










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.105 n.4 Pretoria Apr. 2015
http://dx.doi.org/10.7196/SAMJ.8927
FORUM
ISSUES IN PUBLIC HEALTH
Food insecurity in households in informal settlements in urban South Africa
N NaickerI; A MatheeII; J TeareIII
IMB BCh, FCPHM, PhD, is based at the Environment and Health Research Unit, South African Medical Research Council, and is an honorary lecturer at the School of Public Health, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IIPhD, is the Director of the Environment and Health Research Unit, and holds honorary professorial positions in the Wits School of Public Health and the Faculty of Health Sciences, University of Johannesburg
IIIMSc (Med), is a senior scientist at the Environment and Health Research Unit, currently based at Nelson Mandela Metropolitan University, Port Elizabeth, South Africa
ABSTRACT
Food insecurity in the urban poor is a major public health challenge. The Health, Environment and Development study assessed trends in food insecurity and food consumption over a period of 7 years in an informal settlement in Johannesburg, South Africa (SA). Annual cross-sectional surveys were conducted in the informal settlement (Hospital Hill). The degree of household food insecurity decreased significantly from 2006 (85%) to 2012 (70%). There was a spike in 2009 (91%), possibly owing to global food price increases. Childhood food insecurity followed the same trend as household food insecurity. During the first 3 study years, consumption of protein, vegetables and fruit decreased by 10 - 20%, but had returned to previous levels by 2012. In this study, although declining, food insecurity remains unacceptably high. Hunger relief and poverty alleviation need to be more aggressively implemented in order to improve the quality of life in poor urban communities in SA.
Food security is a basic human right. However, during the period 2010 - 2012, 852 million people in developing countries remained food insecure.[1,2] Of these 852 million people, 234 million lived in sub-Saharan Africa.[1] The First Millennium Development Goal endeavoured to reduce hunger by half from 1990 to 2015. Reports produced by the United Nations Food and Agriculture Organisation (FAO) indicate that progress towards this goal has been slow, and declined after 2009.[1]
In South Africa (SA), three national surveys showed a decrease (from 52.3% to 25.9%) in food insecurity over the 10-year period 1999 - 2008.[3] In urban areas, food insecurity decreased from 42% to 20.5%. In 2009, a study conducted in three impoverished communities in Johannesburg, SA, showed that 56% of all households surveyed were food insecure and 60% of households in an informal settlement were food insecure.[4]
Food insecurity has been linked to detrimental health outcomes such as obesity, chronic diseases and mental health disorders in adults.[5-9] In children, research has established a relationship between food insecurity and stunting, poor development and decreased academic ability.[10-13] The literature contains numerous publications pointing to a variety of factors that increase the risk of being food insecure, such as poverty, lower levels of maternal education, unemployment, larger household size, and households that experience events that place an added demand on their budgets.[14,15]
Cities, especially in developing countries, are highly heterogeneous, with communities ranging from extremely wealthy to impoverished. National surveys are limited and provide an overview, but often do not reflect the degree of food insecurity faced by very poor, marginalised communities such as those residing in informal settlements.
Case study
The Health, Environment and Development study was conducted in an informal settlement (Hospital Hill) in Johannesburg to assess trends in food security from 2006 to 2012. The main predictors of food insecurity in this community and associated health outcomes were determined. Hospital Hill is located on the south-western outskirts of Johannesburg. A convenience sample of 188 dwellings was initially drawn for inclusion in the study. The response rate ranged from 55% in 2006 to 73% in 2012.
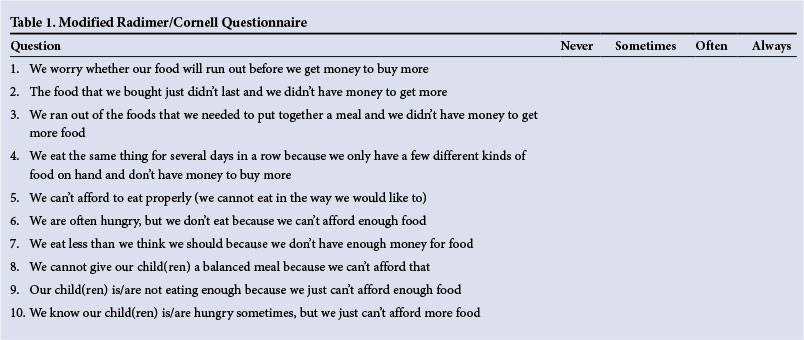
At the selected dwellings, after written, informed consent had been obtained, a prestructured questionnaire was administered to a household member at least 18 years of age to obtain information on sociodemographic status, perceptions of housing and neighbourhood conditions, food security and health status. The Radimer/Cornell Questionnaire Rating Scale[16] was modified to assess food security in households (Table 1). This scale normally assesses food security in individuals. Modified versions of this tool have been validated in developing countries such as Indonesia.[17] For the purpose of analysis the households were grouped into three categories:
- Food secure: if the interviewee answered 'never' to all questions
- Household food insecure: if they answered 'sometimes', 'often' or 'always' to one or more questions related to household food security (questions 1 - 7)
- Child food insecure: if they answered 'sometimes', 'often' or 'always' to one or more questions related to childhood food security (questions 8 - 10).
The categories 'sometimes', 'often' and 'always' were combined and a binary variable produced.
Food security and related socioeconomic factors
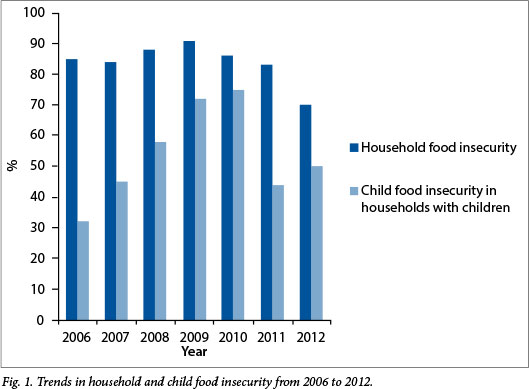
The results of this study showed a high degree of household food insecurity in the Hospital Hill community. In 2006, 85% of households were food insecure. This increased and peaked at 91% in 2009. Between 2009 and 2012, the number of food-insecure households decreased by 21%. These results are indicative of the effects of the 2007 - 2009 food price increases experienced globally, and confirm the vulnerability of the very poor.[1] In households with children, 67% were food insecure. Households with children were therefore more likely to be food insecure, but the association was not statistically significant (p=0.1). However, there was a significant risk of child food insecurity if the whole household was food insecure (p<0.01) (Fig. 1).
The degree of food security has been shown, in this study and in the literature, to vary within and between households in the same community over time, owing to economic and other stressors such as illness or unexpected expenses.[1,18] Compared with national levels of food insecurity (estimated at 48%),[3] residents of this urban informal settlement face a much higher level of food insecurity (70%). The same is likely to apply to other urban informal settlement communities in SA.
Factors such as very low income (<ZAR1 000 per month; 1.00 ZAR = 0.09 USD at the time of writing) (p=0.01; crude odds ratio (OR) 3.46; 95% confidence interval (CI) 2.13 - 5.62), low asset ownership (p<0.01; crude OR 4.11; 95% CI 2.31 - 7.32), having a higher number of major problems with the dwelling (p<0.01; crude OR 3.48; 95% CI 2.19 - 5.54) and lack of full-time employment of the head of the household (p=0.01; crude OR 2.81; 95% CI 1.21 -6.53) were significantly associated with an increased risk of having a food-insecure household. This study confirms the well-documented finding that indicators of poor socioeconomic status are predictive of food insecurity.[3,19,20] Monthly food expenditure was significantly lower in food-insecure relative to food-secure households (p=0.04), indicating the degree of poverty faced by food-insecure households. According to Bonti-Ankomah,[21] an average household of four members in 2001 needed at least R1 146 per month to obtain a healthy diet for all members. Owing to inflation, higher monthly food expenditure would be expected in 2012. In this Hospital Hill community, households spent on average only R753.61 on food, an increase of R119.97 from 2009 to 2012.
Household food consumption from 2006 to 2012
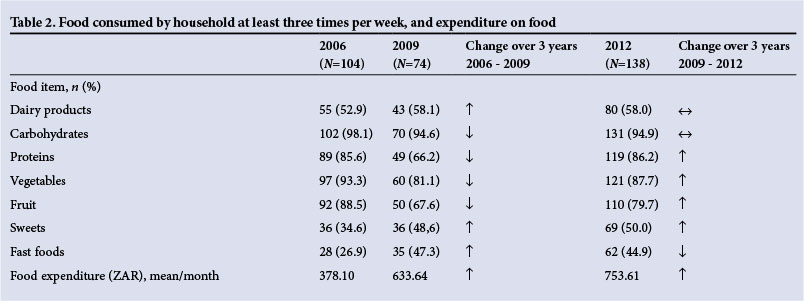
From 2006 to 2009, there was a 10 - 20% decrease in the consumption of vegetables, protein foods and fruit. However this increased steadily from 2009 to 2012 to approximately the same levels as in 2006, indicating that in periods of food stress or economic downturn, consumption of vegetables, fruit and protein decreased (Table 2). Another finding of this study is the increased trend in the consumption of fast foods, which climbed by 18% between 2006 and 2009, and was sustained at the higher level of consumption in subsequent years. Undernutrition or malnutrition, i.e. a lack of adequate micronutrients, is a major consequence of chronic food insecurity.[18,20] Coping strategies during periods of food insecurity such as decreasing the variety of foods eaten, limiting portion sizes and eating cheaper fast foods will affect nutritional status negatively.[19,22]
The 2012 FAO report showed that worldwide, more than 2.5 million children die each year from malnutrition as a consequence of food insecurity.[1] Sub-Saharan Africa has the highest rates of child underweight and infant and child mortality in the world.[1] Underweight and stunting are common among undernourished children, although at a global level the percentage of stunting and underweight in children has decreased.[1] In SA, this decrease may be attributed to interventions such as the Child Support Grant or school food programmes.[1,3] However, such national or provincial programmes may not be enough to mitigate the effects of high levels of food insecurity (70% in 2012) in very poor urban households.[18] The study by Oldewage-Theron et al.[19] in an SA informal settlement showed that 31% of boys and 30% of girls were stunted. The review by Labadarios et al.[3] on the national surveys in SA indicated that the diet consumed by poor SA children was inadequate and did not meet nutritional requirements. These national surveys also confirmed the limited variety of foods consumed.[3] Therefore, although hunger and food insecurity may not be widespread in SA in general, there are communities that are particularly vulnerable.[19]
Food insecurity and health outcomes
Levels of chronic disease in this community were relatively low, with only 24% being affected with any type of chronic disease (diabetes mellitus, hypertension or heart disease). Twenty per cent of households with a member who had a chronic disease were food insecure. Thirteen per cent of respondents in food-insecure households screened positive for common mental health disorders (anxiety or depression) using the World Health Organization self-reporting questionnaire,[23] compared with 1% in food-secure households; however, this difference was not significant (p=0.34). While we did not find a significant association with health outcomes, chronic illness has been shown to be a predictor and a consequence of food insecurity, and in some cases the hungry are forced to choose between food and medicine.[24] Sorsdahl et al,[5] showed in a national survey that after controlling for socioeconomic data, food insecurity was significantly related to having a 12-month and lifetime Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV)-confirmed diagnosis of an anxiety disorder. A possible reason for the low levels of chronic ill health or common mental disorders may be the sociodemographic profile of the Hospital Hill community.
Conclusion
This study highlights the plight of South Africans living in urban informal settlements where poverty levels dictate the degree of food insecurity. As an immediate solution, social grants may help to alleviate deprivation by increasing household income, but medium- and long-term strategies such as increased employment opportunities, education and the empowerment of women are required.
References
1. FAO, WFP and IFAD. The State of Food Insecurity in the World 2012. Economic Growth Is Necessary But Not Sufficient To Accelerate Reduction of Hunger and Malnutrition. Rome: Food and Agricultural Organization of the United Nations, 2012. http://www.fao.org/docrep/016/i3027e/i3027e.pdf(accessed 10 March 2014). [ Links ]
2. De Weerdt J, Beegl K, Friedman J, Gibson J. The Challenge of Measuring Hunger. Policy Research Working Paper No. WPS 6736. Washington, DC: World Bank Group, 2014. http://documents.worldbank.org/curated/en/2014/01/18741920/challenge-measuring-hunger (accessed 15 February 2014). [ Links ]
3. Labadarios D, Mchiza ZJ-R, Steyn NP, et al. Food security in South Africa: A review of national surveys. Bull World Health Organ 2011;89:891-899. [http://dx.doi.org/10.2471/BLT.11.089243] [ Links ]
4. Rudolph M, Kroll F, Ruysenaar S, Dlamini T. The State of Food Insecurity in Johannesburg. Urban Food Security Series No. 12. Kingston and Cape Town: Queen's University and AFSUN, 2012. [ Links ]
5. Sorsdahl K, Slopen N, Siefert K, Seedat S, Stein DJ, Williams DR. Household food insufficiency and mental health in South Africa. J Epidemiol Community Health 2011;65(5):426-431. [http://dx.doi.org/10.1136/jech.2009.091462] [ Links ]
6. Stuff JE, Casey PH, Szeto KL, et al. Household food insecurity is associated with adult health status. J Nutr 2004;134(9):2330-2335. [ Links ]
7. Heflin C, Ziliak J. Food insufficiency, food stamp participation and mental health. Soc Sci Q 2008;89(3):706-727. [http://dx.doi.org/10.1111/j.1540-6237.2008.00556.x] [ Links ]
8. Adams EJ, Grummer-Strawn L, Chavez G. Food insecurity is associated with increased risk of obesity in California women. J Nutr 2003;133(4):1070-1074. [ Links ]
9. Ford ES. Food security and cardiovascular disease risk among adults in the United States: Findings from the National Health [ Links ]
10. Casey PH, Szeto KL, Robbins JM, et al. Child health-related quality of life and household food security. Arch Pediatr Adolesc Med 2005;159(1):51-56. [ Links ]
11. Matheson DM, Varady J, Varady A, Killen JD. Household food security and nutritional status of Hispanic children in the fifth grade. Am J Clin Nutr 2002;76(1):210-217. [ Links ]
12. Alaimo K, Olson CM, Frongillo EA jr. Food insufficiency and American school-aged children's cognitive, academic, and psychosocial development. Pediatrics 2001;108(1):44-53. Erratum in: Pediatrics 2001;108(3):824. [http://dx.doi.org/10.1542/peds.108.3.824b] [ Links ]
13. Jyoti DF, Frongillo EA, Jones SJ. Food insecurity affects school children's academic performance, weight gain, and social skills. J Nutr 2005;135(12):2831-2839. [ Links ]
14. Ben-Davies ME, Kinlaw A, Estrada del Campo Y, Bentley ME, Siega-Riz AM. Risk factors associated with the presence and severity of food insecurity in rural Honduras. Public Health Nutr 2014;17(1):5-13. [http://dx.doi.org/10.1017/S1368980013002048] [ Links ]
15. Rose D. Economic determinants and dietary consequences of food insecurity in the United States. J Nutr 1999;129(2 Suppl):517S-520S. [ Links ]
16. Radimer KL, Olson CM, Campbell CC. Development of indicators to assess hunger. J Nutr 1990;120(11 Suppl):1544-1548 [ Links ]
17. Studdert LJ, Frongillo EA jr, Valois P. Household food insecurity was prevalent in Java during Indonesia's economic crisis. J Nutr 2001;131(10):2685-2691. [ Links ]
18. Altman M, Hart TGB, Jacobs PT. Household food security status in South Africa. Agrekon 2009;48(4):345-361. [http://dx.doi.org/10.1080/03031853.2009.9523831] [ Links ]
19. Oldewage-Theron WH, Dicks EG, Napier CE. Poverty, household food insecurity and nutrition: Coping strategies in an informal settlement in the Vaal Triangle, South Africa. Public Health 2006;120(9):795-804. [http://dx.doi.org/10.1016/j.puhe.2006.02.009] [ Links ]
20. Bhattacharya J, Currie J, Haider S. Poverty, food insecurity, and nutritional outcomes in children and adults. J Health Econ 2004;23(4):839-862. [http://dx.doi.org/10.1016/j.jhealeco.2003.12.008] [ Links ]
21. Bonti-Ankomah S. Addressing Food Insecurity in South Africa. Pretoria: National Institute for Economic Policy, 2001. http://www.sarpn.org.za/EventPpers/Land/20010605Bonti.pdf (accessed 10 April 2014). [ Links ]
22. Battersby J, McLachlan. Urban food insecurity: A neglected public health challenge. S Afr Med J 2013;103(10):716-717. [http://dx.doi.org/10.7196/SAMJ.7463] [ Links ]
23. Beusenberg M, Orley JH. A User's Guide to the Self Reporting Questionnaire (SRQ). World Health Organisation 1994. Geneva: World Health Organization. http://www.who.int/iris/handle/10665/61113#sthash.XudX8GOM.dpuf (accessed 10 March 2014). [ Links ]
24. Biros MH, Hoffman PL, Resch K. The prevalence and perceived health consequences of hunger in emergency department patient populations. Acad Emerg Med 2005;12(4):310-317.[http://dx.doi.org/10.1197/j.aem.2004.12.006] [ Links ]
 Correspondence:
Correspondence:
N Naicker
nisha.naicker@mrc.ac.za
Accepted 13 February 2015


{kind=link}
{kind=link}