










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSAMJ: South African Medical Journal
versión On-line ISSN 2078-5135
versión impresa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.106 no.2 Pretoria feb. 2016
http://dx.doi.org/10.7196/SAMJ.2016.V106I2.8942
RESEARCH
Mortality in paediatric burns victims: A retrospective review from 2009 to 2012 in a single centre
B JugmohanI; J LovelandII; L DoedensIII; R L MooreIV; A WelthagenV; C J Westgarth-TaylorVI
IMB ChB; Department of Paediatric Surgery, Chris Hani Baragwanath Academic Hospital and Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IIMB ChB, FCS (SA), Cert Paed Surg (SA); Department of Paediatric Surgery, Chris Hani Baragwanath Academic Hospital and Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IIIMB ChB, FC Paed (SA), Cert Crit Care (SA); Department of Paediatric Critical Care, Chris Hani Baragwanath Academic Hospital and Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IVMB ChB, FCS (SA); Department of Paediatric Surgery, Chris Hani Baragwanath Academic Hospital and Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
VDepartment of Paediatric Surgery, Chris Hani Baragwanath Academic Hospital and Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
VIMB ChB, FC Paed Surg (SA); Department of Paediatric Surgery, Chris Hani Baragwanath Academic Hospital and Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
ABSTRACT
BACKGROUND: Childhood mortality is high in low- and middle-income countries. Burns are one of the five leading causes of childhood injury mortality in South Africa (SA). While there is an abundance of literature on burns in the developed world, there are far fewer publications dealing with childhood mortality related to burns in Africa and SA.
OBJECTIVE: To describe the mortality of children admitted to a dedicated paediatric burns unit, and investigate factors contributing to reducing mortality.
METHODS: A retrospective review was performed of patients admitted to the Johnson & Johnson Paediatric Burns Unit, Chris Hani Baragwanath Academic Hospital, Johannesburg, SA, between May 2009 and April 2012.
RESULTS: During the study period, 1 372 patients aged <10 years were admitted to the unit. There were 1 089 admissions to the general ward and 283 admissions to the paediatric burns intensive care unit (PBICU). The overall mortality rate was 7.9% and the rate for children admitted to the PBICU 29.3%; 90.8% of deaths occurred in children aged <5 years. Of children admitted with an inhalational injury, 89.5% died. No child with a burn injury >60% of total body surface area (TBSA) survived.
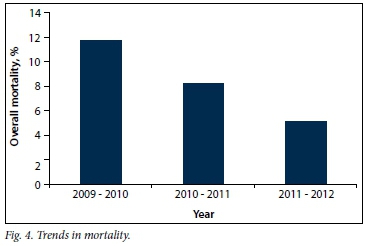
CONCLUSIONS: Our overall mortality rate was 7.9%, and the rate declined significantly over the 3-year study period from 11.7% to 5.1%. Age <5 years, the presence of inhalational injury, burn injury >30% of TBSA and admission to the PBICU were significant risk factors for mortality.
In high-income countries, the mortality rate for children <5 years of age is 1 in 152.[1] In sub-Saharan Africa (SSA) the rate is 1 in 9.[1] In 2011, SSA and Southern Asia shared 83% of global deaths in children <5 years of age.[1] In 2007, the childhood mortality rate was 1 in 21 in South Africa (SA).[2] The 2010 Bulletin of the World Health Organization lists burns as one of the top five causes of fatal urban injuries in SA children.[3] Globally, burn-related deaths account for approximately 100 000 deaths per annum.[4] In SA, approximately 1 300 children die annually as a result of burns.[4]
The Johnson & Johnson Paediatric Burns Unit at Chris Hani Baragwanath Academic Hospital (CHBAH), Johannesburg, SA, opened in 1995. The unit admits approximately 450 patients per year. Before 2009, the unit, including the paediatric burns intensive care unit (PBICU), was run solely by the Department of Paediatric Surgery. For the surgeons managing the unit, burns were just one of several key areas that they were expected to take responsibility for, the others broadly divided into neonatal and general paediatric surgery. Record-keeping before 2009 was imperfect, but there was a perception that the mortality due to burns, particularly those involving a total body surface area (TBSA) of 10 - 20%, was unacceptably high. An internal audit at this point revealed an overall mortality rate approximating 20%, which was deemed unacceptably high, particularly when compared with major burn centres such as the Shriners Hospital for Children in Texas, USA (mortality rate 2.7%) and SB Ankara Diskapi Paediatric Education and Research Hospital in Ankara, Turkey (5.8%).[5,6] This finding prompted negotiations with the paediatric intensive care unit with a view to the intensivists taking over the intensive care management of all patients admitted to the PBICU. This programme in which intensivists became an inclusive part of the multidisciplinary team managing burns patients began in 2009. In addition, a dedicated burns surgeon was employed, and advances in wound care were adopted during the study period. The use of a database enabled improved record keeping.
Objective
To investigate the mortality among children admitted to a dedicated paediatric burns unit at CHBAH.
Methods
After ethical approval had been obtained, the records of patients admitted to the Johnson & Johnson Paediatric Burns Unit, CHBAH, were retrospectively reviewed for May 2009 to April 2012. After excluding elective readmissions for skin grafts and other reconstructive procedures as well as cases with incomplete records, 1 372 patients were included in the study. Age, gender, mechanism of injury and TBSA burned were recorded. The presence of inhalational injury was recorded. Autopsy findings and results were unavailable, and only the suspected cause of death was recorded. Admission to the PBICU, either initially or during the course of the hospital stay, was noted.
The mortality rate for each year was determined. Mortality in the paediatric burns general ward and the PBICU was calculated separately. The overall mortality was then determined. Median ages of children admitted to the general ward and the PBICU and of those who died were calculated. Age groups (years) were categorised as follows: 0 - 1, 1 - 3, 3 - 5 and 5 - 10. The cause of the burn injury was classified as hot water, flame or other, the latter including electrical burns, surface contact burns and various other liquid burns (e.g. tea, coffee and oil). The TBSA burned was determined using a Lund-Browder chart. In this regard, there were often discrepancies between the assessment of the admitting doctor in casualty and the treating team in the unit. The assessment in the unit was taken to be correct, as this was a consensus decision by several staff including surgeons, intensivists and nurses. Simple erythema was not included as part of the TBSA. The TBSA was categorised as follows: 0 - 10%, 11 - 20%, 21 - 30%, 31 - 40%, 41 - 60% and >60%. Specific mortality rates for gender and the subgroups of age and TBSA were also determined for each year of the study period. The Cochran-Armitage test for trends was used to determine the significance of the trends over the 3-year period. The z-test for proportions was used to determine the significance of the difference in mortality between male and female patients admitted to the unit. A statistician assisted with the statistical analysis of the data.
Results
Including all children <10 years of age, 1 372 patients, of whom 754 (55.0%) were male, were admitted to the unit during the study period, 283 having been managed in the PBICU. Table 1 shows the admissions to and deaths in the unit, further subdivided into the general ward and the PBICU, for the 3-year study period. The median age of all patients admitted to the unit was 4.1 years, while the median age of those admitted to the PBICU was 3.0 years. Children aged <5 years comprised 63.0% of the total admissions. The median age of the patients who died was 3.0 years.
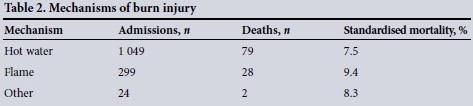
The vast majority of admissions were of children with hot-water burns (n=1 049, 76.5%). Flame burns were the second leading cause of burn injuries (n=299, 21.8%). Electrical burns, contact burns and burns from liquids other than water together accounted for 1.8% of all admissions to the unit. The standardised mortality for the respective mechanisms of injury for the study period is shown in Table 2.
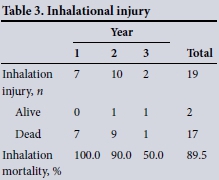
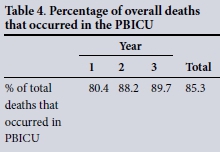
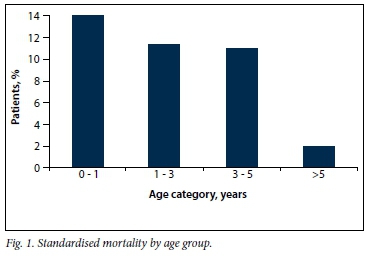
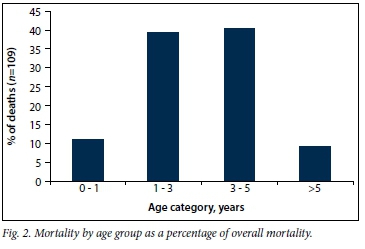
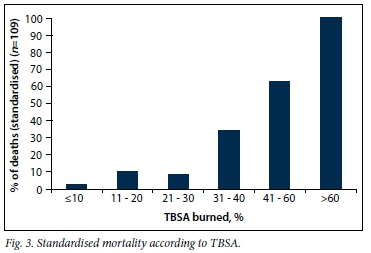
Nineteen patients were admitted with inhalational injury, all to the PBICU. Of these, 17 died (Table 3). There were 109 deaths during the 3-year period, giving an overall mortality rate of 7.9%. Of these deaths, 85.3% occurred in the PBICU (Table 4), the remaining 14.7% occurring in the ward. The majority of deaths occurred in younger children. There was an inverse relationship between age and mortality (Fig. 1). Of the deaths, 50.4% were in children <3 years of age, while 90.8% of deaths were in children <5 years of age (Fig. 2). The standardised mortality according to TBSA is shown in Fig. 3. During the study period, no child with a burn injury >60% TBSA survived. The mortality rates since 2009 are shown in Fig. 4.
Discussion
Reported rates of burn mortality are highest in the first 3 years of life, decreasing and reaching a nadir in adolescence, after which they start to increase again. This concentration of burn injury and mortality among infants and toddlers occurs across SA's population groups. Mortality as well as injury rates are higher in males than in females.[4] This male preponderance is not limited to SA and other low- and middle-income countries (LMICs). A large European systematic review published in 2010 found a 60% male predominance among burn victims aged <16 years.[7] According to the National Injury Mortality Surveillance System, the childhood mortality rate for burns in SA in 2001 was 14.1%, with the majority of deaths occurring in children <6 years of age.[4]
Several decades ago, TBSA burns of >80% were considered uniformly fatal, particularly in the elderly and in very young children. With improvements in resuscitation, intensive care and understanding of the patho-physiology of burns, the mortality has significantly improved. In 1998, the Shriners Institute showed a mortality rate of 33% for massive burns (TBSA >80%) in patients aged 6 months - 17 years. They cited lower age, larger burn size, the presence of inhalation injury, delayed intravenous access, lower admission haematocrit, lower base deficit on admission, higher serum osmolarity at arrival, sepsis, requirement for inotropic support, platelet count <20 x 109/L and ventilator dependency as significant predictors of mortality.[8] In 2001, the same institute showed that children aged <3 years have an increased mortality risk, whether or not they have an additional inhalational burn injury.[9] The hypothesis that very young children are at increased risk was further backed up by a large multicentre study in 2006 that reviewed 12 000 children from 43 burn centres across the USA. The authors concluded that there is strong evidence that, when comparing children based on burn injuries of similar size and aetiology, children aged <4 years are at substantial risk for death compared with their older counterparts.[10]
We compared our overall mortality rate with rates for various institutions around the world (Table 5).

Our overall burn mortality is lower than that in institutions from other LMICs, but higher than that in the SB Ankara Diskapi Paediatric Education and Research Hospital in Turkey, an upper middle-income country, and the Shriners Hospital for Children in the USA, a high-income country. While we believe that this comparison is useful to see where we feature in the global picture, we understand that the various overall mortality rates may be influenced by many factors, including resources and admission criteria.
The majority of our patients had thermal injuries caused by hot water (76.5%). The problems associated with low socioeconomic status, poor living conditions and their correlation with thermal injuries in the SA setting have been well documented.[13] The next most common burns were due to flame injuries (21.8%). Electrical injuries and contact burns made up a very small percentage of our admissions. There was no significant difference in the standardised mortality for the different mechanisms of burn injury (z-test for proportions) (Table 2).
Fifty-five percent of patients admitted during the study period were male. While the mortality in female patients was higher than that in their male counterparts (8.7% v. 7.3%), this difference was not significant (p=0.31; z-test for proportions). This is in contrast to the national population injury mortality in the SA setting, where the mortality rate for male children was found to be significantly higher than that for female children.[4] Inhalational injury was a significant risk factor for mortality, 17 of 19 patients admitted with an inhalational injury having died. Although our overall mortality decreased significantly during the 3-year study period (p=0.0002; Cochran-Armitage test for trend), there was no significant decrease during this time in the trend of mortality of patients who sustained inhalational injuries (p=0.07; Cochran-Armitage test for trend). Another vulnerable subgroup was children aged <5 years. We observed a decreasing trend in mortality with increasing age (Fig. 1), also noted in the literature.[4] Children aged <5 years comprised 63.0% of total admissions and 90.8% of total deaths (Fig. 2). Patients requiring admission to the PBICU have a greatly increased mortality compared with those admitted to the ward (29.3% v. 1.5% chance of dying), with 85.3% of deaths occurring in the PBICU setting. The change in this trend over the 3-year study period was not significant (p=0.24; Cochran-Armitage test for trend). The fact that more severely injured patients are being admitted to the PBICU accounts for the significantly higher mortality in this environment. However, it is concerning that 16 patients (mortality 1.5%) died during their admission to the ward. These deaths were either truly unexpected or the patients were inadequately assessed and incorrectly admitted to the general ward instead of the PBICU. While we have seen a decreasing trend in the number of ward deaths over the 3-year study period, this decline was not significant. This potentially incorrect assessment or underassessment of burn injuries is an area that we should improve on.
The mortality of patients admitted to our unit increased steeply once the TBSA burned rose to >30%. While massive burns (TBSA >60%) were uniformly fatal during the study period, we have had two survivors subsequently.
Numerous major changes have taken place in the unit since the commencement of the study. These have included improvement in human resources with the introduction of paediatric intensivists, a dedicated burn surgeon, and increased numbers of junior and mid-level trainees. Since their introduction, the paediatric intensivists manage all patients admitted to the PBICU. All outside referrals to the PBICU are discussed with the paediatric intensivist, as are patients admitted to the PBICU from casualty after they have initially been assessed and resuscitated by the surgical registrar. The intensivist sees all patients admitted to the PBICU at least twice a day, and also assists with the management of certain patients admitted to the paediatric burns general ward. This includes patients awaiting intensive care unit beds, assistance with antimicrobial coverage and fluid management, and any patient the surgical team may be concerned about. Improved availability and usage of dressings and a perceived general trend towards earlier skin coverage have occurred. Since 2009, there has been a significant decline in the overall mortality rate (Fig. 4) (p=0.0002; Cochran-Armitage test for trend), with mortality during the final year of the study period being similar to those in high-income countries. It is our opinion that this significant decline is largely due to the above changes.
Unfortunately we did not document time taken from admission to achieving skin coverage in this data set, but this will be documented in the future. Clean burn wounds with a TBSA >10% up to a depth of superficial partial thickness have increasingly been covered with Biobrane and Acticoat dressings within the first 24 hours after burn injury. We have also tended towards earlier skin coverage for wounds that would take >2 weeks to heal. Where there was sufficient donor skin on the patient, early split-thickness skin grafting was used. If necessary, the skin was meshed up to a ratio of 3:1. If meshing the skin did not give sufficient skin coverage, attempts were made to procure cadaver donor skin. We have found cadaver donor skin to be very useful. In the majority of our patients, the cadaver skin sloughs between days 10 and 14. The underlying wound can then be skin grafted using healed donor skin sites. Occasionally the underlying wound had begun to epithelialise, negating the need for further skin grafting. More rarely, the cadaver skin had taken completely.
Our challenges in managing massive burns (TBSA >60%) and paying special attention to children aged <5 years are clear. Significant improvement in the management and outcome of children admitted with TBSA burns of 30 - 60% is also required. There are currently two ongoing studies in our unit directly addressing: (i) the impact of paediatric intensivists on our unit; and (ii) the impact of specific dressings on specific populations.
Conclusion
The mortality rate in the Johnson & Johnson Paediatric Burns Unit at CHBAH is 7.9%, having declined significantly over the 3-year study period, and is lower than that quoted in institutions from other LMICs. Age <5 years, the presence of inhalational injury, TBSA >30% and admission to the PBICU were significant risk factors for mortality. We believe that other burn centres in SA should pay special attention to these at-risk populations. In particular, a lower threshold for admission to the PBICU and the early involvement of a paediatric intensivist is recommended.
The importance of the multidisciplinary team in the management of burns is widely known.[14] Advances in wound care and skin coverage continue. Our challenges lie in understanding how best to implement these advances in a resource-constrained environment, and more importantly to ensure that the changes implemented translate into improvements in patient care. If these challenges are successfully met, our long-term goal of achieving and sustaining the standards achieved by major international paediatric burn centres may be realised.
Acknowledgements. We acknowledge and thank Petra Gaylard and the Wits Donald Gordon Medical Centre for their assistance with our statistical analyses, as well as all members of the paediatric surgical, intensive care and allied medical staff that have had such a positive impact on the outcomes of these children.
References
1. You D, New JR, Wardlaw T. Levels and Trends in Child Mortality Report 2012. New York: United Nations Children's Fund, 2012. [ Links ]
2. Nannan N, Dorrington R, Laubscher R, et al. Under-5 Mortality Statistics in South Africa: Shedding Some Light on the Trend and Causes 1997-2007. Cape Town: South African Medical Research Council, 2012. [ Links ]
3. Burrows S, van Niekerk A, Laflamme L. Fatal injuries among urban children in South Africa: Risk distribution and potential for reduction Bull World Health Organ 2010;88:267-272. [http://dx.doi.org/10.2471/BLT.09.068486] [ Links ]
4. Van Niekerk A, Titi N, Lau U, Arendse N. Flame and scalding burns in children. In: Van Niekerk A, Suffla S, Seedat M, Ratele K, eds. Crime, Violence and Injury in South Africa: Enabling Child Safety, 01/2011: chapter; Cape Town: South African Medical Research Council, 2011. [ Links ]
5. Williams FN, Herndon DN, Hawkins HK, et al. The leading causes of death after burn injury in a single pediatric burn center. Crit Care 2009;13(6):R183. [http://dx.doi.org/10.1186/cc8170. [ Links ]]
6. Senel E, Yasti AC, Reis E, Doganay M, Karacan CD, Kama NA. Effects on mortality of changing trends in the management of burned children in Turkey: Eight years' experience. Burns 2009;35(3):372-377. [http://dx.doi.org/10.1016/j.burns.2008.07.020] [ Links ]
7. Brusselaers N, Monstrey S, Vogelaers D, Hoste E, Blot S. Severe burn injury in Europe: A systematic review of the incidence, etiology, morbidity, and mortality. Crit Care 2010;14(5):R188. [http://dx.doi.org/10.1186/cc9300/ccforum.com/content/14/5/R188] [ Links ]
8. Wolf SE, Rose JK, Desai H, et al. Mortality determinants in massive pediatric burns: An analysis of 103 children with 70-80% (full-thickness) TBSA burns. Ann Surg 1997;225(5):554-569. [ Links ]
9. Barrow RE, Spies M, Barrow LN, Herndon DN. Influence of demographics and inhalation injury on burn mortality in children. Burns 2004;30(1):72-77. [http://dx.doi.org/10.1016/j.burns.2003.07.003]. [ Links ]
10. Thombs BD, Singh VA, Milner SM. Children under 4 years are at greater risk of mortality following acute burn injury: Evidence from a national sample of 12902 pediatric admissions. Shock 2006;26(4):348-352. [http://dx.doi.org/10.1097/01.shk.0000228170.94468.e1] [ Links ]
11. Fadeyibi IO, Mustapha IA, Ibrahim NA, et al. Characteristics of paediatric burns seen at a tertiary centre in a low income country: A five year (2004-2008) study. Burns 2011;37(3):528-534. [http://dx.doi.org/10.1016/j.burns.2010.09.015. [ Links ]]
12. Karimi H, Motevalian S-A, Rabbani A, et al. Prediction of mortality in pediatric burn injuries: R-Baux score to be applied in children (Pediatrics-Baux Score). Iran J Pediatr 2013;23(2):165-170. http://ijp.tums.pub/en/articles/1911.html (accessed 6 January 2016). [ Links ]
13. Blom L, van Niekerk A, Laflamme L. Epidemiology of fatal burns in rural South Africa: A mortuary register-based study from Mpumalanga Province. Burns 2011;37(8):1394-1402. [http://dx.doi.org/10.1016/j.burns.2011.07.014] [ Links ]
14. Rode H, Rogers AD, Numanoglu A, et al. A review of primary and secondary burn services in the Western Cape, South Africa. S Afr Med J 2015;105(10):852-857. [http://dx.doi.org/10.7196%2FSAMJnew.8187] [ Links ]
 Correspondence:
Correspondence:
B Jugmohan
benjugmohan@gmail.com
Accepted 20 October 2015.


{kind=link}