










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSAMJ: South African Medical Journal
versão On-line ISSN 2078-5135
versão impressa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.105 no.7 Pretoria Jul. 2015
EDITOR'S CHOICE
Janet Seggie
CME: Nutrition and malnutrition of young children
This issue of CME is dedicated to the nutrition, and malnutrition, of young children. This is an important topic in paediatric medicine and child health, because toddlers are at an age when they begin to feed independently and patterns of feeding for health in later life are set in motion. By the same token, malnutrition as a result of protein or energy deficiency or chronic illness is relatively common in this age group, even in our modern world.
The establishment of normal nutritional patterns in toddlers is precariously balanced between the legacy of infancy, genetic determinants, environmental inputs and social and cultural norms. Healthy nutrition is both physically and emotionally manipulated, and while disease is reflected in growth, it is equally revealed in micronutrient deficiency, intellectual dysfunction, immune disorders and behavioural pathology. A number of overt as well as subtle physical conditions are consequences of malnutrition. This issue focuses on obvious gross malnutrition as well as malnutrition from more subtle deficiencies and deficiencies associated with chronic illness.
Ultimately our goal is the improved health of the children of South Africa (SA) and potentially achievement of the Millennium Development Goals (MDGs) of improved child health in our country and on our continent.
Lung health in children
A number of articles in this issue of SAMJ deal with lung health in children, lower respiratory infections (LRTIs) ranking among the top five causes of mortality in children under the age of 4 years.
An article on the impact of highly active antiretroviral therapy (HAART) on the burden of bacterial LRTIs in children[1]deals with children presenting to primary care with symptoms of LRTIs. Echoing the May issue,[2] all were treated with amoxicillin with no complications. More significantly, HAART is proving effective in reducing the burden of LRTIs in children, even when the diagnosis of positive HIV status is delayed. Furthermore, immunisations against Streptococcus pneumoniae, Haemophilus influenzae and Varicella have proved safe and effective even in HIV-infected children, despite the fact that their primary immunological response is inferior and there is faster decay in immunological memory.
Children are particularly vulnerable when exposed to indoor and outdoor air pollution. A study undertaken in 2002 conservatively indicated that just over 1% of the burden of mortality in young children was a result of exposure to indoor air pollution. According to the 2011 census, around a quarter of SA households still use fuels other than electricity for daily cooking. Against this background, Albers et al.[3] of the Medical Research Council Environment and Health Research Unit in Johannesburg show in an article on household fuel use and child respiratory ill health in two Mpumalanga towns that the prevalence of respiratory illness is significantly greater among children whose homes use non-electrical fuels rather than electricity for cooking or heating.
Empyema is one of the commonest complications of pneumonia, the usual treatment of which requires antibiotics, adjusted according to clinical response and microbiological results, insertion of a chest tube to achieve drainage of the pus, and referral for surgery. Zampoli et al.,[4]in the first study describing the use of fibrinolytics in African children, describe the experience at Red Cross War Memorial Children's Hospital with intrapleural fibrinolytic therapy as first-line treatment in empyema. Tissue plasminogen activator (TPA) (Alteplase; Boehringer Ingelheim) was instilled into the pleura via the chest tube within 24 hours after its insertion. There was a four-fold reduction in requirement for surgical intervention and a trend towards shorter hospital stay and fewer chest drains in children receiving fibrinolytics: 18/47 (38%) children not treated with fibrinolytics required surgery compared with 5/52 (10%) of those treated with TPA.
Intracranial suppuration (ICS)
In an article reviewing an 8-year experience of ICS at Umtata General Hospital and Nelson Mandela Academic Hospital in the Eastern Cape Province, Anwary[5] describes the experience at the two hospitals and the changing epidemiology of ICS over the study period. While, as expected, sinusitis, ear infection and meningitis remain the major source of ICS, head trauma now accounts for 25 - 40% of cases, with a steady decline in cases related to ear infection and meningitis.
Maternal health
The April SAMJ dealt extensively with SA's failure to meet the MDG 5 maternal health goal - to reduce the maternal mortality rate by three-quarters and achieve universal access to reproductive health. In commemoration of Mother's Day (10 May 2015), Save the Children published its 16th annual State of the World's Mothers Report, 'with a special focus on our rapidly urbanising world and the poorest mothers and children who must struggle to survive despite overall urban progress'.[6] South Africa is ranked 72 of 179 countries (see table).
Dr Margaret Chan, Director-General, World Health Organization, observed in her foreword to the report that 'one of the worst places in the world to be a mother is in an urban slum. Poverty, and the social exclusion that goes with it, leave the urban poor trapped in overcrowded, makeshift or decrepit housing, with few opportunities to stay clean or safe on a daily basis. Diets are poor. Diseases are rife. Pregnancies occur too early in life and too often. Good health care, especially preventive care, is rare. In most cases, the publicly funded health services that reach the urban poor are under-staffed and ill-equipped. These are the women and children left behind by this century's spectacular socioeconomic advances. Far too often, even the simplest and most affordable health-promoting and lifesaving interventions - such as immunisations, vitamin supplements, safe drinking water, and prenatal check-ups - fail to reach them.'
Extending the MDG 5 maternal health theme, a population-based study of maternal near misses and maternal death in the Pretoria Academic Complex (PAC)[7]reveals that about one in 20 pregnant women admitted to the PAC, 40% of whom had presented with an acute emergency to a primary level facility and had to be transferred for tertiary care, had potentially life-threatening conditions. The emphasis must be on ensuring that all healthcare professionals involved in maternity care have the knowledge and skills to manage obstetric emergencies.
Healthcare delivery
Two Forum articles are key reading.
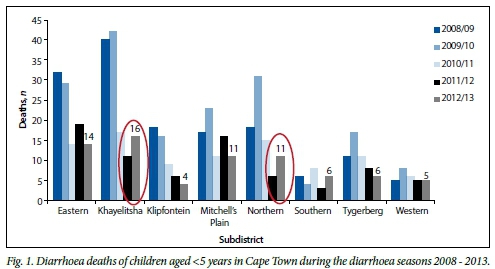
Colleagues from the Medical Research Council Burden of Disease Research Unit, City Health (City of Cape Town), the City of Cape Town Cape Metropole Health Information Group and the Department of Health, Provincial Government of the Western Cape, point to the importance of identified cause-of-death information being available for public health surveillance, actions and research.[8]A recent amendment to the SA Births and Deaths Registration Act has compromised efforts to strengthen local mortality surveillance to provide small-area statistics and information for public health actions. Diarrhoea deaths in children aged under 5 years during the diarrhoea season (November - May) were plotted to identify diarrhoea 'hot spots' and provide appropriate public health intervention at subdistrict level in the Cape Metropole. The results are evident in Fig. 1 in the article (see alongside).

The authors suggest that a practical solution to overcome the adverse impact of the recent change to the death notification form (DNF) would be for the National Department of Home Affairs to print all pages of the DNF in triplicate, with one copy to be sent to Statistics SA for statistical purposes, one copy to be sent to the health department in each province for public health action, such as that described above, and one copy to remain in the DNF as a paper trail for audit purposes.
In 'Social franchising primary healthcare clinics - a model for South African National Health Insurance?'[9]Robinson introduces the concept of social franchising, which emerged in the 1990s, and describes the North West provincial health department's social franchising initiative for PHC that is currently being piloted in Dr Kenneth Kaunda District. The project draws on SA's franchising industry, which has grown since 1945, operates through nearly 30 000 outlets, contributes 12% to the SA gross domestic product and provides stable employment to more than 500 000 people.
Genomics in medicine
Finally, the editorial by Urban[10] offers a lucid and comprehensive description of the rapidly advancing field of genomics, which is assuming an increasing role in patient care. Genomic medicine is expected to transition into the broader paradigm of precision medicine, with profound long-term implications for the practice of medicine and the training of future practitioners.
References
1. De Campos KR, Granga DD, Olorunju S. The impact of highly active antiretroviral therapy on the burden of bacterial lower respiratory tract infections in children. S Afr Med J 2015;105(7):554-557. [http://dx.doi.org/10.7196/SAMJnew.7820] [ Links ]
2. Lowman W Key to antimicrobial stewardship success: Surveillance by diagnostic microbiology laboratories. S Afr Med J 2015;105(5):359-360. [http://dx.doi.org/10.7196/SAMJ.9615] [ Links ]
3. Albers P, Wright CY, Voyi KVV, Mathee A. Household fuel use and child respiratory ill health in two towns in Mpumalanga, South Africa. S Afr Med J 2015;105(7):573-577. [http://dx.doi.org/10.7196/SAMJnew.7934] [ Links ]
4. Zampoli M, Kappos A, Verwey C, Mamathuba R, Zar HJ. Impact of fibrinolytics on the outcome of empyema in South African children. S Afr Med J 2015;105(7):549-553. [http://dx.doi.org/10.7196/SAMJnew.7796] [ Links ]
5. Anwary MA. Intracranial suppuration: Review of an 8-year experience at Umtata General Hospital and Nelson Mandela Academic Hospital, Eastern Cape, South Africa. S Afr Med J 2015;105(7):584-588. [http://dx.doi.org/10.7196/SAMJnew.7881] [ Links ]
6. The Urban Disadvantage. State of The World's Mothers 2015. http://www.savethechildren.org/atf/cf/j9def2ebe-10ae-432c-9bd0-df91d2eba74a|/SOWM_2015.PDF (accessed 13 May 2015). [ Links ]
7. Soma-Pillay P, Pattinson RC, Langa-Mlambo L, Nkosi BSS, Macdonald AP. Maternal near miss and maternal death in the Pretoria Academic Complex, South Africa - a population-based study. S Afr Med J 2015;105(7):578-583. [http://dx.doi.org/10.7196/SAMJnew.8038] [ Links ]
8. Groenewald P, Azevedo V, Daniels J, et al. The importance of identified cause-of-death information being available for public health surveillance, actions and research. S Afr Med J 2015;105(7):528-530. [http://dx.doi.org/10.7196/SAMJnew.8019] [ Links ]
9. Robinson AKL. Social franchising primary healthcare clinics - a model for South African National Health Insurance? S Afr Med J 2015;105(7):531-534. [http://dx.doi.org/10.7196/SAMJnew.7814] [ Links ]
10. Urban MF. Genomics in medicine: From promise to practice. S Afr Med J 2015;105(7):545-547. [http://dx.doi.org/10.7196/SAMJnew.7894] [ Links ]
This month in the SAMJ ...

Tamara Kredo* is a senior specialist scientist at the South African Medical Research Council and Deputy Director of Cochrane South Africa. She is a specialist in clinical pharmacology with an interest in evidence-informed healthcare, including clinical practice guideline development and implementation in resource-limited settings. Her research is focused on developing innovative partnerships to explore primary care guideline activities in South Africa. Her current work aims to expand capacity development initiatives for evidence synthesis in the African region, and dissemination of evidence to inform healthcare decision making. The upcoming Cochrane Corner marks the start of a new collaboration with the SAMJ to regularly bring relevant Cochrane reviews to the readership through brief bite-size summaries.
*Kredo T, Young T, Wiysonge CS, McCaul M, Volmink J. The Cochrane Corner in the SAMJ: Summaries of Cochrane systematic reviews for evidence-informed practice. S Afr Med J 2015;105(7):548. [http://dx.doi.org/10.7196/SAMJnew.8035]

Mushtaq Ahmad Anwary* qualified MBBS from the University of Mysore, India, and MMed (Radiology) from the University of Nairobi, Kenya. His main field of interest is ultrasonography and multi-detector computed tomography, and he currently heads the Clinical Unit in the Department of Radiology, Nelson Mandela Academic Hospital, Mthatha, Eastern Cape, and is a senior lecturer at Walter Sisulu University. He provides radiological services to the Transkei region as one of a team of two radiologists who have access to multi-detector CT, magnetic resonance imaging, digital fluoroscopy, digital mammography, colour Doppler ultrasonography and a picture archiving and communication system in a modern radiology department. A radiology registrar training programme has been set up in co-operation with University of Cape Town.
*Anwary MA. Intracranial suppuration: Review of an 8-year experience at Umtata General Hospital and Nelson Mandela Academic Hospital, Eastern Cape, South Africa. S Afr Med J 2015;105(7):584-588. [http://dx.doi.org/10.7196/SAMJnew.7881]

