










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.105 n.5 Pretoria May. 2015
http://dx.doi.org/10.7196/SAMJ.9603
CONTINUING MEDICAL EDUCATION
CASE REPORT
A lady with a broken heart: Apical ballooning syndrome
C RushI; M NtsekheII
IMB ChB; Department of Internal Medicine, Faculty of Health Sciences, University of Cape Town and Groote Schuur Hospital, Cape Town, South Africa
IIMD, PhD, FACC; Division of Cardiology, Department of Internal Medicine, Faculty of Health Sciences, University of Cape Town and Groote Schuur Hospital, Cape Town, South Africa
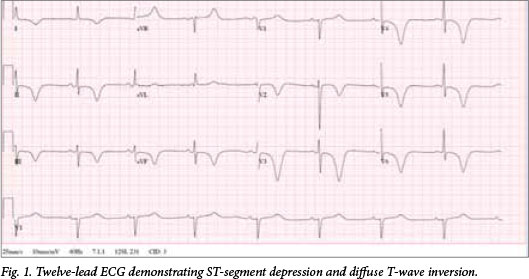
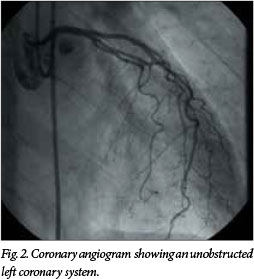
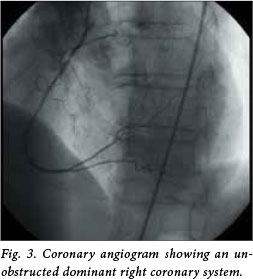
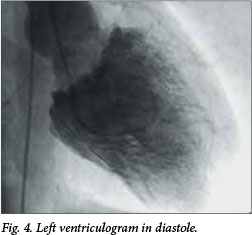
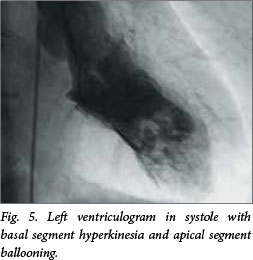
Severe chest pain after an emotional argument resulted in the admission of a healthy 72-year-old woman. She was haemodynamically compromised, with an electrocardiogram (ECG) demonstrating anterior ST-depression and T-wave inversions (Fig. 1). Her 6-hour troponin T level was 132 ng/L. Cardiac catheterisation revealed unobstructed coronary arteries and a reduced left ventricular ejection fraction (LVEF) of <35%, with basal hyperkinesia and apical segment ballooning (Figs 2 - 5). She was discharged home after 3 days of supportive therapy. At 3 months she was asymptomatic, with an equilibrium radionuclide angiography scan revealing a normal heart with an LVEF of 73%.
First described in Japan in 1990, apical ballooning syndrome accounts for 1 - 2% of suspected acute myocardial infarctions globally.[1,2] Often preceded by an emotional or physical stressor, the syndrome is characterised by transient left ventricle dysfunction and electrographic changes that mimic acute myocardial infarction with minimal release of myocardial enzymes in the absence of obstructive coronary artery disease.[3] Although 90% of all reported cases have been in postmenopausal women, it does occur across age and gender boundaries.[4] The exact pathophysiological basis of the disease still has to be demonstrated. Recognition of the syndrome is important because of its favourable natural history and the use of only supportive therapy.
References
1. Akashi YJ, Goldstein DS, Barbaro G, Takashi U. Takotsubo cardiomyopathy: A new form of acute, reversible heart failure. Circulation 2008;118:2754-2762. [http://dx.doi.org/10.1161/CIRCULATIONAHA.108.767012] [ Links ]
2. Prasad A, Lerman A, Rihal CS. Apical ballooning syndrome: A mimic of acute myocardial infarction. Am Heart J 2008;155:408-417. [http://dx.doi.org/10.1016/j.ahj.2007.11.008] [ Links ]
3. Gianni M, Dentali F, Grandi AM, Sumner G, Hiralal R, Lonn E. Apical ballooning syndrome or Takotsubo cardiomyopathy: A systematic review. Eur Heart J 2006;27:1523-1529. [ Links ]
4. Bybee KA, Prasad A, Barsness G, Wright RS, Rihal CS. Clinical characteristics, outcomes and impaired myocardial circulation in patients with transient left ventricular apical ballooning syndrome: A case series from a US medical center. Am J Cardiol 2004;94:343-346. [ Links ]
 Correspondence:
Correspondence:
C Rush
rshcol002@gmail.com

