










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSAMJ: South African Medical Journal
versión On-line ISSN 2078-5135
versión impresa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.105 no.4 Pretoria abr. 2015
http://dx.doi.org/10.7196/SAMJ.9108
RESEARCH
Pathological findings in reduction mammoplasty specimens: A South African perspective
C SofianosI; R J ZinnII; D A GeoffreysIII; D KrugerIV
IMB BCh, MRCS (Eng); Department of Surgery, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IIMB ChB, FC Plast Surg (SA), MMed; Department of Surgery, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IIIMB ChB, FC Plast Surg (SA); Department of Surgery, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IVBSc, PGCHE, PhD; Department of Surgery, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
ABSTRACT
BACKGROUND: Preoperative, intraoperative and follow-up guidelines for managing occult carcinoma in reduction mammoplasty specimens are scant
METHODS: We retrospectively analysed the records and pathology reports of 200 patients who had undergone reduction mammoplasty at two major public hospitals in Johannesburg, South Africa, during 2009 - 2014. Demographic data, their history of breast cancer and preoperative screening, the surgical techniques used and pathological reports were included. In all cases preoperative screening for breast cancer had been negative
RESULTS: All the patients were female, mean age 37.1 years, range 20 - 84 (standard deviation 11.9). All reductions were performed using standard techniques. Benign pathology was observed in 98 patients (49%) and malignant pathology in four (2%). The most common benign pathology observed was fibrocystic disease, and the most common malignant pathology ductal carcinoma in situ. Patient age correlated significantly with benign or malignant disease
CONCLUSIONS: Reduction mammoplasty produces tissue that should always be sent for pathological assessment. Patients should be stratified by risk, as doing so helps in selecting both the surgical setting and the approach to pathological analysis of the specimen. While the incidence of occult carcinoma in reduction mammoplasty specimens is low, all patients undergoing the procedure should be informed that tissue will be sent for pathological examination, allowing them to prepare to receive possible news of breast cancer and be adequately equipped for subsequent decision-making
Breast reduction (reduction mammoplasty) is frequently performed by plastic and breast surgeons to relieve macromastia symptoms.[1] In the USA, a 97% increase in the number of reduction mammoplasty procedures has been observed.[2] The procedure increases both physical and psychological wellbeing and improves quality of life for many patients.[3]
Crikelair and Malton[4] published the first reported case of occult carcinoma discovered during reduction mammoplasty in 1959. They described the presence of ductal carcinoma seen on microscopic examination of surgical specimens. Interestingly, they then published an addendum to their initial report when the patient developed another primary tumour in the other breast. Since then, as detailed below, many studies have attempted to investigate the incidence of occult carcinoma in reduction mammoplasty specimens.
Snyderman and Lizardo[5] performed a landmark study investigating the presence of occult carcinoma in reduction mammoplasty specimens. They examined 5 008 cases and demonstrated an incidence of 0.38%. In 1997, Jansen et al.[6] found an incidence of 0.16% in their series of 2 576 patients; however, the study design made use of a postal questionnaire sent out to consultant plastic surgeons, so it was susceptible to sampling bias. A population-based series study in Ontario, Canada, found a significantly lower incidence (0.06%) of breast cancer at the time of reduction mammoplasty.[7] While older studies such as this are possibly outdated, given the improved awareness of breast malignancy and enhanced clinical and radiological techniques used in its detection, in the above series, patients diagnosed with breast cancer at the time of reduction mammoplasty were less likely to have advanced cancer than the general population and had a better 5-year survival rate. Preoperative screening featured both a clinical breast examination and mammography.[7]
In South Africa (SA), from which our data are drawn, the latest available statistics from the SA National Cancer Registry are from 2006 and show that the incidence of breast cancer in SA is 0.029%.[8]
Macromastia is in itself a factor predisposing to breast cancer.[9] The increased prevalence of carcinoma of the breast in these women suggests that they may ultimately develop breast cancer following breast reduction.[10] Surgeons should be mindful of this fact, and undertake preoperative screening.[11] If a lesion is detected, the recommended triple breast evaluation steps outlined in Table 1 must be followed.
Diagnosis of breast cancer prior to reduction mammoplasty is vital, as management and treatment options may change significantly.[12] A woman would be unlikely to opt to proceed with reduction mammoplasty without having both a biopsy and a multidisciplinary team decision on the management of malignancy. The diagnosis of breast cancer during reduction mammoplasty reduces the number of appropriate surgical options available and also complicates further treatment of the cancer.[2]
Methods
The worldwide incidence of occult carcinoma in reduction mammoplasty specimens is low. No study examining these pathological findings has been performed in SA. As discussed, studies have been conducted in developed countries, but this information may not be accurately extrapolated to developing countries such as SA.
Study area
Chris Hani Baragwanath Academic Hospital (CHBAH) is a public hospital situated in Soweto, Johannesburg, South Africa. It serves a mostly black African, lower-income population of 2.5 million. Mammoplasty procedures are performed at CHBAH free of charge to the patient. Helen Joseph Hospital (HJH) is a public hospital situated in Westdene, Johannesburg, and serves a population of approximately 198 000 of mixed socioeconomic status. Mammoplasty procedures are not provided free of charge at HJH, but the cost is lower than that at a private hospital.
Study design
A retrospective record review was performed of all patients who had undergone reduction mammoplasty procedures at CHBAH or HJH between January 2009 and January 2014, inclusive. Along with demographic data, patient histories of breast cancer, findings on preoperative screening, surgical techniques and pathological reports were recorded.
Inclusion criteria
To be included in the study sample, each patient had to meet the following three inclusion criteria: no preoperative history or examination suggestive of any breast disease; reduction mammoplasty performed on one or both breasts, using standard surgical techniques; and surgical specimens submitted for pathological review.
Preoperative screening
A detailed history was obtained, and aimed to identify previous or current breast disease and personal or family risk factors for breast disease. Screening further included clinical examination of the breasts as well as imaging - specifically, breast ultrasound for patients <35 years of age, and mammography for those aged >35 years. Preoperative imaging not only enabled significant breast disorders to be identified before surgery, but provided a control for detection of abnormalities after surgery had been performed.[13]
Pathological assessment
Pathological findings were categorised into two broad groups: benign lesions and malignant lesions. Fibrocystic disease was included under benign pathology. Malignant pathology included carcinoma in situ. Only cases with at least two random blocks per breast were included. All specimens had been submitted to the SA National Health Laboratory Service.
Statistical analysis
The Statistical Package for the Social Sciences (SPSS) 20.0 (SPSS Inc., USA) software program for Macintosh was used in data analysis. Descriptive results were expressed as means and standard deviations (SDs). Statistical evaluations were performed using the non-parametric Mann-Whitney (7-test. The level of significance was set at p<0.05.
Ethical approval
Ethical approval was obtained from the Human Research Ethics Committee of the University of the Witwatersrand (clearance No. M140239).
Results
A total of 209 patients were identified for inclusion in the study. Nine were excluded because their operative specimens had not been submitted for pathological analysis. The 200 patients included were all female, with a mean (SD) age of 37.1 (11.9) years. The youngest patient was 20 years of age, and the oldest 84. All patients had undergone a preoperative work-up including history-taking, clinical examination and imaging. All reductions were performed using standard techniques, with 195 procedures being bilateral and five unilateral. The mean (SD) weight of specimens submitted for pathological review was 1 002.8 (652.1) g.
Benign pathology was observed in 98/200 patients (49%) and malignant pathology in four (2%). Specific pathological findings are listed in Table 2. Benign pathology was observed at a mean age of 46.5 years and malignant pathology at a mean of 50.2 years.

The Shapiro-Wilk test of normality revealed that the age and average specimen weight variables were not normally distributed. A Mann-Whitney U-test showed that age was a variable significantly associated with the presence of both benign disease (p<0.0001) and malignant disease (p=0.012). No significant difference was found when the presence of benign or malignant disease was correlated with specimen weight. Furthermore, there was no significant difference when specific malignant lesions were compared, probably owing to the small sample number.
Discussion
Reduction mammoplasty produces a variable amount of tissue that should always be sent for pathological examination.[14] The procedure is of both cosmetic and oncological significance.[15] Its oncological significance is based primarily on the observation that breast cancer risk is reduced proportionate to the amount of breast tissue removed during the procedure.[16] Additionally, breast cancer encountered before, during, or after reduction mammoplasty requires a multidisciplinary approach to treatment, like any other breast cancer.
Malignant pathology was observed in 2% (n=4) of the 200 patients in this study. The incidence of occult breast carcinoma in other series ranges from 0.06% to 4.6%, with the most recent study in 2013 reporting a 0.56% rate of malignant pathology (including both invasive carcinoma and carcinoma in situ).[17]Differences in incidence arise because some studies include patients with previous or current breast disease, while in others, carcinoma in situ was not included. In addition, the pick-up of abnormal pathology increases in proportion to the degree of the pathological analysis.[18] In 1984, Nielsen et al.[19] showed through intensive pathological scrutiny of breast specimens obtained from autopsy (200 or more blocks per specimen) that 14 -16% of these specimens had occult carcinoma or carcinoma in situ. A future direction for our study would be a prospective investigation including a higher number of blocks per specimen to increase the rate of pick-up of pathological lesions.
Freedman et al.[20]found that the incidence of both premalignant and malignant lesions increased with increasing patient age; this trend was also seen in the current study, the significance extending to benign lesions as well as premalignant and malignant lesions. The malignant conditions encountered were largely (75%) of the ductal carcinoma in situ variety. The most common benign lesion encountered was fibrocystic change, followed by sclerosing adenosis. We found fibroadenoma, classically a condition encountered in younger individuals, to be more common among older patients. The weight of the specimen was not found to influence the presence of benign or malignant disease.
Patients who undergo reduction mammoplasty at CHBAH or HJH are followed up at 6 and 12 months. They are given advice regarding further screening, and are also followed up as part of SA's standard breast cancer screening programmes. Long-term follow-up of these patients would be of value to ascertain the incidence of breast cancer in the remaining breast tissue. Furthermore, in countries with a high prevalence of HIV/AIDS, variables such as HIV positivity and CD4 count would be useful data to capture and examine in future research. These data were not available for our retrospective review, but could be included in future prospective studies.
Every patient in the current study had had preoperative screening, despite the scant availability of universal guidelines for preoperative assessment and pathological assessment.
All methods of breast reduction allow for good exposure of breast parenchyma, and for direct visualisation and palpation of other segments; theoretically, any palpable tumour therefore can and should be detected at that time.[1] Titley et al.[21] suggested in 1996 that surgical specimens be separated clearly into left and right, and that a marker stitch be placed in the main specimen, possibly separating tissues into quadrants. Since the majority of reduction mammoplasty specimens do not have occult carcinoma, it would be difficult to convince all surgeons to ink the margins of surgical specimens; however, it is reasonable to insist that specimens from women at an increased risk of developing breast cancer be inked for orientation.[2]
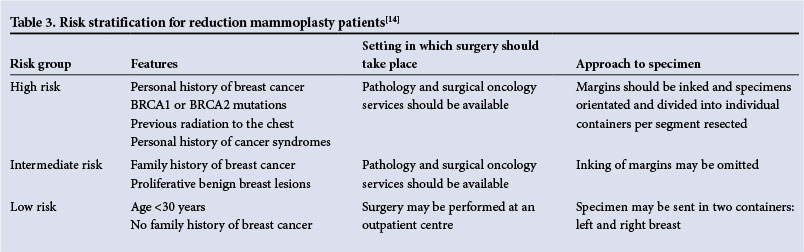
More recently it has been suggested that patients undergoing reduction mammoplasty be stratified according to risk; doing so would dictate the setting in which surgery should take place and the approach to pathological analysis of the specimen.[15] Table 3 outlines the approach to risk stratification and in what settings surgery should be done.
Patients diagnosed with breast cancer at the time of reduct ion mammoplasty are likely to be treated with a completion mastec-tomy.[7] The basis of this decision is the rearrangement of tissue during the procedure, as well as the possibility of tumour seeding in the normal breast. Discovery of a breast carcinoma during or after a reduction mammoplasty poses a number of technical challenges: a large field of dissection, including a breach of pectoral fascia in certain areas; a larger skin incision; and possible contamination of the other breast during bilateral procedures.[12] The suggested technique, if breast cancer is discovered in pathological examination of surgical specimens from reduction mammoplasty, is a completion mastectomy that includes pre-existing incisions from the reduction mammoplasty procedure.[22] Reduction mammoplasty should not be considered a contraindication to sentinel lymph node biopsy, as many lymphatic channels remain intact and most breast reduction techniques involve incisions on the inferior aspect of the breast.[23]
Many philosophical debates on ethics and informed consent have arisen in recent years. In the UK, screening for breast cancer is not recommended for any woman under the age of 50.[24] Furthermore, the US Preventive Services Task Force's breast screening recommendations recently indicated that mammography is of no benefit for patients under the age of 50.[25] Given these recommendations, many young women worldwide who are undergoing reduction mammoplasty are in effect undergoing a 'screening procedure' without their informed consent.[26] Although the incidence of occult carcinoma among reduction mammoplasty specimens is low, all patients undergoing the procedure should be fully informed that the tissue will be sent for pathological examination, as doing so allows them to prepare for the possibility of receiving news of breast cancer, and to be adequately equipped for the decision-making that will follow.[26] Indeed, 'The primary intent of mammoplasty is cosmetic, but it is a medical procedure, taking place in a medical setting, and those performing it have a fiduciary obligation towards their patients' health and wellbeing.'[26]
Conclusion
It has been demonstrated that, even in developing countries, it is of vital importance that surgeons aim to adequately investigate reduction mammoplasty candidates preoperatively and ensure that all tissue is submitted for pathological analysis. During the informed consent process for the procedure, patients should be fully informed of the potential consequences of the pathological analysis of surgical specimens obtained. Multidisciplinary approaches to breast cancer treatment should always be included for patients undergoing reduction mammoplasty who are diagnosed with breast cancer. Age was found to correlate significantly with the presence of benign or malignant disease in reduction mammoplasty specimens. Further areas of study exist, and the results thereof could increase our understanding of the various pathological lesions found in reduction mammoplasty specimens.
References
1. Viana GA, Pitanguy I, Torres E. Histopathological findings in surgical specimens obtained from reduction mammaplasties. Breast 2005;14(3):242-248. [http://dx.doi.org/10.1016/j.breast.2004.12.006] [ Links ]
2. Keleher AJ, Langstein HN, Ames FC, et al. Breast cancer in reduction mammaplasty specimens: Case reports and guidelines. Breast J 2003;9(2):120-125. [http://dx.doi.org/10.1046/j.1524-4741.2003.09216.x] [ Links ]
3. Goyal A, Coulson SG, Wu JM, et al. Occult breast carcinoma in breast reduction specimens in European women. Breast Cancer Res Treat 2011;128(3):749-753. [http://dx.doi.org/10.1007/s10549-011-1589-9] [ Links ]
4. Crikelair GF, Malton SD. Mammaplasty and occult breast malignancy: Case report. Plast Reconstr Surg Transplant Bull 1959;23(6):601-606. [http://dx.doi.org/10.1097/00006534-195906000-000061] [ Links ]
5. Snyderman RK, Lizardo JG. Statistical study of malignancies found before, during, or after routine breast plastic operations. Plast Reconstr Surg Transplant Bull 1960;25(3):253-256. [http://dx.doi.org/10.1097/00006534-196003000-000061] [ Links ]
6. Jansen DA, Murphy M, Kind GM, et al. Breast cancer in reduction mammoplasty: Case reports and a survey of plastic surgeons. Plast Reconstr Surg 1998;101(2):361-364. [http://dx.doi.org/10.1097/00006534-199802000-000141] [ Links ]
7. Tang CL, Brown MH, Levine R, et al. Breast cancer found at the time of breast reduction. Plast Reconstr Surg 1999;103(6):1682-1686. [http://dx.doi.org/10.1097/00006534-199905000-000161] [ Links ]
8. National Health Laboratory Service. National Cancer Registry of South Africa. http://www.nioh.ac.za/assets/files/NCR_2006_TABLES_FINAL.pdf (accessed 29 April 2014). [ Links ]
9. Dotto J, Kluk M, Geramizadeh B, et al. Frequency of clinically occult intraepithelial and invasive neoplasia in reduction mammoplasty specimens: A study of 516 cases. Int J Surg Pathol 2008;16(1):25- 30. [http://dx.doi.org/10.1177/10668969073071761] [ Links ]
10. Rees TD, Coburn R. Breast reduction: Is it an aid to cancer detection? Br J Plast Surg 1972;25(2):144- 146. [http://dx.doi.org/10.1016/S0007-1226(72)80036-51] [ Links ]
11. Van der Torre PM, Butzelaar RM. Breast cancer and reduction mammoplasty: The role of routine pre-operative mammography. Eur J Surg Oncol 1997;23(4):341-342. [http://dx.doi.org/10.1016/S0748-7983(97)90885-41] [ Links ]
12. Gottlieb JR, McKinney P, Walkinshaw MD, et al. Occult breast carcinoma in patients undergoing reduction mammaplasty. Aesthetic Plast Surg 1989;13(4):279-283. [http://dx.doi.org/10.1007/BF015703611] [ Links ]
13. Shiffiman MA. Mammograms in cosmetic breast surgery. In: Shiftman MA, ed. Mastopexy and Breast Reduction: Principles and Practice. 1st ed. Heidelberg: Springer, 2009:37-40. [ Links ]
14. Ishag MT, Bashinsky DY, Beliaeva IV, et al. Pathologic findings in reduction mammaplasty specimens. Am J Clin Pathol 2003;120(3):377-380. [http://dx.doi.org/10.1309/4KD652HN739XTLM3] [ Links ]
15. Jansen DA, Ghere MC, Lee M, et al. Breast cancer and reduction mammaplasty. In: Shiftman MA, ed. Mastopexy and Breast Reduction: Principles and Practice. 1st ed. Heidelberg: Springer, 2009:657-670. [ Links ]
16. Brinton LA, Persson I, Boice JD jr, et al. Breast cancer risk in relation to amount of tissue removed during breast reduction operations in Sweden. Cancer 2001;91(3):478-483. [http://dx.doi.org/10.1002/1097-0142(20010201)91:3%3C478::AID-CNCR1025%3E3.3.CO;2-X] [ Links ]
17. Aytac B, Sahsine T, Erturk FY, et al. Evaluation of incidence and histolopathological findings of breast lesions in reduction mammoplasty specimens: Uludag University experience. J Pak Med Assoc 2013;63(7):878-881. [ Links ]
18. Kerrigan CL, Slezak SS. Evidence-based medicine: Reduction mammaplasty. Plast Reconstr Surg 2013;132(6):1670-1683. [http://dx.doi.org/10.1097/PRS.0b013e3182a807ec] [ Links ]
19. Nielsen M, Jensen J, Andersen J. Precancerous and cancerous breast lesions during lifetime and at autopsy: A study of 83 women. Cancer 1984;54(4):612-615. [http://dx.doi.org/10.1002/1097-0142(1984)54:4%3C612::AID-CNCR2820540403%3E3.0.CO;2-B] [ Links ]
20. Freedman BC, Smith SM, Estabrook A, et al. Incidence of occult carcinoma and high-risk lesions in mammaplasty specimens. Int J Breast Cancer 2012;2012:145630. 'http://dx.doi.org/10.1155/2012/145630] [ Links ]
21. Titley OG, Armstrong AP, Christie JL, et al. Pathological findings in breast reduction surgery. Br J Plast Surg 1996;49(7):447-451. [http://dx.doi.org/10.1016/S0007-1226(96)90028-4] [ Links ]
22. Rudolph R, Niedbala AR. Surgical management of the patient with invasive carcinoma discovered at reduction mammoplasty. Am Surg 2003;69(11):1003-1005. [ Links ]
23. Golshan M, Lesnikoski BA, Lester S. Sentinel lymph node biopsy for occult breast cancer detected during breast reduction surgery. Am Surg 2006;72(5):397-400. [ Links ]
24. McPherson K. Screening for breast cancer - balancing the debate. BMJ 2010;340:c3106. [http://dx.doi.org/10.1136/bmj.c3106] [ Links ]
25. Screening for breast cancer: US Preventive Services Task Force recommendation statement. Ann Intern Med 2009;151(10):716-736. [http://dx.doi.org/10.7326/0003-4819-151-10-200911170-00008] [ Links ]
26. Keshtgar M, Hamidian Jahromi A, Davidson T, et al. Tissue screening after breast reduction. BMJ 2009;338:b630. [http://dx.doi.org/10.1136/bmj.b630] [ Links ]
 Correspondence:
Correspondence:
C Sofianos
sofianosc@gmail.com
Accepted 13 February 2015


{kind=link}
{kind=link}