










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSAMJ: South African Medical Journal
versión On-line ISSN 2078-5135
versión impresa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.105 no.4 Pretoria abr. 2015
http://dx.doi.org/10.7196/SAMJ.9179
FORUM
MANAGEMENT OF OBSTETRIC HAEMORRHAGE
Oxytocin - ensuring appropriate use and balancing efficacy with safety
Z FarinaI; S FawcusII
IMB ChB, DA (SA), FCA (SA), is National Anaesthetic Assessor for the National Committee for Confidential Enquiries into Maternal Deaths in South Africa (NCCEMD), Chief Specialist in the Pietermaritzburg Metropolitan Department of Anaesthesia, and an honorary lecturer in anaesthesia at the College of Health Sciences, School of Clinical Medicine, University of KwaZulu-Natal, Durban, South Africa
IIMA, MB ChB, FRCOG, is an obstetric assessor for the NCCEMD and a professor in the Department of Obstetrics and Gynaecology, Faculty of Health Sciences, University of Cape Town, South Africa, and heads the Obstetric Unit at Mowbray Maternity Hospital, Cape Town
ABSTRACT
Maternal deaths due to haemorrhage continue to increase in South Africa (SA). It appears that oxytocin and other uterotonics are not being used optimally, even though they are an essential part of managing maternal haemorrhage. Oxytocin should be administered to every mother delivering in SA. Awareness is required of the side-effects that can occur and the appropriate measures to avoid harm from these. Second-line uterotonics should also be available and utilised in conjunction with mechanical and surgical means to arrest haemorrhage in women who continue to bleed after the appropriate administration of oxytocin.
The National Committee for Confidential Enquiries into Maternal Deaths in South Africa (NCCEMD) has issued an alert regarding the continuing high levels of maternal deaths due to obstetric haemorrhage, the majority of which are judged to be preventable. This is especially noted for haemorrhage during and after caesarean section (CS).
The preliminary data of the 2011 - 2013 Saving Mothers triennial report reveal that obstetric haemorrhage accounted for 684 maternal deaths, making it the second most common cause of maternal death.[1] There were 221 deaths (32.3%) ascribed to haemorrhage associated with CS. This bleeding was detected intraoperatively or postoperatively, or was intra-abdominal. Frequently bleeding was due to uterine atony secondary to prolonged labour, other causes being traumatic extensions of the uterine incision or placental site bleeding. Maternal death assessors found over 85% of these deaths to be clearly avoidable.
Issues contributing to these deaths
The following major causes have been identified among the cohort of the 2011 - 2013 deaths ascribed to haemorrhage:
- Inadequate utilisation of uterotonic agents
- Poor recognition of the severity of the blood loss causing hypovolaemia
- Inadequate surgical skill
- Delays in relaparotomy and/or referral in case of post-CS bleeding.
Specific problems with uterotonics
- Poor documentation of whether prophylactic oxytocin was given, by what route and in what dosage (there is no designated space on the recommended anaesthetic form, the recommended surgery form or the anaesthetic assessment tool used by the NCCEMD to record oxytocin use)
- Poor documentation of additional uterotonic agents given to treat uterine atony, both by the anaesthetist during the surgery and by the obstetrician or nurses postoperatively
- Insufficient prophylactic dose of oxytocin at CS (e.g. several cases when only a 10 IU oxytocin infusion was given, and several where no uterotonic agent was given at all)
- Excessive intravenous (IV) boluses of oxytocin (e.g. 10 IU IV bolus)
- Inadequate dosages of therapeutic oxytocin for treatment of established intraoperative bleeding due to an atonic uterus (e.g. a repeat 2 - 3 IU IV bolus not given, or infusion containing a too-low concentration of oxytocin administered; 10 IU instead of the recommended 20 - 40 IU infusion)
- Infrequent use of ergometrine or oxytocin/ergometrine (Syntometrine) as treatment for uterine atony at CS, even in women with no contraindication to ergot alkaloids. These agents are of similar efficacy to oxytocin and therefore would be expected by inference to have superior efficacy to misoprostol.[2] Ergometrine has a longer duration of action than oxytocin.[3]
Oxytocin
A key step in avoiding postpartum haemorrhage (PPH) is ensuring adequate uterine contraction, as this serves to control bleeding from the placental bed naturally.
The mainstay of uterotonic drugs in obstetric practice has been oxytocin. However, recently this drug has become a cause for concern among anaesthesiologists. The 1997 - 1999 triennial report of the Confidential Enquiries into Maternal Deaths in the UK cited the administration of 10 IU oxytocin as an IV bolus as the precipitating cause of death in two hypovolaemic patients and as contributing to the deaths of a number of other patients.[4] This problem was noted as contributory in two deaths in the 2005 - 2007 NCCEMD report[5] in South Africa (SA) and in another three cases in the 2008 -2010 report.[6] A preliminary review of the 2011 - 2013 NCCEMD anaesthesia data reveals that the problem is still occurring.
Over-reaction to adverse reports
Anecdotally, there appears to have been a marked over-reaction to this information, with a number of medical practitioners avoiding the use of oxytocin entirely. There has been much discussion of the NCCEMD findings concerning bleeding at CS in obstetric and anaesthetic forums. There is evidence of differences of opinion about the use of oxytocin at CS in situations of hypovolaemia and hypotension, especially when this situation has arisen as a result of bleeding from uterine atony at CS. Obstetricians appear to request higher doses of oxytocin to contract the uterus, but anaesthetists express reluctance to administer oxytocin because of concern about worsening the hypotension. The conflict seems more pronounced among junior obstetric doctors and anaesthetists.
An over-reaction to the information of potential harm is inappropriate. Oxytocin is still highly beneficial, and administration of this drug needs to continue, both intraoperatively and postoperatively. Obviously protocol adaptations need to be made to ensure that the reported adverse events do not impact on the patient. In the situation of hypovolaemic shock, a rapid high-dose IV bolus of oxytocin is contraindicated, but an infusion is essential to contract the uterus. This should be provided in addition to active fluid, colloid and red blood cell concentrate resuscitation, and the concomitant use of vasopressors. The obstetric surgeon needs to have the expertise to perform surgical measures to reduce bleeding, such as uterine compression sutures, if all medical therapy is unsuccessful.
Vasodilation caused by oxytocin
The main adverse effect of oxytocin is hypotension secondary to vasodilation. This appears to be mediated by calcium-dependent stimulation of nitric oxide release.[3] In animal studies coronary vasoconstriction has been demonstrated.[7] Of concern is the repeated finding of significant reproducible ST depression on the electrocardiogram in pregnant women receiving IV oxytocin boluses.[8] The adverse effects appear to be more marked at higher bolus doses and with more rapid administration. The cardiovascular effects of oxytocin have been well documented and produce a clinical picture of peripheral vasodilation, hypotension and increased pulmonary artery pressures. Cardiac output is increased by an increase in both heart rate and stroke volume.[3] The increase in heart rate and stroke volume protects the majority of women from adverse outcomes, but clearly points to a group who will be especially vulnerable to cardiovascular collapse: those women who cannot achieve an increase in cardiac output. This problem is especially marked in patients who are already hypovolaemic.
It has been determined that the ED90 effect for uterine myocyte stimulation (the dose that can be expected to confer 90% maximal contraction) is 0.35 IU in oxytocin-naïve patients at CS[9] and 3.0 IU in patients who have previously been augmented with oxytocin during labour.[10] Another important finding is that the magnitude of the hypotensive effect of oxytocin appears to be reduced with the administration of repeated doses.[3]
In common with all short-acting drugs (oxytocin has a plasma half-life of 3 - 20 minutes[11]), administration of larger IV boluses of oxytocin to try to prolong effects leads to excessive peaks in concentration, but little increase in the duration of action. The solution to this effect is repeated smaller boluses, and/or a constant infusion of the drug.
Suggested dosing of oxytocin
These observations suggest that the use of the lowest effective dose of oxytocin that produces adequate uterine contraction will improve the risk/benefit profile. In the event of inadequate uterine contraction after delivery of the baby, the obstetric surgeon should undertake the usual physical manoeuvres such as removal of any remaining products of conception and manual rubbing up the uterus while the anaesthetist administers a repeat bolus of oxytocin (2.5 IU over 30 seconds). The infusion rate of the oxytocin should be increased simultaneously. It is important to ensure that the postoperative infusion of oxytocin should not be interrupted in any manner.
It has also been noted that the vasodilatory effect of an oxytocin bolus can be countered by administration of a concurrent dose of phenylephrine.[12] When administering oxytocin to a hypotensive hypovolaemic woman, in addition to the normal resuscitative measures of rapid fluid administration it would be appropriate to administer phenylephrine 50 - 100 μg as an intravenous infusion (IVI).
Prophylactic use of oxytocin at CS
Recommendations for the routine prophylactic administration of oxytocin at CS have previously been issued in SA.[13] These can be summarised as prophylactic administration of 2.5 IU oxytocin as an IVI over 1 minute, followed by 20 IU in 1 L clear fluid over 8 hours. In the situation where haemorrhage is occurring, judicious administration of increased doses of oxytocin is required. The oxytocin infusion regimen may be increased up to the equivalent of 10 IU/h (80 IU in 1 000 mL fluid at 125 mL/h). Where there is access to a syringe driver, this can be achieved by placing 100 IU oxytocin in 50 mL saline and running it at 5 mL/h.
Controlled postoperative infusion of oxytocin for at least 8 hours is the gold standard for the pharmacological prevention of PPH after CS. This is especially important if the obstetrician is inexperienced.[14] However, it may be difficult to achieve in some hospital environments, where care in the wards is erratic and there is limited access to labour-saving devices such as rate controllers. Mechanical rate controllers (Dial-A-Flo) have been utilised, but are dependent on a functioning IVI line and a specific height of the attached IVI fluid, while flow rates are not constant when other fluids are 'piggy backed' onto the IVI line.
Medical practitioners should motivate for mechanical rate-controlling devices (infusion pumps and syringe drivers) where possible. When it is not possible to achieve reliable oxytocin infusion for at least 8 hours after CS, the intramuscular administration of oxytocin 10 IU 4-hourly or oxytocin/ergometrine 5 IU/0.5 μg 8-hourly may provide a satisfactory alternative.
Ergometrine
Ergometrine is a uterotonic drug that has received bad publicity, firstly because ergometrine is contraindicated when vasoconstriction is a major concern (hypertension and cardiac disease), and secondly because it has pronounced side-effects such as nausea and emesis. However, ergometrine has an alternative mechanism of action to either oxytocin or misoprostol, and represents a useful second-line agent. The vasoconstrictive action of ergometrine counterbalances the vasodilation of oxytocin. Small IV doses of 0.2 mg, building up to a maximum total of 0.6 mg, are beneficial. Ergometrine has a long duration of action (half-life 120 minutes).[3]
Misoprostol
Misoprostol (Cytotec) has become a popular means of causing uterine contraction. It is easy to administer orally, rectally or sublingually, and appears benign. However, concerning data have been published about adverse effects and worsening outcomes at higher doses.[2] While side-effects of pyrexia and tachycardia are well documented, misoprostol may be a useful adjunct when used in appropriate doses. Since many patients will have received prior doses of misoprostol, it is important to check carefully on the total dose already administered; sufficient drug should be given to bring the total dose up to 600 mg. Anaesthetists find that misoprostol is often most conveniently administered sublingually. The fact that it does not require refrigeration is an advantage in the resource-poor environment.
Prostaglandin F2-alpha
Prostaglandin F2-alpha is often used as a 'last line' of pharmacological action. It is very potent, and severe hypertension and bronchospasm have been recorded after IV use.[15] Off-label intramyometrial injection has been described,[16] but its use should be confined to institutions with specialist skills and experience.
Guidance for use of uterotonics
The NCCEMD has produced guidelines on the prevention and treatment of blood loss at CS adapted from World Health Organization guidelines, Royal College of Obstetricians and Gynaecologists guidelines and recommendations from obstetric anaesthetic experts.[3,17,18] These are found in the monograph of management of PPH in SA, which contains algorithms outlining use of uterotonic agents.[19] Of note, most international guidelines on prevention and treatment of PPH focus on vaginal delivery and do not separately specify routes and dosages for CS. There is a need to strengthen guidance for use of uterotonics at CS, globally and in SA.
The SA guidelines have been described in a number of publi-cations,[19,20] and wall posters for use in operating theatres have been developed.
The NCCEMD advocates that the problem of maternal death be approached under the '5Cs':
1. Care - a Commitment to quality
2. Coverage - ensuring that all woman receive the care they deserve
3. Caesarean section safety
4. Contraception
5. Community involvement.
The suggestions in this article encompass three of these important principles.
Commitment to quality
Implement and enforce recognised protocols. Hitherto, the uptake of these guidelines and algorithms has not been widespread.
Implement methods of monitoring uteronic administration. The recommended monitoring tools have been added to the maternity case record charts and the assessment tools used by the confidential enquiry processes. Documentation needs to be improved in SA hospitals.
Coverage
Effective rollout of guidelines at district level must occur, and familiarity with them among the anaesthetic fraternity must increase.
Managers of health facilities conducting CS need to ensure availability of the appropriate drugs, and facilities for administration of these drugs.
Caesarean section safety
It is very important that anaesthetists, obstetricians and midwives achieve consensus on the use of oxytocin and other uterotonics at CS, so that uterine atony at CS can be prevented and treated adequately.
Renewed emphasis on these issues needs to be encouraged via medical schools, the district clinical specialist teams, the Essential Steps in the Management of Obstetric Emergencies programme and the national anaesthesiology and obstetric societies.
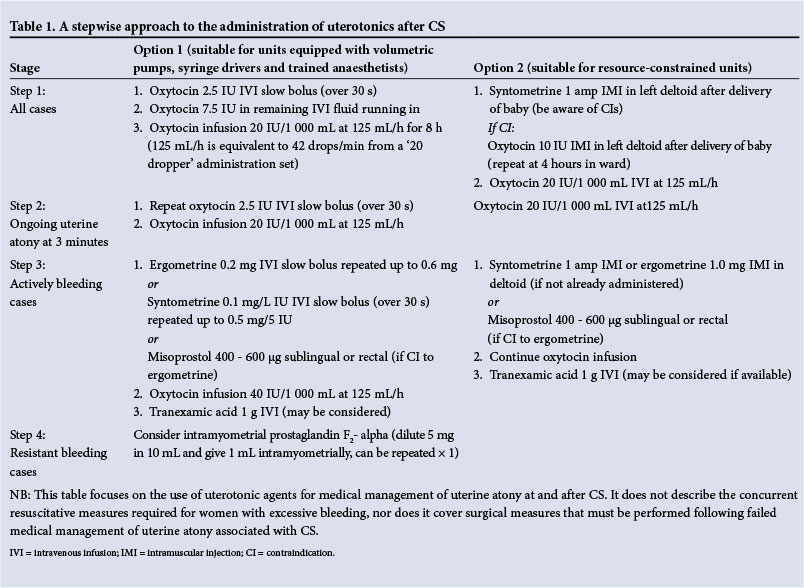
Table 1 presents a guideline for a stepwise approach to use of uterotonics at CS that has been mutually agreed on between obstetricians and anaesthetists of the NCCEMD and is evidence based.
Conclusion
We strongly recommend roll-out and implementation of these guidelines at all SA facilities conducting CS. The continued increase in deaths from maternal haemorrhage, particularly after CS, is unacceptable. It is the responsibility of the doctors giving the anaesthetic, the doctors performing the surgery and the nurses performing postoperative monitoring to reduce these deaths.
Acknowledgement. The authors thank Prof. J Moodley, Prof. J Hofmeyer and Dr D G Bishop for constructive advice and comments on this article.
References
1. Pattinson RC, ed. Saving Mothers 2011-2013: The Sixth Report of the National Committee for Confidential Enquiries into Maternal Deaths in South Africa. Pretoria: Government Printer, 2014. [ Links ]
2. Tunçalp Ö, Hofmeyr GJ, Gülmezoglu AM. Prostaglandins for preventing postpartum haemorrhage. Cochrane Database Syst Rev 2011, Issue 3. Art. No.: CD000494. [http://dx.doi.org/10.1002/14651858.CD000494.pub4] [ Links ]
3. Dyer RA, van Dyk D, Dresner A. The use of uterotonic drugs during caesarean section. Int J Obst Anesth 2010;19(3):313-319. [http://dx.doi.org/10.1016/j.ijoa.2010.04.011] [ Links ]
4. Royal College of Obstetricians and Gynaecologists. Why Mothers Die. Report on Confidential Enquiries into Maternal Deaths, 1997-9. London: RCOG, 2001. [ Links ]
5. Pattinson RC, ed. Saving Mothers: Fourth Report on Confidential Enquiries into Maternal Deaths in South Africa 2005 - 2007. Pretoria: National Department of Health, 2010. [ Links ]
6. Pattinson RC, ed. Saving Mothers: Fifth Report on Confidential Enquiries into Maternal Deaths in South Africa 2008 - 2010. Pretoria: National Department of Health, 2012. [ Links ]
7. Fortner CL. Effects of synthetic oxytocin with and without preservatives upon coronary blood flow in the dog. J Pharmacol Exp Ther 1969;165(2):258-266. [ Links ]
8. Jonsson M, Hanson U, Lidell C, Norde'n-Lindeberg S. ST depression at caesarean section and the relation to oxytocin dose: A randomised controlled trial. BJOG 2010;117(1):76-83. [http://dx.doi.org/10.1111/j.1471-0528.2009.02356.x] [ Links ]
9. Carvalho JC, Balki M, Kingdom J, Windrim R. Oxytocin requirements at elective caesarean delivery: A dose-finding study. Obstet Gynecol 2004;104(5):1005-1010. [http://dx.doi.org/10.1097/01.AOG.0000142709.04450.bd] [ Links ]
10. Balki M, Ronayne M, Davies S, et al. Minimum oxytocin dose requirement after cesarean delivery for labor arrest. Obstet Gynecol 2006;107(1):45-50. [http://dx.doi.org/10.1097/01.AOG.0000191529.52596.c0] [ Links ]
11. Syntocinon® [package insert]. Novartis Pharmaceuticals Australia Pty. Ltd., 12 March 2009. [ Links ]
12. Dyer RA, Reed AR, van Dyk D, et al. Hemodynamic effects of ephedrine, phenylephrine, and the coadministration of phenylephrine with oxytocin during spinal anesthesia for elective cesarean delivery. Anesthesiology 2009;111(4):753-765. [http://dx.doi.org/10.1097/ALN.0b013e3181b437e0] [ Links ]
13. Farina Z, Rout C. Anaesthesia for caesarean section In: Moodley J, ed. A Monograph on Caesarean Section. Pretoria: National Department of Health, 2013:9-29. http://www.hst.org.za/publications/saving-mothers-caesarean-section-monograph-2013 (accessed 6 February 2015). [ Links ]
14. Sheehan SR, Montgomery AA, Carey M, et al. Oxytocin bolus versus oxytocin bolus and infusion for control of blood loss at elective caesarean section: Double blind, placebo controlled, randomised trial. BMJ 2011;343:d4661. [http://dx.doi.org/10.1136/bmj.d4661] [ Links ]
15. Harber C, Levy D, Chidambaram S, Macpherson M. Case report: Life-threatening bronchospasm after intramuscular carboprost for postpartum haemorrhage. BJOG 2007;114(3):366-368. [http://dx.doi.org/10.1111/j.1471-0528.2006.01227.x] [ Links ]
16. Chou MM, MacKenzie IZ. A prospective, double-blind, randomized comparison of prophylactic intramyometrial 15-methyl prostaglandin F sub 2alpha, 125 micrograms, and intravenous oxytocin, 20 units, for the control of blood loss at elective cesarean section. Am J Obstet Gynecol 1994;171(5):1356- 1360. [http://dx.doi.org/10.1016/0002-9378(94)90160-0] [ Links ]
17. World Health Organization. WHO Guidelines for the Management of Postpartum Haemorrhage and Retained Placenta. Geneva: WHO, 2012. [ Links ]
18. Royal College of Obstetricians and Gynaecologists. Postpartum Haemorrhage, Prevention and Management (Green-top Guideline No. 52). London: RCOG, May 2009. https://www.rcog.org.uk/en/guidelines-research-services/guidelines/gtg52/ (accessed 26 February 2015). [ Links ]
19. South African National Committee for Confidential Enquiries into Maternal Deaths. A Monograph of the Management of Postpartum Haemorrhage. Pretoria: National Department of Health, 2010. [ Links ]
20. Fawcus S, Moodley J. Postpartum haemorrhage associated with caesarean section and caesarean hysterectomy. Best Pract Res Clin Obstet Gynaecol 2013; 27(2):233-249. [http://dx.doi.org/10.1016/j.bpobgyn.2012.08.018] [ Links ]
 Correspondence:
Correspondence:
Z Farina
zane.farina@kznhealth.gov.za
Accepted 24 November 2014


{kind=link}