










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.105 n.3 Pretoria Mar. 2015
http://dx.doi.org/10.7196/SAMJ.8731
RESEARCH
Hypertension, end-stage renal disease and mesangiocapillary glomerulonephritis in methamphetamine users
E S W JonesI; B L RaynerII
IMB BCh, PhD, FCP (SA), Cert Nephrol (SA); Department of Medicine, Faculty of Health Sciences, University of Cape Town, and Renal Unit, Groote Schuur Hospital, Cape Town, South Africa
IIMB ChB, FCP (SA), MMed, PhD; Department of Medicine, Faculty of Health Sciences, University of Cape Town, and Renal Unit, Groote Schuur Hospital, Cape Town, South Africa
ABSTRACT
BACKGROUND: Methamphetamine abuse has risen dramatically in South Africa. The chronic effects of abuse on the kidneys and blood pressure have not been documented. This study reviewed patients referred for evaluation of kidney disease and/or hypertension, who had been abusing methamphetamines.
METHODS: The records of patients referred to the renal unit between 2005 and 2013 who had been using methamphetamines were retrospectively reviewed. Patient demographics, biophysical parameters, blood pressure, renal function, renal ultrasound and biopsy findings, complications of chronic kidney disease and comorbidities were recorded.
RESULTS: Forty-seven patients were included in the study. Their mean age was 29 years. Hypertension was present in 42 (89.4%) of patients, with malignant hypertension in 21 (44.7%). Forty-five (95.7%) had chronic kidney disease (CKD), and 26 (55.3%) had end-stage renal disease. Renal biopsies were performed in 24 patients. Twelve (50.0%) of the biopsies showed hypertensive changes and 14 (58.3%) mesangiocapillary glomerulonephritis type 1, with deposition of IgM and C3 complement.
CONCLUSION: Methamphetamine use is associated with severe hypertension, mesangiocapillary glomerulonephritis and CKD.
South Africa (SA) is experiencing a dramatic rise in the use of methamphetamines, particularly in the Western Cape Province.[1] The drug is commonly used by young people of mixed ancestry,[2] and particularly those of lower socioeconomic status and educational level.[3] A closely related amphetamine, known as Ecstasy, was initially used as an appetite suppressant but rapidly became a recreational drug used in dancing clubs, where it was found to cause hyperthermia, dehydration and rhabdomyolysis, and an increased risk of acute renal failure.[4] Methamphetamine is relatively easy and inexpensive to produce, making it readily accessible.[5]
The use of amphetamines is associated with significant adverse physical effects. The toxic effects include cardiomyopathy,[6] ischaemic heart disease, aneurysm formation, seizures, psychosis, hallucinations, stroke,[7] hyperthermia, rhabdomyolysis, pulmonary hypertension, systemic hypertension, acute renal failure[8] and hepatocellular damage.[9] A review of the histopathological findings in drug users does not mention any renal effects in amphetamine users.[10] There have been isolated reports of adverse renal effects including necrotising renal vasculopathy,[8] an exaggerated decline in renal function over 15-year follow-up of patients who used methamphetamines,[11] an increased serum creatinine level 1 year after transplant in recipients of kidneys from donors who had used methamphetamines,[12] and early graft loss of two kidneys from donors who had used methamphetamines.[13]
In Africa there is even less information on the health outcomes of methamphetamine use. What literature there is addresses the dental, psychiatric and social impact of drug use in SA, particularly in the Western Cape.[14-16]
This study reviewed patients attending a single tertiary hospital with hypertension and/or chronic kidney disease (CKD) and who reported the use of methamphetamines.
Methods
Patients with a history of methamphetamine use who were referred to the Division of Nephrology and Hypertension at Groote Schuur Hospital, Cape Town, for evaluation were retrospectively studied from their medical records from 2005 to 2013. Patient demographics, biophysical parameters, blood pressure, renal function, renal ultrasound and biopsy findings, complications of CKD defined in terms of the Kidney Disease: Improving Global Outcomes guidelines,[17] and comorbidities were recorded.
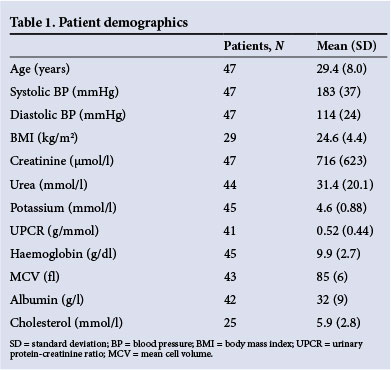
The estimated glomerular filtration rate was calculated using the Modification of Diet in Renal Disease formula (Table 1). Hypertensive retinopathy was graded 1 - 4 according to the presence of silver wiring, arteriovenous nipping, haemorrhages/exudates or papilloedema, respectively.[18] Malignant hypertension on fundoscopy was defined as grade 3 - 4 hypertensive retinopathy. Left ventricular hypertrophy (LVH) was defined by Sokolow-Lyon criteria of >35 mm.[19]
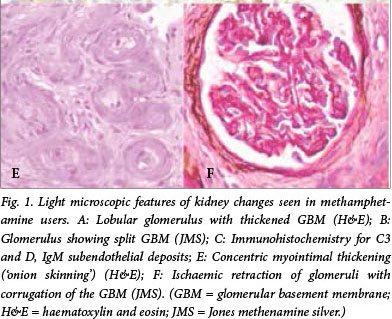
Renal biopsy was performed in patients with impaired renal function of unknown cause and/or proteinuria >3 g/d in the presence of normal-sized kidneys. Malignant hypertension on histology was defined as the presence of fibrinoid necrosis and onion-skinning of the arterioles associated with crenation of the glomerular basement membrane.
The study was approved by the University of Cape Town Research Ethics Committee (HREC REF: 573/2011).
Results
Forty-seven patients were identified, of whom 40 (85.1%) were male. Their mean (standard deviation (SD)) age was 29 (8) years. Table 1 shows the baseline demographics. Five patients (10.6%) were black Africans and the remainder (89.4%) of mixed ancestry. At the time of data collection, 11 patients had died, all of whom had end-stage renal disease (ESRD) at presentation and were not eligible for chronic dialysis in terms of the criteria for long-term dialysis and transplantation in the Western Cape;[20] all died as a consequence of chronic renal failure.
At presentation, 42 (89.4%) of the patients were hypertensive, with evidence of malignant hypertension (defined by grade 3 or 4 hypertensive retinopathy and/or evidence on renal biopsy) in 21 (44.7%). The mean (SD) blood pressure was 183 (37)/114 (24) mmHg. Significant target organ damage (TOD) as a result of hypertension was evident in 34 patients (72.3%). Of the 37 patients (78.7%) who had documentation of electrocardiographic findings, LVH was found in 26 (70.3%). Findings on fundoscopy were recorded in 26 patients (55.3%): stage 1 hypertensive retinopathy was seen in 2 (7.7%) patients, stage 2 in 5 (19.2%), stage 3 in 11 (42.3%) and stage 4 in 7 (26.9%). CKD was found in 45 patients (95.7%). On ultrasound, 24 patients (51.1%) had evidence of CKD (i.e. small kidneys in 10, loss of corticomedullary differentiation in 4, increased echogenicity in 19). The mean (SD) urine protein-creatinine ratio was 0.52 (0.44) g/mmol. Twenty-six patients (55.3%) had stage 5 CKD, 4 (8.5%) stage 4, 4 (8.5%) stage 3, 5 (10.6%) stage 2, and 6 (12.8%) stage 1; only 2 (4.3%) had no evidence of CKD.
Renal biopsy was performed in 24 patients (51.1%). Hypertensive changes were found in 12 biopsies (50.0%) with 6 (25.0%) showing malignant changes (Fig. 1, E and F). Six (25.0%) showed ESRD. Mesangiocapillary glomerulonephritis (MCGN) type 1 was found in 14 biopsy cases (58.3%) (Fig. 1, A and B), all of which were positive for IgM and C3 complement (Fig. 1, C and D). In addition, 9 (37.5%) showed staining for IgG and 7 (29%) for IgA.


One individual (2.1%) tested positive for HIV, and 2 (4.3%) for syphilis. The HIV-positive patient underwent renal biopsy, the histological findings showing hypertensive changes only. No patients were positive for hepatitis B or C, or had infective endocarditis or systemic lupus erythematosus.
All the patients in this study had been using methamphetamines, but in only a few cases was the length of drug use documented. Some patients used other recreational drugs, methaqualone in 10 cases (21.3%) and cocaine in 3 (6.4%); no patient used intravenous drugs. All three patients using cocaine had malignant hypertension and ESRD. Two of these patients underwent renal biopsy, which showed hypertensive changes and ESKD in both cases, but no evidence of MCGN. Of the patients who had used methaqualone, 7 underwent renal biopsies; 6 had hypertensive changes and 5 had MCGN.
Discussion
This study investigated the association between hypertension and/ or CKD and methamphetamine use in patients referred to a single large tertiary hospital in Cape Town for evaluation of CKD and/or hypertension between 2005 and 2013. The major findings were the presence of severe hypertension, with 44.7% of cases complicated by malignant hypertension; CKD (stage 4 or 5 in 64%) was present in in 95.7%. The unexpected and novel finding was the presence of MCGN in 58.3% of the 24 biopsies performed.
The association of methamphetamine use with hypertension is not unexpected, as the drug has vasoconstrictive properties causing increased systemic vascular resistance and raised blood pressure. However, the severity of the hypertension is remarkable. The mean (SD) blood pressure was 183 (37)/114 (24) mmHg, and 44.7% had malignant hypertension. TOD was commonly seen: 70.3% had LVH and 96.2% hypertensive retinopathy. On renal biopsy of hypertensive methamphetamine users, there were vascular changes of hypertension in 12 with evidence of malignant hypertension in 6.
The prevalence of CKD in this group of patients was 95.7%, with 63.8% of patients having very severe disease (CKD stages 4 and 5). In the cohort, 41 cases of CKD were related to hypertension on clinical grounds, and this was confirmed by renal biopsy in 12 cases. The unexpected finding in this study was that not all cases of CKD were a consequence of hypertension. MCGN was found to be the cause in 14 cases (58.3% of biopsies and 29.7% of the entire group). Idiopathic MCGN is the most common biopsy finding in Cape Town[21] and in other areas of SA the second most common,[22] although it is declining in incidence in developed countries.[23]
Known associations with MCGN did not explain the link between methamphetamine use and MCGN. All the biopsies that showed MCGN had IgM and C3 deposits, supporting chronic antigenaemia as a possible cause. Hepatitis C virus, hepatitis B virus, HIV, malaria and infective endocarditis are common infectious agents associated with MCGN, but these were excluded on clinical and serological grounds in all except one patient, who was HIV-positive. This patient had hypertensive changes on renal biopsy without evidence of MCGN. The two patients who tested positive for syphilis did not undergo renal biopsy.
MCGN is thought to result from chronic antigenaemia with defects in elimination or clearing of foreign antigen.[24] It is possible that people who use methamphetamines are exposed to multiple infectious antigens through the sharing of drugs and devices to inhale the drug. Another possible means of exposure to infectious antigens is through close physical contact between people during the process of taking the drug. It is also possible that methamphetamines alter self-proteins, making them immunogenic or creating haptens. However, these explanations are highly speculative.
On renal biopsy, MCGN and hypertension were fairly equally represented (14 and 12 cases, respectively). MCGN has a poor prognosis, with 50% of patients progressing to ESRD within 5 years.[24] Severe hypertension (affecting 37 patients (78.7%)) also results in ESRD. Seven patients (14.9%) had isolated hypertension without ESRD. This suggests that there are at least two pathways to ESRD for patients using methamphetamines.
MCGN has been associated with intravenous drug use, especially of heroin.[25] However, it is unlikely that intravenous drug use was relevant in this group of patients; no such drug use was reported, and no patient was hepatitis B- or C-positive. Only one patient was found to be HIV-positive. The prevalence of HIV in the mixed-ancestry community it is ~5.5 - 6.6%[26] and in SA overall ~8.5%,[27] considerably higher figures than in this study. Similarly, hepatitis B prevalence is high in SA (~8%).[28]
Study limitations
The limitations of this study are that it is purely observational of the presence of hypertension, MCGN and ESRD in patients using methamphetamines. In addition, there is no clear pathophysiological pathway linking methamphetamine abuse to MCGN. Further studies, while difficult in the setting of illicit substances, are clearly required.
Conclusion
The abuse of methamphetamines appears to be associated with severe hypertension and MCGN, both of which can lead to ESRD and death. In a resource-limited setting, this has important implications for the management of these young patients. Strategies to prevent exposure to this easily accessible drug need to be implemented.
Acknowledgements. This research was initiated by Dr Nazier Khan, who tragically died before he could complete the project.
References
1. Peltzer K, Ramlagan S, Johnson BD, Phaswana-Mafuya N. Illicit drug use and treatment in South Africa: A review. Subst Use Misuse 2011;45(13):2221-2243. [http://dx.doi.org/10.3109/10826084.2010.481594] [ Links ]
2. Matsha TE, Yako YY, Rensburg MA, Hassan MS, Kengne AP, Erasmus RT. Chronic kidney diseases in mixed ancestry South African populations: Prevalence, determinants and concordance between kidney function estimators. BMC Nephrol 2013;14(1):75-84. [http://dx.doi.org/10.1186/1471-2369-14-75] [ Links ]
3. Pluddemann A, Flisher AJ, McKetin R, Parry C, Lombard CJ. Methamphetamine use, aggressive behavior and other mental health issues among high school students in Cape Town, South Africa. Drug Alcohol Depend 2010;109(1-3):14-19. [http://dx.doi.org/10.1016/j.drugalcdep.2009.11.021] [ Links ]
4. Fahal IH, Sallomi DF, Yaqoob M, Bell GM. Acute renal failure after ecstasy. BMJ 1992;305(6844):29. [http://dx.doi.org/10.1136/bmj.305.6844.29] [ Links ]
5. Pluddemann A, Myers B, Parry C. Fact sheet - Methamphetamine. Cape Town: Medical Research Council, 2007:1-3. [ Links ]
6. Ito H, Yeo K-K, Wijetunga M, Seto TB, Tay K, Schatz IJ. A comparison of echocardiography findings in young adults with cardiomyopathy: With and without a history of methamphetamine abuse. Clin Cardiol 2009;32(6):E18-E22. [http://dx.doi.org/10.1002/clc.20367] [ Links ]
7. Ances BM, Vaida F, Cherner M, et al. HIV and chronic methamphetamine dependence affect cerebral blood flow. J Neuroimmune Pharmacol 2011;6(3):409-419. [http://dx.doi.org/10.1007/s11481-011-9270-y] [ Links ]
8. Bingham C, Beaman M, Nicholls AJ, Anthony PP. Necrotizing renal vasculopathy resulting in chronic renal failure after ingestion of methamphetamine and 3,4-methylenedioxymethamphetamine ('ecstasy'). Nephrol Dial Transplant 1998;13(10):2654-2655. [http://dx.doi.org/10.1093/ndt/13.10.2654] [ Links ]
9. Albertson TE, Derlet RW, van Hoozen BE. Methamphetamine and the expanding complications of amphetamines. West J Med 1999;170(4):214-219. [ Links ]
10. Milroy CM, Parai JL. The histopathology of drugs of abuse. Histopathology 2011;59(4):579-593. [http://dx.doi.org/10.1111/j.1365-2559.2010.03728.x] [ Links ]
11. Vupputuri S, Batuman V, Muntner P, et al. The risk for mild kidney function decline associated with illicit drug use among hypertensive men. Am J Kidney Dis 2004;43(4):629-635. [http://dx.doi.org/10.1053/j.ajkd.2003.12.027] [ Links ]
12. Inouye DS, Kickertz K, Wong LL. Methamphetamine use in deceased kidney donors impairs one-yr graft function. Clin Transplant 2007;21(5):643-650. [http://dx.doi.org/10.1111/j.1399-0012.2007.00703.x] [ Links ]
13. De Ligny BH, El Haggan W, Comoz F, et al. Early loss of two renal grafts obtained from the same donor: Role of ecstasy? Transplantation 2005;80(1):153-156. [http://dx.doi.org/10.1097/01.TP.0000158713.70266.06] [ Links ]
14. Meade CS, Watt MH, Sikkema KJ, et al. Methamphetamine use is associated with childhood sexual abuse and HIV sexual risk behaviors among patrons of alcohol-serving venues in Cape Town, South Africa. Drug Alcohol Depend 2012;126(1-2):232-239. [http://dx.doi.org/10.1016/j.drugalcdep.2012.05.024] [ Links ]
15. Wechsberg WM, Luseno WK, Karg RS, et al. Alcohol, cannabis, and methamphetamine use and other risk behaviours among black and coloured South African women: A small randomized trial in the Western Cape. Int J Drug Policy 2008;19(2):130-139. [http://dx.doi.org/10.1016/j.drugpo.2007.11.018] [ Links ]
16. Jones HE, Browne FA, Myers BJ, et al. Pregnant and nonpregnant women in Cape Town, South Africa: Drug use, sexual behavior, and the need for comprehensive services. Int J Pediatr 2011;2011:353410. [http://dx.doi.org/10.1155/2011/353410] [ Links ]
17. Stevens PE, Levin A. Clinical guidelines. Evaluation and management of chronic kidney disease: Synopsis of the Kidney Disease: Improving Global Outcomes 2012 Clinical Practice Guideline. Ann Intern Med 2013;158(11):825-831. [http://dx.doi.org/10.7326/0003-4819-158-11-201306040-00007] [ Links ]
18. Talley NJ, O'Connor S. Clinical Examination. 3rd ed. Talley NJ, O'Connor S, eds. Eastgardens, NSW, Australia: Blackwell Science, 1996. [ Links ]
19. Romhilt DW, Bove KE, Norris RJ, et al. A critical appraisal of the electrocardiographic criteria for the diagnosis of left ventricular hypertrophy. Circulation 1969;40(2):185-195. [http://dx.doi.org/10.1161/01.CIR.40.2.185] [ Links ]
20. Swanepoel CR, Wearne N, Duffield MS, Okpechi IG. The evolution of our knowledge of HIV-associated kidney disease in Africa. Am J Kidney Dis 2012;60(4):668-678. [http://dx.doi.org/10.1053/j.ajkd.2012.04.034] [ Links ]
21. Okpechi I, Swanepoel C, Duffield M, et al. Patterns of renal disease in Cape Town South Africa: A 10-year review of a single-centre renal biopsy database. Nephrol Dial Transplant 2011;26(6):1853-1861. [http://dx.doi.org/10.1093/ndt/gfq655] [ Links ]
22. Van Rensburg BWJ, van Staden AM, Rossouw GJ, Joubert G. The profile of adult nephrology patients admitted to the renal unit of the Universitas Tertiary Hospital in Bloemfontein, South Africa from 1997 to 2006. Nephrol Dial Transplant 2010;25(3):820-824. [http://dx.doi.org/10.1093/ndt/gfp535] [ Links ]
23. Simon P, Ramée MP, Autuly V, et al. Epidemiology of primary glomerular diseases in a French region. Variations according to period and age. Kidney Int 1994;46(4):1192-1198. [http://dx.doi.org/10.1038/ki.1994.384] [ Links ]
24. Floege J, Johnson RJ, Feehally J. Section IV: Glomerular disease. In: Floege J, Johnson RJ, Feehally J, eds. Comprehensive Clinical Nephrology. 4th ed St Louis: Elsevier Saunders, 2010:193-358. [http://dx.doi.org/10.1016/B978-0-323-05876-6.00015-0] [ Links ]
25. Jaffe JA, Kimmel PL. Chronic nephropathies of cocaine and heroin abuse: A critical review. Clin J Am Soc Nephrol 2006;1(4):655-667. [http://dx.doi.org/10.2215/CJN.00300106] [ Links ]
26. Connolly C, Shisana O, Colvin M, Stoker D. Epidemiology of HIV in South Africa - results of a national, community-based survey. S Afr Med J 2004;94(9):776-781. [ Links ]
27. Lehohla P. Mid-Year Population Estimates 2013. Pretoria: Statistics South Africa, 2013:1-17. [ Links ]
28. Kew MC. Epidemiology of chronic hepatitis B virus infection, hepatocellular carcinoma, and hepatitis B virus-induced hepatocellular carcinoma. Pathol Biol 2010;58(4):273-237. [http://dx.doi.org/10.1016/j.patbio.2010.01.005] [ Links ]
 Correspondence:
Correspondence:
E S W Jones
eswjones@gmail.com
Accepted 13 October 2014.

