










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSAMJ: South African Medical Journal
versão On-line ISSN 2078-5135
versão impressa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.105 no.8 Pretoria Ago. 2015
http://dx.doi.org/10.7196/SAMJNEW.7890
RESEARCH
Human papillomavirus genotypes and clinical management of genital warts in women attending a colposcopy clinic in Cape Town, South Africa
S TayibI, II; B AllanIII; A-L WilliamsonIV, V; L DennyVI
IMB ChB, MMed (O&G), Fellowship in Gynaecology Oncology (Malaysia). Department of Obstetrics and Gynaecology, Hospital Pulau Pinang, Penang, Malaysia
IIMB ChB, MMed (O&G), Fellowship in Gynaecology Oncology (Malaysia). Gynaecological Oncology Unit, Department of Obstetrics and Gynaecology, Groote Schuur Hospital and Faculty of Health Sciences, University of Cape Town, South Africa
IIIMSc. Institute of Infectious Disease and Molecular Medicine and Division of Medical Virology, Faculty of Health Sciences, University of Cape Town, South Africa
IVPhD. Institute of Infectious Disease and Molecular Medicine and Division of Medical Virology, Faculty of Health Sciences, University of Cape Town, South Africa
VPhD. National Health Laboratory Service, Cape Town, South Africa
VIMB ChB, MMed (O&G), PhD, FCOG (SA). Gynaecological Oncology Unit, Department of Obstetrics and Gynaecology, Groote Schuur Hospital and Faculty of Health Sciences, University of Cape Town, South Africa
ABSTRACT
BACKGROUND: Genital human papillomavirus (HPV) infection is the most common sexually transmitted viral disease in the world. HPV infection of the genital epithelium is associated with genital warts and malignancies of the lower genital tract.
OBJECTIVES: To describe the distribution, phenotypic appearance and HPV type associated with genital warts in women.
METHODS: This was a prospective observational study of all women with genital warts who attended the Colposcopy Clinic, Groote Schuur Hospital, Cape Town, South Africa, during 2010 and fulfilled the inclusion and exclusion criteria. One hundred and thirteen women were tested for HPV using the Roche Linear Array HPV genotyping kit to determine the HPV genotypes causing genital warts.
RESULTS: The median age of the women was 27 years (range 15 - 53); 90 (79.6%) were HIV-positive, and two-thirds were on antiretroviral treatment. Treatment involved ablation with topical agents, cauterisation or carbon dioxide laser. At 3 months' follow-up after treatment, 56.6% of the women, the majority of whom were HIV-positive, had recurrent/persistent disease. In both HIV-positive and HIV-negative women, HPV was detected in over 90% of cases. However, over half the HIV-positive women as opposed to 2/18 of the HIV-negative women were infected with multiple HPV genotypes. The commonest HPV genotypes in HIV-positive and HIV-negative women were types 11, 6, 89, 61, 55 and 62 and types 11 and 6, respectively.
CONCLUSIONS: The majority of the patients were HIV-positive and had multiple HPV infections. While this did not alter the phenotypic appearance of the warts, recurrence/persistence after treatment was more common.
Genital human papillomavirus (HPV) infection is the most common sexually transmitted viral disease in the world.[1,2] HPV infection of the genital epithelium is associated with a range of diseases, including genital warts and cancers of the cervix, vagina, vulva, anus and penis and their precursors. However, HPV infection may exist in the latent form in apparently normal epithelium.[3,4] Genital warts are typically associated with low-risk HPV genotypes, most commonly HPV types 6 and 11.[5] However, recent studies have shown that 20 - 50% of genital warts may be co-infected with high-risk HPV types associated with malignancy.[6,7]
Although genital warts are not life-threatening, they cause significant psychosocial harm, including low self-esteem, negative self-perception, embarrassment and anxiety.[8,9] Genital warts represent a health problem for the individual, and carry a significant economic burden for society owing to their generally poor response to conventional therapies and the need for multiple therapeutic interventions.[9] Immunisation against high-risk HPV types to prevent cervical cancers is likely to have a positive public health impact in the future. In addition, the quadrivalent vaccine, which has been approved for use in males and females aged 9 - 26 years, protects against the HPV types that cause 90% of genital warts (i.e. types 6 and 11).[4]
Genital warts are a common reason for referral to the Colposcopy Clinic at Groote Schuur Hospital (GSH), a tertiary hospital serving the Cape Town area and the Western Cape Province, South Africa. We undertook this study to examine the nature of the disease, seeking particularly to determine the rate of recurrence after treatment, the response to various therapies using trichloroacetic acid (TCA), electrocautery and carbon dioxide laser, and the HPV genotypes associated with genital warts in women referred to our clinic.
Objectives
To describe the demographic features of women diagnosed with genital warts, the characteristics of genital warts seen and treatment modalities used, and to determine the type of HPV infections associated with warts according to HIV status and response to treatment at 3 months.
Methods
Study design
This was a prospective observational study performed over a 6-month period (1 April - 30 September 2010). Subjects were recruited from women diagnosed with genital warts referred to the Colposcopy Clinic at GSH. Those who were pregnant or unable to undergo gynaecological examination were excluded.
Written informed consent was obtained from all participants in their home language (English, Afrikaans or Xhosa), with subsequent back-translation to ensure accuracy. Approval for the study was obtained from the Human Research Ethics Committee of the University of Cape Town and the GSH Bioethics Unit. Separate consent was sought for photographing the warts.
At enrolment, each participant was interviewed using a structured questionnaire. A urine pregnancy test was performed prior to clinical examination if the patient had been amenorrhoeic for more than a month and/or was not using contraception. All participants had a detailed examination of the anogenital area, and a macroscopic photograph of the lesions was taken. Cervical and anal smears were taken during colposcopy, which was followed by detailed examination of the cervix, vagina, vulva and anus. Any acetowhite areas observed during colposcopy of the cervix and any macroscopically visible anogenital warts were biopsied for histological investigation. The anal smears were not examined for this study. All patients received serological screening for HIV and syphilis. Those confirmed as HIV-positive had CD4 cell counts and HIV viral load determined in accordance with HIV management guidelines at the time of the study.
HPV analysis
HPV DNA analysis was performed at the Institute of Infectious Disease and Molecular Medicine, University of Cape Town. All biopsy specimens for HPV DNA analysis were given a unique identification number that was matched to the participant's data and was only known to the principal investigator. The specimens were each placed in a separate container with the specific identification number and collected by the testing laboratory on a daily basis. When the sample was appropriately sized, the Qiagen DNA extraction mini-kit (cat. 51304) was used to complete extraction. For biopsy samples in excess of the recommended size, the Qiagen protocol was used only to provide a first-step digestion lysate of tissue. Anogenital wart biopsy DNA was subjected to HPV typing employing the Roche Linear Array HPV genotyping kit (testing for HPV types 11, 16, 18, 26, 31, 33, 35, 39, 40, 45, 51, 52, 53, 54, 55, 58, 59, 61, 62, 66, 68, 70, 72, 73, 81, 82, 83, 84 and 89) according to the manufacturer's instructions (Roche Molecular Systems, USA).
The HPV target DNA for amplification was a 450-bp fragment of the L1 region. To confirm sample quality and the DNA extraction process, a second target was a 268-bp fragment of the human β-globin gene. A sample was considered adequate if it was β-globin-positive (internal control) or β-globin-negative but HPV DNA-positive.
Pathology
Cervical cytology and biopsy specimens for histological confirmation were interpreted by pathologists at the GSH pathology laboratory. The pathologists examining the specimens were not blinded as to the HIV status of the participants.
Treatment modalities
All participants received treatment based on the morphology and distribution of lesions. The lesions were classified as small, moderate, and large or extensive. Small lesions referred to multiple small warts around the genitalia of diameter <0.5 cm, moderate lesions to warts with diameter 0.5 - 1.0 cm, and large or extensive lesions to a perineum infiltrated by warts.
Treatments involved topical application of TCA; electrocautery or excision under local or general anaesthesia; or ablation with a CO2 laser under general anaesthesia, depending on the size of the warts. Women with small warts received topical treatment with TCA and were advised to attend weekly until no visible lesions were seen. Women with warts of moderate size were treated with electrocautery under local anaesthesia in the clinic setting. Women requiring general anaesthesia for excision of large or extensive warts or CO2 laser were given a date for admission to the ward for laser ablation and surgery.
All patients were seen after treatment for follow-up assessment of their response. The wart(s) were categorised as recurrent if recurring 3 months after treatment, or persistent if recurring less than 3 months after treatment. Patients who were found to be HIV-positive were referred to a social welfare officer for post-test counselling and subsequently referred for management at their local HIV clinic for initiation of antiretroviral treatment (according to the 2010 Clinical Guidelines on the Management of HIV and AIDS in Adults and Adolescents of the National Department of Health, SA[10]).
Data collection and statistical analysis
To guarantee confidentiality, all participants were allocated a unique study number. Data obtained were entered into an anonymous database and data analysis was performed using SPSS Statistical Software, version 19.
Ethical considerations
Ethical approval was obtained from the Research Ethics Committee of the Faculty of Health Sciences, University of Cape Town (Ref. 131/2010).
Results
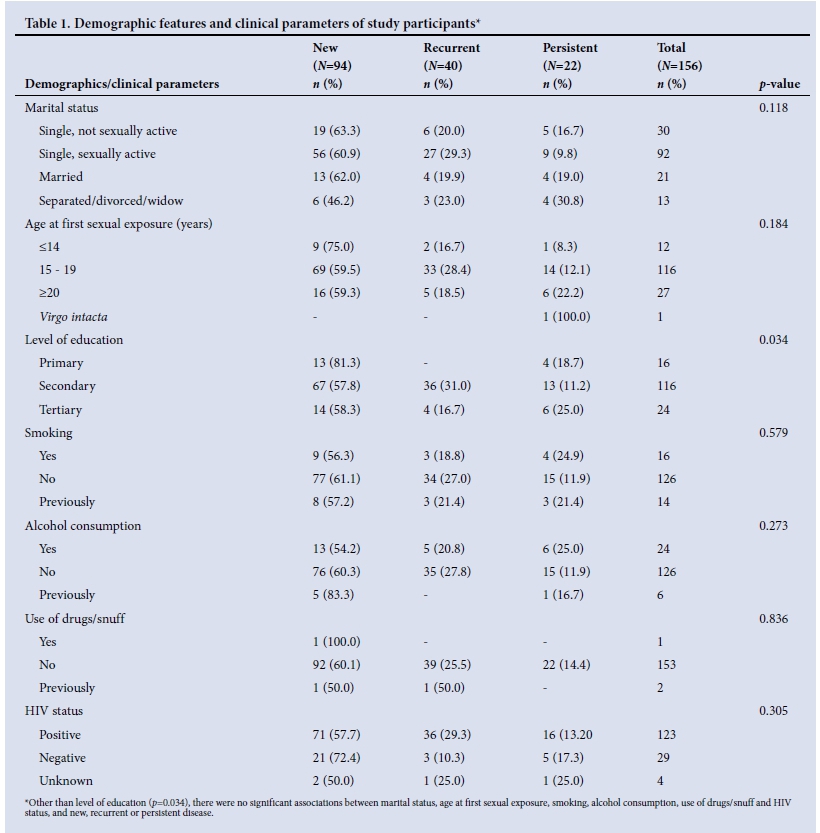
A total of 156 patients (mean age 27 years, range 15 - 53) participated in the study. Ninety-four patients (60.3%) were new cases, 40 (25.6%) were recurrent cases and 22 (14.1%) had been treated previously but had persistent disease. Table 1 summarises the demographic and clinical characteristics of the participants. More than 50% of the women were single (not legally married) but sexually active. The majority (n=128, 82.1%) had had their first sexual encounter before the age of 20 years, often between the ages of 15 and 19.
The majority of the women (123/156, 78.8%) were HIV-positive (Table 1). Four patients declined HIV screening and were categorised as 'HIV status unknown'. Of the HIV-positive women, 83/123 (67.5%) were already on antiretroviral therapy with a median CD4 count of 356 cellsμL (range 22 - 483).
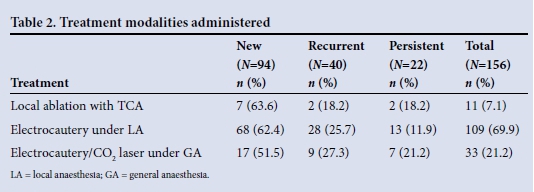
Table 2 shows the modalities of treatment administered. Local ablation with TCA and electrocautery under local anaesthesia were performed on patients with lesions of small to moderate size. Patients with large and extensive lesions received CO2 laser. The average length of hospital stay for these patients was 5.1 days (range 1 - 7) owing to poor home circumstances and requirement for wound care. Histological examination confirmed genital warts in 154 patients. Two of the 156 specimens (1.3%) were reported as invasive squamous cell carcinoma, and these patients were treated with radical wide local excision of the lesions and groin node dissection. Both were HIV-positive.
One hundred and thirteen of the 156 specimens were successfully investigated for HPV with positive β-globin tests. Of these 113 specimens, 7 (6.2%) had no detectable HPV DNA. Table 3 shows the relationship between HPV DNA detection and HIV status. Of 106 HPV DNA-positive patients, 85 (80.2%) were HIV-positive.
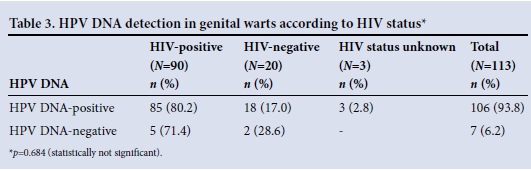
Table 4 shows the association between HPV DNA status and cervical cytological abnormalities. Seventy of 106 HPV DNA-positive women (66.0%) had cervical cytological abnormalities noted: high-grade squamous intraepithelial lesions (HSILs) in 8.5% (9/106) and low-grade squamous intraepithelial lesions (LSILs) in 52.8% (56/107). Thirty-six of 106 patients with HPV DNA-positive warts (34.0%) had normal cervical cytological findings. Women with cervical abnormalities were subsequently recalled and managed according to standard clinical protocols.
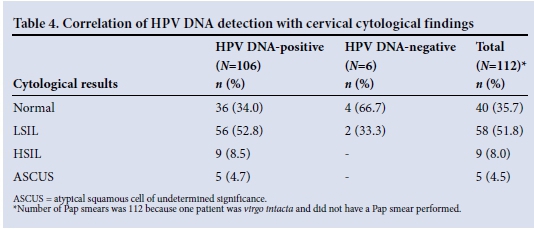
Of the 7 women with no HPV DNA detectable from biopsied genital warts, 2 had LSILs, 4 had normal cytological findings, and 1 had no cervical cytology performed (virgo intacta).
Table 5 shows the HPV genotypes detected from anogenital warts. The ten most frequent types detected were HPV 11, 6, 89, 61, 55, 62, 81, 16, 18 and 45. HPV genotypes 6 and 11 were the most common genotypes encountered in both HIV-positive and negative women. In addition to the most prevalent genotypes 6 and 11, HIV-positive cases yielded types 16, 18, 31, 33, 35, 39, 40, 45, 51, 52, 53, 54, 55, 58, 59, 61, 62, 66, 68, 70, 72, 73, 81, 82, 83, 84 and 89. Fifteen of 85 HIV-positive women who were HPV DNA-positive (17.6%) were co-infected with HPV 16 and 18, among other types.
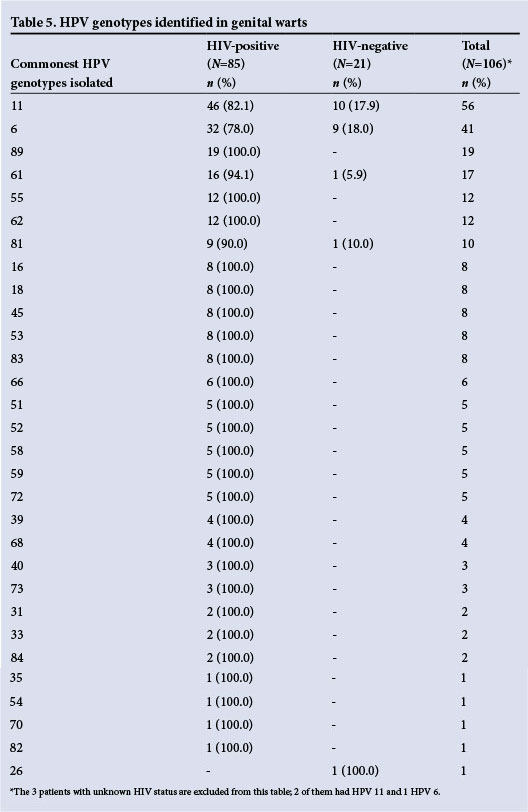
Of the 106 women who were positive for HPV DNA, 58 (54.7%) had a single genotype identified. Co-infection with more than one genotype was detected in 43/85 HIV-positive women (50.6%) as opposed to 3/18 HIV-negative women (16.7%). This difference was statistically not significant (p=0.771), possibly owing to the small number of HIV-negative cases. Among the HIV-positive cases, 15 genotypes were detected from one patient and 11 genotypes from two patients. The maximum number of HPV genotypes detected from HIV-negative women was three, detected in two specimens. One of the two specimens with histological confirmation of invasive squamous cell carcinoma was available for HPV typing and had seven HPV types detected (HPV 11, 16, 53, 55, 61, 62 and 89).
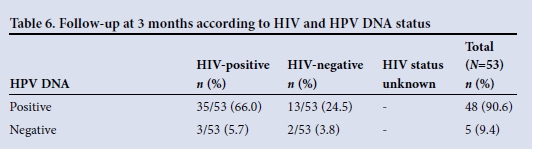
Fifty-three of 113 women for whom HPV analysis could be performed (46.9%) returned for follow-up 3 months after treatment. Of this group, 35 (66.0%) were HIV- and HPV DNA-positive and 13 (24.5%) were HIV-negative but HPV DNA-positive (Table 6). The majority of recurrences at 3 months' follow-up were in HIV-positive women (26/30, 86.7%). In the HIV- and HPV DNA-positive group, 25 women (71.4%) had recurrent genital warts compared with three women (23.1%) in the HIV-negative, HPV DNA-positive group (p=0.114). Recurrent genital warts were seen more often in women with more than one HPV genotype initially detected (40%, 10/40) than in those with a single detectable genotype (60%, 15/25) (p=0.172).
The most common HPV types detected were HPV 11 (54.7%, 58/106) and HPV 6 (39.6%, 42/106). Three women had dual HPV 6 and HPV 11 infection. Of note, 39/106 (36.8%) of women were infected with high-risk HPV types such as 16, 18, 31, 33, 35, 39, 45 and 51. Only nine women (8.5%) had no infection with either HPV 6 or 11.
Discussion
It is well known that persistent infection with HPV is a necessary precursor for the development of cervical cancer. Infection with HPV is also associated with genital warts and other types of anogenital neoplasia, including penile, anal and oropharyngeal tumours.[11] Although genital warts are not life threatening, they are common and cause considerable psychosocial and sexual morbidity.[9] Genital warts in both men and women are readily transmitted, have a high recurrence rate after treatment, and cause local pain and discomfort.[9,12] Treatment for genital warts also requires multiple clinical visits associated with increased cost. In the USA, the cost was highest in young adults (USD1 717/1 000 person-years) for women aged 15 - 24 years.[13]
Main findings
In this study, the mean age of the patients recruited was 27 years; 63 (40.4%) were aged <25. This is consistent with the known prevalence of HPV infection, which peaks at age 15 - 25 years.'41 A number of studies show that the occurrence of genital warts is strongly linked with sexual behaviour, and more weakly associated with cigarette smoking. [14] More than 80% of patients in this study were sexually active, and 80.1% had had more than one sexual partner. However, only 19.2% were current or ex-smokers. It has been postulated that cigarette smoking is associated with more risky sexual behaviours, and biologically with decreased S-100 and CD1a-positive Langerhans cells in the cervical epithelium.[14]
It is well known that HIV infection is an important risk factor for HPV infection and persistence. HIV-seropositive women are at increased risk of contracting HPV infection and developing HPV-related preinvasive and invasive lesions compared with their seronegative counterparts.'3,41 In addition, HIV-seropositive women have a high rate of persistent HPV infection with high-risk HPV genotypes (16 and 18),[5] which are responsible for 70% of cervical cancers.
In this study, the majority of the patients (n=123, 78.9%) were HIV-positive. HIV seropositivity and HIV-induced immune suppression are known to be associated with an increased prevalence of anogenital HPV infections in men and women. This association involves HPV infection of all types, as well as infections with multiple types of HPV, including the oncogenic types.'151 Our study showed that HIV-infected women not only had genital warts with more HPV genotypes, with the maximum number being 15 in one patient, but also had multiple oncogenic types of HPV. HPV types 6 and 11 were detected in most cases (85.8%). The role of the other HPV types in the pathogenesis of genital warts is unknown. It is also not clear what the implications are in terms of HPV vaccination, as this raises the question as to whether the other types will also cause genital warts.
Study strengths and limitations
The strength of this study is that it was conducted prospectively, with detailed documentation of the clinical diagnosis of genital warts by one clinician. Limitations include the short follow-up period of only 3 months, with a significant number of patients lost to follow-up. Furthermore, these data refer to a group of women referred specifically for genital warts and cannot be considered to be representative of the general population.
Interpretation
Our data show that HIV-infected women have a high incidence of HPV infection and infection with multiple types of HPV, including high-risk types. Recently, some investigators have suggested that HPV infection is a risk factor for HIV transmission. Lissouba et al.,[16] in their systematic review and meta-analysis of 2 601 abstracts, six observational studies and 6 567 participants, found that HIV acquisition was significantly associated with HPV infection (summary odds ratio (OR) 1.96; 95% confidence interval (CI) 1.55 - 2.49). HIV incident infection was significantly associated with high-risk HPV in five of six studies and with low-risk HPV in two out of five. The association was significant for high-risk HPV (summary OR 1.92; 95% CI 1.49 - 2.46) and borderline for low-risk HPV. However, our study was not designed to evaluate the impact of HPV infection on HIV transmission. This study showed that HIV co-infection is a risk factor for infection with multiple HPV genotypes.
Conclusions
There was a high rate of HIV positivity among women with genital warts recruited into the study. HPV-associated disease is likely to become a major clinical issue in HIV-positive women, because: (i) both HPV and HIV viruses are transmitted sexually; and (ii) clearance of HPV infection relies on functional cell-mediated immunity, precisely the immune system attacked by HIV infection. There is an urgent need for effective strategies for management of HPV-associated disease in HIV-positive women. This may be achieved through extensive public education programmes on the prevention and transmission of HPV, as well as HIV and HPV vaccination. HPV vaccination with the quadrivalent vaccine (Gardasil; Merck, USA) has recently been shown to significantly reduce the incidence of genital warts in individuals less than 21 years of age in Australia and New Zealand.[17,18]
Acknowledgements. We thank all staff members of the GSH Colposcopy Clinic.
Conflict of interest. ST: none; BA: none; ALW: none; LD: has received honoraria for appearing on various speaker forums on HPV vaccination from GlaxoSmithKline and MSD/Merck and has received research funding from both organisations.
Contributions to authorship. ST: study design, data collection and analysis, data interpretation, writing of manuscript and literature search; BA: performed HPV typing tests, data collection and analysis, data interpretation, writing of manuscript; ALW: head of HPV testing laboratory, data interpretation and writing of manuscript; LD: study design, data collection and analysis, data interpretation and writing of manuscript
Funding. This study was supported by a research grant from Investigator-Initiated Studies Program of Merck Sharp & Dohme. The opinions expressed in this article are those of the authors and do not necessarily represent those of Merck Sharp & Dohme. This work was also partially based upon research supported by the South African Research Chairs Initiative of the Department of Science and Technology and the National Research Foundation.
References
1. Kjaer SK, Tran TN, Sparen P, et al. The burden of genital warts: A study of nearly 70000 women from general female population in the 4 Nordic countries. J Infect Dis 2007;196(10):1447-1454. [http://dx.doi.org/10.1086/522863] [ Links ]
2. Hagensee ME. Infection with human papillomavirus: Update on epidemiology, diagnosis and treatment. Curr Infect Dis Rep 2000;2(1):18-24. [http://dx.doi.org/10.1007/s11908-000-0083-z] [ Links ]
3. Singer A, Monaghan JM, Quek SC, Deery ARS. Human papillomaviruses in pathogenesis of lower genital tract neoplasia (chapter 2). In: Singer A, Monaghan JM, Quek SC, Deery ARS, eds. Lower Genital Tract Precancer: Colposcopy, Pathology and Treatment. 2nd ed. London: Blackwell Publishing, 2000:15-33. [http://dx.doi.org/10.1002/9780470760093] [ Links ]
4. Lacey CJ. Genital warts and anogenital papillomavirus disease. Medicine 2010;38(6):271-275. [http://dx.doi.org/10.1016/j.mpmed.2010.02.003] [ Links ]
5. Sun XW, Kuhn L, Ellerbrock TV, Chiasson MA, Bush TJ, Wright TC. Human papilloma virus infection in women infected with the human deficiency virus. N Engl J Med 1997;337(19):1343-1349. [http://dx.doi.org/10.1056/NEJM199711063371903] [ Links ]
6. Lacey CJ. Therapy for genital human papillomavirus-related disease. J Clin Virol 2005;32(Suppl.1):S82-S90. [http://dx.doi.org/10.1016/j.jcv.2004.10.020] [ Links ]
7. Vandepapeliere P, Barrasso R, Meijer CJ, et al. Randomised controlled trial of an adjuvanted human papillomavirus (HPV) type 6 L2E7 vaccine: Infection of external anogenital warts with multiple HPV types and failure of therapeutic vaccination. J Infect Dis 2005;192(12):2099-2107. [http://dx.doi.org/10.1086/498164] [ Links ]
8. Persson G, Dahlf LG, Krantz I. Physical and psychological effects of anogenital warts on female patients. Sex Transm Dis 1993;20(1):10-13. [http://dx.doi.org/10.1097/00007435-199301000-00003] [ Links ]
9. Wiley D, Masongsong E. Human papillomavirus: The burden of infection. Obstet Gynecol Surv 2006;61(Suppl 1):S3-S14. [http://dx.doi.org/10.1097/01.ogx.0000221010.82943.8c] [ Links ]
10. National Department of Health, South Africa. Clinical Guidelines on the Management of HIV and AIDS in Adults and Adolescents. 2010. http://www.sahivsoc.org/upload/documents/Clinical_Guidelines_for_the_Management_of_HIV_AIDS_in_Adults _Adolescents_2010.pdf (accessed 4 July 2015). [ Links ]
11. Onon TS. History of human papillomavirus, warts and cancer: What do we know today? Best Pract Res Clin Obstet Gynaecol 2011;25(5):565-574. [http://dx.doi.org/10.1016/j.bpobgyn.2011.05.001] [ Links ]
12. Von Grogh G. Management of anogenital warts (condyloma cuminata). Eur J Dermatol 2001;11(6):589-603. [ Links ]
13. Insinga RP, Dasbach EJ, Myers ER. The health and economic burden of genital warts in a set of private health plans in the United States. Clin Infect Dis 2003;36(11):1397-1403. [http://dx.doi.org/10.1086/375074] [ Links ]
14. Lacey CJN, Lowndes CM, Shah KV. Chapter 4: Burden and management of non-cancerous HPV- related conditions: HPV-6/11 disease. Vaccine 2006;24(Suppl 3):S35-S41. [http://dx.doi.org/10.1016/j.vaccine.2006.06.015] [ Links ]
15. Sun XW, Kuhn L, Ellerbrock TV, Chiasson MA, Bush TJ, Wright TC. Human papillomavirus infection in women infected with the human immunodeficiency virus. N Engl J Med 1997;337(19):1343-1349. [http://dx.doi.org/10.1056/NEJM199711063371903] [ Links ]
16. Lissouba P, van de Perre P, Auvert B. Association of genital human papillomavirus infection with HIV acquisition: A systemic review and meta-analysis. Sex Transm Infect 2013;89(5):350-356. [http://dx.doi.org/10.1136/sextrans-2011-050346] [ Links ]
17. Read TR, Hocking JS, Chen MY, Donovan B, Bardshaw CS, Fairley CK. The near disappearance of genital warts in young women 4 years after commencing a national human papillomavirus (HPV) vaccination programme. Sex Transm Infect 2011;87(7):544-547. [http://dx.doi.org/10.1136/sextrans-2011-050234] [ Links ]
18. Oliphant J, Perkins N. Impact of human papillomavirus (HPV) vaccine on genital warts diagnosed at Auckland Sexual Health Services. N Z Med J 2011;124(1339):51-58. [ Links ]
Accepted 15 June 2015
Corresponding author: S Tayib (syarq@yahoo.com)


{kind=link}