










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSAMJ: South African Medical Journal
versión On-line ISSN 2078-5135
versión impresa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.105 no.12 Pretoria dic. 2015
http://dx.doi.org/10.7196/samj.2015.v105i12.10225
CONTINUING MEDICAL EDUCATION
ARTICLE
M N Abrahams
MB ChB, FCP (SA), Cert Rheumatology (SA). Division of Rheumatology, Department of Medicine, Faculty of Health Sciences, Groote Schuur Hospital and University of Cape Town, and Gatesville Medical Centre, Cape Town, South Africa
ABSTRACT
Gout is the most common crystal arthritis and its prevalence is rising. It is associated with the metabolic syndrome, and hyperuricaemia may be an independent risk factor for cardiovascular disease. The acute presentation of gout is easily managed, but the underlying cause is seldom addressed. Indications for initiating uric acid therapy have been clearly established. The classification criteria for gout have been reviewed and are presented here.
Lifestyle modification is key to the management of gout. The clinician must screen for diabetes, hypertension and hypercholesterolaemia when the diagnosis of gout is made. The management of asymptomatic hyperuricaemia is still being researched. As yet, there is no indication to start urate-lowering therapy in such patients. Allopurinol remains the first line of treatment, but there are newer drugs being researched in various clinical trials. Probenecid is the alternative in patients with preserved renal function, who do not have a history of renal calculi.
Gout is the most common inflammatory arthritis. Worldwide, gout and hyperuricaemia are on the rise owing mainly to dietary changes, obesity, the metabolic syndrome and increasing age. In the past 2 decades the prevalence of gout has doubled owing mostly to changes in diet. Western diets rich in meat, seafood, fructose-sweetened drinks and beer have especially been identified.[1]
Gout has two clinical presentations that affect the musculoskeletal system - acute arthritis and chronic tophaceous gout. The acute attack results in the person experiencing severe pain and swelling of the affected joint, which impairs quality of life. In between attacks patients are asymptomatic.
In tophaceous gout, patients develop a chronic debilitating arthritis with loss of function. Tophi cause erosions of joints, but also deposit in the skin and soft tissue, including the bursae, tendons and articular cartilage. Tophi are the pathognomonic features of gout. Renal manifestations include kidney stones and rarely an interstitial nephritis.
The acute attack can be very easily managed by using non-steroidal anti-inflammatory drugs (NSAIDs), colchicine or glucocortico-steroids, followed up by lifestyle modification and, if appropriate, urate-lowering therapy (ULT). The indications to commence ULT are:
-
Recurrent attacks (>2).
-
Tophaceous gout.
-
Radiological evidence of erosive disease.
Pathogenesis
Gout results from the accumulation of uric acid, which is formed as the end result of purine metabolism. Xanthine oxidase is an import enzyme in the purine pathway, which ultimately results in the formation of uric acid. The majority of purines are endogenous, while diet is a source of exogenous purines. High fructose results in hyperuricaemia via the fructose phosphokinase shunt.
The body regulates uric acid primarily in the kidneys. After uric acid is filtered by the glomerulus, almost all of it is reabsorbed in the proximal convoluted tubule. This is followed by secretion of uric acid back into the tubules before being reabsorbed again. The net effect is that only 5 - 10% of filtered uric acid is lost through the kidneys. There are various transporters within the tubules that are involved in this complex uric acid transport. Uric acid transporter 1 (URAT1) and organic anion transporter 4 (OAT4) are transporters in the proximal tubules that reabsorb uric acid and have been identified as targets for future treatments.
When the serum concentration of uric acid rises above the saturation point to >0.42 mmol/L, uric acid crystallises. These are deposited into joints and various tissues, forming tophi. The microtophi are sealed off by proteins, and consequently do not cause an inflammatory response. The tophi may rupture, exposing the monosodium urate (MSU) crystals to circulating macrophages. Joint damage, dehydration and cool peripheral temperatures may cause the microtophi to rupture, thus exposing the MSU to tissue macrophages. MSU crystals are then engulfed by macrophages, which set off an inflammatory response where interleukin 1 beta, among other pro-inflammatory cytokines, is activated. This results in an acute inflammatory process with swelling, redness, warmth and tenderness of the affected joint.[2]
Diagnosis
The definitive diagnosis of gout is made when MSU crystals are observed in a joint aspirate. Any patient who presents with an acute monoarthritis needs the joint aspirated to exclude sepsis and has to be assessed for crystals. A history of recurrent self-limiting joint pain is suggestive of gout. When one includes podagra and the presence of tophi, the specificity increases. Serum urate is often helpful with the diagnosis, but it cannot be the only criterion on which the diagnosis is based. The urate level may be normal in an acute attack and conversely may be elevated in asymptomatic individuals.[3] The demonstration of MSU does not exclude the possibility of another cause of monoarthritis. Importantly, sepsis and trauma may coexist in an inflamed joint.
Once a diagnosis of gout is made, the modifiable risk factors must be assessed.
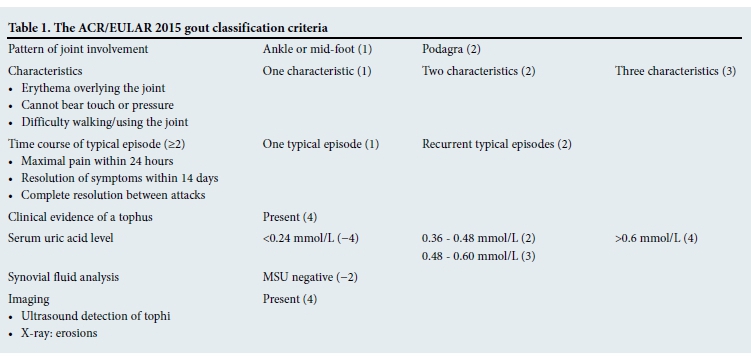
The American College of Rheumatology/European League Against Rheumatism (ACR/EULAR) 2015 gout classification criteria (Table 1) have recently been published. They propose a 3-step process for making the diagnosis of gout:[4]
-
Step 1. Entry criterion: at least 1 episode of swelling or tenderness in a peripheral joint or bursa.
-
Step 2. Sufficient clinical criteria (if met, can classify as gout; then step 3 is not necessary): presence of MSU crystals in a symptomatic joint or bursa or the presence of tophus.
-
Step 3. If Step 2 does not confirm the diagnosis, then use the given scoring system in Table 1. A score of >8 is sufficient for the diagnosis of gout.
Treatment
The acute attack
The management of the acute attack is very effective and may be a contributing factor as to why gout is poorly managed. The effectiveness of the acute management may make the patient forget about the more important ULT.
NSAIDs, colchicine and corticosteroids are all effective in managing the acute attack. The choice of anti-inflammatory drug will depend on the risk of side-effects and comorbidities. Patients do report that early treatment at the first sign of pain may abort a full attack. Once established, the acute attack will last for several days before it resolves.
Colchicine is particularly effective in the acute attack, but the therapeutic window is very narrow. Gastrointestinal side-effects are especially common and may cause unwanted problems in patients who are immobilised as a result of the acute attack. Oral corticosteroids are equally effective; however, patient selection is important, e.g. corticosteroids are more effective than NSAIDs in patients with renal disease but not ideal in diabetics with sepsis. The patient profile will determine the agent of choice.[5-7]
Intra-articular steroids are also effective in the acute attack, but have not been well studied. They are favoured in acute monoarthritis after aspirating the joint to dryness.
Lifestyle modification
Lifestyle modification and dietary changes should be addressed at the first attack of gout. One should screen for comorbidities because of the strong association with the metabolic syndrome. Hypertension, diabetes and dyslipidaemia should be considered. Chronic medication should be reviewed to ensure that there are no drugs that will cause hyperuricaemia. Alternatives to thiazide diuretics should be selected and low-dose aspirin indications scrutinised. Weight reduction should be advised and alcohol intake reduced. Beer must be avoided at all costs. Foods high in purines should be avoided. Most people are aware that offal and oily fish are sources of purines, but certain vegetables are also high in purines. Mushrooms, broccoli and spinach have a moderate content of purines and may also need to be avoided. High-fructose corn syrup (HFCS) is an artificial sweetener that is used in many different food products. A high fructose intake will increase uric acid production via the phosphokinase shunt. The ingredients of fruit juices, cereals, sauces, syrups and even breads may include HFCS.
Angiotensin receptor blockers have a mild uricosuric effect and may help with lowering uric acid levels.
Urate-lowering therapy
The goal of ULT is to decrease the uric acid level below the saturation point. A treat-to-target strategy should be started with the goal of lowering the urate level to 0.35 mmol/L. In tophaceous gout the target should be lower.
Allopurinol is the first line of treatment for gout. It is a xanthine oxidase inhibitor and decreases uric acid production. It has been shown to be effective in both under-excretors (under-secretors) and over-producers of uric acid. Ideally, allopurinol should be started once the acute attack has settled. Twenty percent of patients will experience the acute attack when starting allopurinol. Colchicine should be used as prophylaxis to prevent acute flares when starting daily allopurinol - up to at least 3 months.
Allopurinol should be started at 100 mg daily and the uric acid levels checked every 4 weeks. Allopurinol should be increased by 100 mg until the target is reached. Allopurinol hypersensitivity syndrome (AHS) is a rare side-effect in 0.1% of patients. It entails a desquamating rash, fever and hepatitis and is potentially life threatening. Pre-existing renal disease is the main risk factor for AHS. Patients should be advised to discontinue allopurinol if they develop a rash and seek urgent medical attention.[6-8]
Febuxostat is another xanthine oxidase inhibitor that is used to lower uric acid.
Probenecid is a uricosuric agent and an alternative to allopurinol. It inhibits urate reabsorption in the proximal convoluted tubule.
It is contraindicated in renal failure and in patients who have urolithiasis. Probenecid is not as effective as allopurinol.
Losartan and fenofibrate both have mild uricosuric effects and may be used in combination with the conventional therapies to lower uric acid levels.
Pegloticase is a pegylated recombinant uricase that converts uric acid to allopurinol. It has been licensed by the US Food and Drug Administration (FDA) for refractory tophaceous gout. It is associated with transfusion reactions and immunogenicity.
Asymptomatic hyperuricaemia
Hyperuricaemia has been shown to be associated with the metabolic syndrome. However, only a third of patients with hyperuricaemia develop gout. It is still not clear whether hyperuricaemia is an independent risk factor for cardiovascular disease and whether initiating therapy in patients with asymptomatic hyperuricaemia will be beneficial. Currently, ULT is not indicated in these patients. This is an area of ongoing research.[7]
Conclusion
Gout and hyperuricaemia are becoming more common. Gout can be effectively managed by targeting serum acid and aggressively lowering the level to 0.35 mmol/L. Comorbid diseases and other drugs provide challenges in managing gout. Lifestyle modification is an essential component in the management of gout, particularly dietary changes, maintaining a normal weight and a reduction/ avoidance of alcohol. The management of asymptomatic hyper-uricaemia and its role in cardiovascular disease are areas of ongoing research.
References
1. Hak AE, Choi HK. Lifestyle and gout. Curr Opin Rheumatol 20038;20:178-186. [http://dx.doi.org/10.1097/BOR.0b013e3282f524a2] [ Links ]
2. Terkeltaub R. Update on gout: New therapeutic strategies and options. Nat Rev Rheumatol 2010;6:30-38. [http://dx.doi.org/10.1038/nrrheum.2009.236] [ Links ]
3. Malik A, Schumacher HR, Dinnella JE. Clinical diagnostic criteria for gout: Comparison with the gold standard of synovial fluid crystals. J Clin Rheumatol 2009;15:22-24. [http://dx.doi.org/10.1097/RHU.0b013e3181945b79] [ Links ]
4. Neogi T, Jansen TL, Dalbeth N, et al. 2015 Gout Classification Criteria. Arthritis Rheumatol 2015;67(10):2557-2568. [http://dx.doi.org/10.1002/art.39254] [ Links ]
5. Baker JF, Schumaker H. Update of gout and hyperuricaemia. Int J Clin Pract 2010;64(3):371-377. [http://dx.doi.org/10.1111/j.1742-1241.2009.02188.x] [ Links ]
6. Neogi T. Clinical practice of gout. N Engl J Med 2011;364:443-452. [http://dx.doi.org/10.1056/NEJMcp1001124] [ Links ]
7. Weisman M. Targeted Treatment of the Rheumatic Diseases. Philadelphia: Saunders Elsevier, 2010:293-302. [ Links ]
8. Khanna D, Fitzgerald J, Khanna P, et al. 2012 American College of Rheumatology guidelines for the management of gout. Part 1: Systematic non-pharmacological and pharmacologic therapeutic approaches to hyperuricaemia. Arthritis Care Research 2012;64(10):1431-1446. [http://dx.doi.org/10.1002/acr] [ Links ]
 Correspondence:
Correspondence:
M N Abrahams
nur.abrahams@me.com


{kind=link}