Wichmann J, Voyi K. Comorbidity of respiratory and cardiovascular diseases among the elderly residing close to mine dumps in South Africa: A cross-sectional study. S Afr Med J 2016;106(3):2'0-2'7. [http://dx.doi.org/10.7196/SAMJ.2016.v106i3.10243] [ Links ]
2. Benade EL, Jacobson BF, Louw S, Schapkaitz E. Validation of the CoaguChek XS international normalised ratio point-of-care analyser in patients at Charlotte Maxeke Johannesburg Academic Hospital, South Africa. S Afr Med J 2016;106(3):280-283. [http://dx.doi.org/10.7196/SAMJ.2016.v106i3.9422] [ Links ]
3. Prakaschandra DR, Esterhuizen TM, Motala AA, Gathiram P, Naidoo DP. High prevalence of cardiovascular risk factors in Durban South African Indians: The Phoenix Lifestyle Project. S Afr Med J 2016;106(3):284-289. [http://dx.doi.org/10.7196/SAMJ.2016.v106i3.9837] [ Links ]
4. Bhamjee S, Essack Z, Strode AE. Amendments to the Sexual Offences Act dealing with consensual underage sex: Implications for doctors and researchers. S Afr Med J 2016;106(3):256-259. [http://dx.doi.org/10.7196/SAMJ.2016.v106i3.9877] [ Links ]
5. McQuoid-Mason DJ. The Teddy Bear Clinic Constitutional Court case: Sexual conduct between adolescent consenting children aged under 16 years decriminalised and a moratorium on the reporting duties of doctors and others. S Afr Med J 2014;104(4):275-276. [http://dx.doi.org/10.7196/SAMJ.7653] [ Links ]
6. Meldau S, Riordan G, van der Westhuizen F, et al. Could we offer mitochondrial donation or similar assisted reproductive technology to South African patients with mitochondrial DNA disease? S Afr Med J 2016;106(3):234-236. [http://dx.doi.org/10.7196/SAMJ.2016.v106i3.10170] [ Links ]
7. Seymour HJ, Wainstein T, Macaulay S, Haw T, Krause A. Breast cancer in high-risk Afrikaner families: Is BRCA founder mutation testing sufficient? S Afr Med J 2016;106(3):264-267. [http://dx.doi.org/10.7196/SAMJ.2016.v106i3.10285] [ Links ]
8. Van Wyk C, Wessels T-M, Kromberg JGR, Krause A. Knowledge regarding basic concepts of hereditary cancers, and the available genetic counselling and testing services: A survey of general practitioners in Johannesburg, South Africa. S Afr Med J 2016;106(3):268-271. [http://dx.doi.org/10.7196/SAMJ.2016.v106i3.10162] [ Links ]
9. Jansen van Vuren P, Weyer J, Kemp A, et al. Is South Africa at risk for Zika virus disease? S Afr Med J 2016;106(3):232-233. [http://dx.doi.org/10.7196/SAMJ.2016.v106i3.10615] [ Links ]

