










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSAMJ: South African Medical Journal
versão On-line ISSN 2078-5135
versão impressa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.106 no.2 Pretoria Fev. 2016
http://dx.doi.org/10.7196/SAMJ.2016.V106I2.10534
EDITORIAL
Implications of direct-to-consumer whole-exome sequencing in South Africa
Next-generation sequencing (NGS) has truly transformed human genetics and is now an integral discovery tool in the field. Whole-exome sequencing (WES) - an NGS application focused on the protein-coding regions of the human genome - has already bridged the bench-to-bedside divide internationally and is offered as a clinical test by several accredited laboratories.[1,2] Clinical WES is not currently offered in South Africa (SA) for a number of reasons, including technological constraints, insufficient storage for the resulting large datasets, ethical considerations and limitations of our understanding of the impact of human genetic variants on health and in terms of clinical utility. The historical under-representation of individuals of black African descent in genomics research further complicates the interpretation of results obtained from WES data in black Africans.[3]
Concurrently, the application of WES for preventive healthcare in seemingly healthy individuals is progressing rapidly. WES offered as a direct-to-consumer (DTC) genetic test to healthy individuals in aid of wellness and future disease risk prediction raises many critical considerations, some of which were highlighted previously in the SAMJ by the Southern African Society for Human Genetics.[4] This topic is currently back in the headlines as local health insurance company Discovery Health launched their suite of personalised medicine products, which includes WES.[5-7] This offering is presented in partnership with US-based company Human Longevity, Inc. (HLI) under the leadership of J Craig Venter.
The benefits - improved health and precision medicine
Using genome-focused information to improve health outcomes has great potential. This endeavour could benefit South Africans directly, as it is a start to wide-scale research to unravel the genetic basis of diseases in all populations. Combining NGS data with detailed electronic medical and wellness records and family history is a powerful approach towards providing improved health and wellness. Indeed, this is the course that will be taken by President Barack Obama's Precision Medicine Initiative,[8] led by the National Institutes of Health, and the Genomics England Initiative.[9] Similar to these large public research initiatives, private enterprises such as HLI (Discovery's partner) also strive to sequence millions of genomes in order to potentially fast-track drug discovery and improvement through partnerships with pharmaceutical companies. However, in this case it is with the stated additional purpose of commercial gain. Involving SA in this endeavour, and doing so as a DTC service to health insurance clients, raises important concerns, some of which we outline below.
Issues to consider relevant to the implementation of WES in SA
Owing to the comprehensiveness of WES data and our limited understanding of the impact of genetic variation on traits and diseases, the leading concern when dealing with WES in healthy individuals is the appropriate interpretation of results. The likelihood of identifying variants of unknown significance or disease-causing mutations linked to untreatable diseases is high. Interpreting these data in individuals from previously understudied populations (such as black African populations) further complicates interpretation. The analytical sensitivity and specificity of WES should also be considered - diagnostic laboratories offering clinical WES will validate positive findings with an alternative method before releasing diagnostic results. Owing to the uncertainty and concerns relating to the impact of results generated by WES on an individual's health and wellbeing, guidelines have been established by various international professional groups, most notably the American College of Medical Genetics and Genomics.[10]
Closely linked to the uncertainty of data interpretation in WES is the need for adequate pre- and post-test counselling - a service that may be negated if WES is offered direct to the consumer. The health professionals best placed to provide these services are medical geneticists and genetic counsellors. In SA, genetic counsellors and medical geneticists are healthcare professionals registered with the Health Professions Council of South Africa as independent practitioners, with formal tertiary training in their respective professional fields. Both have a deep and broad knowledge of genetics, communication skills to inform and educate a variable audience on the complexities of genetics, psychosocial assessment abilities and the knowledge and ability to apply professional ethics. There is currently a limited number of them in SA, raising concerns that there would be insufficient capacity to provide proper information prior to testing, during informed consent and when test results are received.
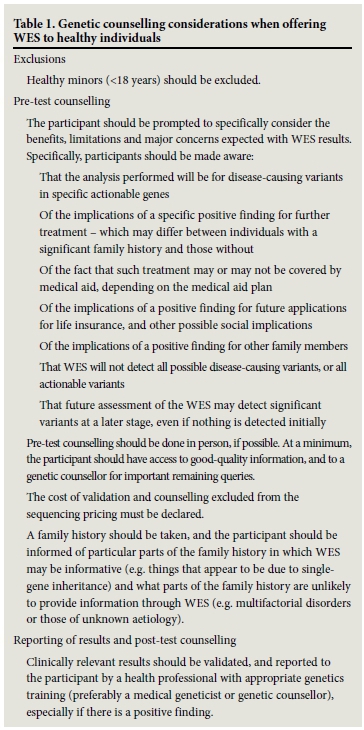
The ethical implementation of WES is crucial and safeguarded by proper pre-test information sharing, counselling and informed consent. Recommendations on what should be considered as part of this process are set out in Table 1. The Discovery/HLI WES offering will implement a broad consent model, with no option to opt out after consent is given, whereas the global trend is to move towards dynamic consent that enables greater participant engagement.'11,121 Post-test counselling for positive results must include practical guidance regarding preventive and therapeutic options, psychosocial support, and the offer of family follow-up. It is crucially important that an appropriate governance framework is in place that restricts exploitative, unapproved use of the data generated. What is important in that framework is that the interests of SA individuals and communities are appropriately considered when granting access to data. Lastly, it is strongly recommended that a local ethics committee review consent documentation and research proposals for this initiative. It would be expected that all these objectives will be in place and approved prior to any testing being offered to participants.
From a legal standpoint, there are many potential pitfalls when offering direct-to-consumer WES. Confidentiality, anti-discrimination and protection of personal information are principles that are embedded in our constitution and legislation. With regard to intellectual property, patenting of DNA sequences is not allowed - however, any new diagnostics and therapeutics developed through the use of DNA sequence data are patentable. Benefit sharing, which can take several forms, should be considered, particularly since participants are paying for the service, if only in part. These details could be included in a material transfer agreement. It should also be remembered that exomes contain a great deal of information beyond disease susceptibility, such as information about ancestry, admixture and so forth. This information needs to be managed with a great deal of care because of the repercussions it might have for individuals and communities involved, including a potential for discrimination. One way of ensuring that secondary use of genomic data is not harmful or exploitative, and that it takes appropriate recognition of contextual factors important in its interpretations, is to carefully govern access to data. There is now considerable experience with regulating access to genomic data globally that should be considered in the Discovery initiative. Managed access to primary data, i.e. limiting access to suitably qualified personnel, should be encouraged.
A final point of consideration is the use of these data for research purposes. Exploitation of local DNA resources with a lack of significant engagement and local capacity development is a reality in the field of genomics, not only in SA but in Africa as a continent.[3,13,14] Although it has been stated that data would potentially be available to local scientists for research purposes, one has to wonder what competitive advantage African scientists will have to utilise these data fully, and whether it would ultimately lead to any kind of capacity development within the SA scientific community. If these date are simply to be used to help a US company to accumulate genome data in order to create a commercialisable private database of DNA and medical records, without any consideration for or intention of addressing urgent health and research needs of the SA population, this endeavour would raise real concern about exploitation.
In conclusion, there are a number of vitally important ethical, legal and scientific concerns that have to be addressed to ensure proper and ethical implementation of this service in SA and that individuals taking part in this endeavour are fully informed of the positive and negative sequelae.
Southern African Society for Human Genetics, Johannesburg, South Africa: Zané Lombard, Fiona Baine, Amanda Krause, Anneline Lochan, Shelley Macaulay, Careni Spencer, Division of Human Genetics, School of Pathology, Faculty of Health Sciences, National Health Laboratory Service, University of the Witwatersrand, Johannesburg, South Africa; Colleen Aldous, School of Clinical Medicine, Nelson Mandela School of Medicine, College of Health Sciences, University of KwaZulu-Natal, Durban, South Africa; Jantina de Vries, Department of Medicine, Faculty of Health Sciences, University of Cape Town, South Africa; Karen Fieggen, Division of Human Genetics, Department of Clinical Laboratory Sciences, Faculty of Health Sciences, University of Cape Town, South Africa; Bertram Henderson, Division of Human Genetics, Faculty of Health Sciences, University of the Free State, Bloemfontein, South Africa; Eileen Hoal, Craig Kinnear, DST/NRF Centre of Excellence for Biomedical Tuberculosis Research/MRC Centre for Molecular and Cellular Biology, Division of Molecular Biology and Human Genetics, Faculty of Medicine and Health Sciences, Stellenbosch University, Tygerberg, Cape Town, South Africa; Noelene Kinsley, GC Network Pty Ltd., Johannesburg, South Africa; Alison September, Division of Exercise Science and Sports Medicine, Department of Human Biology, Faculty of Health Sciences, University of Cape Town, South Africa; Michael Urban, Division of Molecular Biology and Human Genetics, Faculty of Medicine and Health Sciences, Stellenbosch University, Tygerberg, Cape Town, South Africa
Genetic Alliance South Africa, Johannesburg: Himla Soodyall, Division of Human Genetics, School of Pathology, Faculty of Health Sciences, National Health Laboratory Service, University of the Witwatersrand, Johannesburg, South Africa
Southern African Human Genome Programme, Pretoria, South Africa: Michael Pepper, Institute for Cellular and Molecular Medicine, Department of Immunology, Faculty of Health Sciences, University of Pretoria, South Africa; Michele Ramsay, Sydney Brenner Institute for Molecular Bioscience, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
References
1. Volk A, Conboy E, Wical B, Patterson M, Kirmani S. Whole-exome sequencing in the clinic: Lessons from six consecutive cases from the clinician's perspective. Mol Syndromol 2015;6(1):23-31. [http://dx.doi.org/10.1159/000371598] [ Links ]
2. Amendola LM, Lautenbach D, Scollon S, et al. Illustrative case studies in the return of exome and genome sequencing results. Per Med 2015;12(3):283-295. [http://dx.doi.org/10.2217/pme.14.89] [ Links ]
3. De Vries J, Tindana P, Littler K, et al. The H3Africa policy framework: Negotiating fairness in genomics. Trends Genet 2015;31(3):117-119. [http://dx.doi.org/10.1016/j.tig.2014.11.004] [ Links ]
4. Dandara C, Greenberg J, Lambie L, et al. Direct-to-consumer genetic testing: To test or not to test, that is the question. S Afr Med J 2013;103(8):510-512. [http://dx.doi.org/10.7196/samj.7049] [ Links ]
5. Discovery to offer genetic testing to Vitality members. The Citizen, 23 September 2015. http://citizen.co.za/784172/discovery-to-offer-genetic-testing-to-vitality-members/ (accessed 6 November 2015). [ Links ]
6. Discovery Health. New product and benefit enhancements for 2016. https://http://www.discovery.co.za/portal/individual/medical-aid-news-product-enhancements-2016 (accessed 6 November 2015). [ Links ]
7. SA insurer offers cheap whole exome sequencing. Medical Brief 22 September 2015. http://www.medicalbrief.co.za/archives/sa-insurer-offers-cheap-whole-exome-sequencing/ (accessed 6 November 2015). [ Links ]
8. Collins FS, Varmus H. A new initiative on precision medicine. N Engl J Med 2015;372(9):793-795. [http://dx.doi.org/10.1056/NEJMp1500523] [ Links ]
9. Manolio TA, Abramowicz M, Al-Mulla F, et al. Global implementation of genomic medicine: We are not alone. Sci Transl Med 2015;7(290):290ps213. [http://dx.doi.org/10.1126/scitranslmed.aab0194] [ Links ]
10. Green RC, Berg JS, Grody WW, et al. ACMG recommendations for reporting of incidental findings in clinical exome and genome sequencing. Genet Med 2013;15(7):565-574. [http://dx.doi.org/10.1038/gim.2013.73] [ Links ]
11. Kaye J, Whitley EA, Lund D, Morrison M, Teare H, Melham K. Dynamic consent: A patient interface for twenty-first century research networks. Eur J Hum Genet 2015;23(2):141-146. [http://dx.doi.org/10.1038/ejhg.2014.71] [ Links ]
12. Steinsbekk KS, Kare Myskja B, Solberg B. Broad consent versus dynamic consent in biobank research: Is passive participation an ethical problem? Eur J Hum Genet 2013;21(9):897-902. [http://dx.doi.org/10.1038/ejhg.2012.282] [ Links ]
13. De Vries J, Pepper M. Genomic sovereignty and the African promise: Mining the African genome for the benefit of Africa. J Med Ethics 2012;38(8):474-478. [http://dx.doi.org/10.1136/medethics-2011-100448] [ Links ]
14. Hoal E. Famine in the Presence ofthe Genomic Data Feast. Science 2011;331(6019):874. [http://dx.doi.org/10.1126/science.1203261] [ Links ]
 Correspondence:
Correspondence:
Zané Lombard
zane.lombard@wits.ac.za

