










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.105 n.2 Pretoria Feb. 2015
http://dx.doi.org/10.7196/samj.8792
FORUM
TRAUMA CARE
Trauma quality improvement: The Pietermaritzburg Metropolitan Trauma Service experience with the development of a comprehensive structure to facilitate quality improvement in rural trauma and acute care in KwaZulu-Natal, South Africa
D L Clarke
Was a surgeon at Durban's South Beach, also known as Addington Hospital. Since fleeing the ongoing attempts to gentrify and 'Disneyfy' the beachfront, he has tried to reinvent himself as a faux Midlands farmer and member of the landed gentry in the misty foothills of the Drakensberg
ABSTRACT
Improving the delivery of efficient and effective surgical care in rural South Africa is a mammoth task bedevilled by conflict between the stakeholders, who include rural doctors, surgeons, ancillary staff, researchers, educators and administrators. Management training is not part of most medical school curricula, yet as they progress in their careers, many clinicians are required to manage a healthcare system and find the shift from caring for individual patients to managing a complex system difficult. Conflict arises when management-type interventions are imposed in a top-down manner on surgical staff suspicious of an unfamiliar field of study. Another area of conflict concerns the place of surgical research. Researchers are often accused of not being sufficiently focused on or concerned about the tasks of service delivery. This article provides an overview of management theory and describes a comprehensive management structure that integrates a model for healthcare systems with a strategic planning process, strategic planning tools and appropriate quality metrics, and shows how the Pietermaritzburg Metropolitan Trauma Service in KwaZulu-Natal Province, South Africa, successfully used this structure to facilitate and contextualise a diverse number of quality improvement programmes and research initiatives in the realm of rural acute surgery and trauma. We have found this structure to be useful, and hope that it may be applied to other acute healthcare systems.
The strategic planning process and healthcare systems
Strategic planning is a systematic process designed to assist organisational decision-making by taking account of the microenvironment(s) within an organisation, as well as the macroenvironment in which the organisation exists.[1-5] Healthcare systems are complex and tightly coupled. Strategic planning within such a system, without an overarching framework to provide a structure for quality improvement programmes, risks becoming ad hoc, haphazard, ineffectual and even counterproductive. The strategic planning process must identify the organisation's vision and mission or the system's aims and objectives. The mission statement explains the reasons for the healthcare system's existence. The vision statement identifies a potential more ideal 'future state' that the system aspires to achieve. Situational analysis follows and analyses the external environment to identify threats and opportunities, then looks inwards to assess the organisation's resources and capabilities.[1-6]
The stage of synthesis follows, in which the strategic plan is crafted. The plan must then be implemented, and after that outcomes must be audited. There are a number of generic strategic planning tools that are of relevance to developing a structured systemic approach to quality improvement programmes. These include the SWOT analysis, the balanced scorecard, and strategic drift and gap analysis.
SWOT
This acronym stands for Strengths, Weaknesses, Opportunities and Threats (SWOT) and identifies internal strengths and weaknesses, and threats and opportunities in the external environment, that may affect the organisation.
The balanced scorecard
The balanced scorecard is a forward-looking management system that views the organisation from four perspectives, namely learning and growth, process, the customer point of view, and results.
Strategic drift and gap analysis
The final outcome of a strategic plan is a result of the interaction of the external environment and three internal factors, namely the plan, the leadership and the culture of the organisation. A gap analysis model helps identify reasons for the strategic gap.
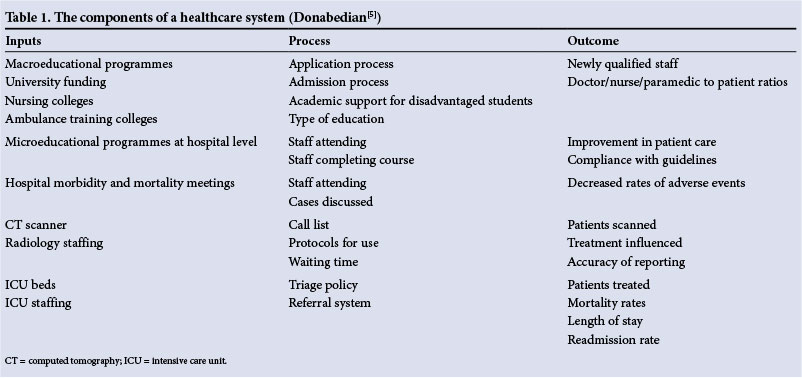
A healthcare system model
There is a well-established model for thinking about healthcare systems (Table 1) that breaks a healthcare system down into inputs, process and outcome.[4,5] Table 1 attempts to give examples of the various constituents of a healthcare system and to categorise them according to which component they reflect. The system comprises two variables and a product of those two variables. Healthcare outcomes are a direct product of the interaction between inputs and processes. The only components of the healthcare system that planners can directly influence are the inputs and the processes. The relationship between inputs and process is not linear, and increasing inputs without altering process will not necessarily improve outputs. Conversely, improving the process of care without increasing the resources available may result in a dramatic improvement in outcomes.
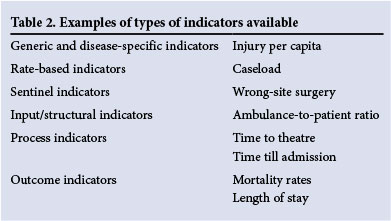
Metrics to measure outcomes of a healthcare system
A good quality indicator provides a platform to improve processes and outcomes and can be classified according to type or according to which component of a healthcare system it measures. Table 2 attempts to contextualise the type of quality indicators against the component of the healthcare system being analysed.[5,6]
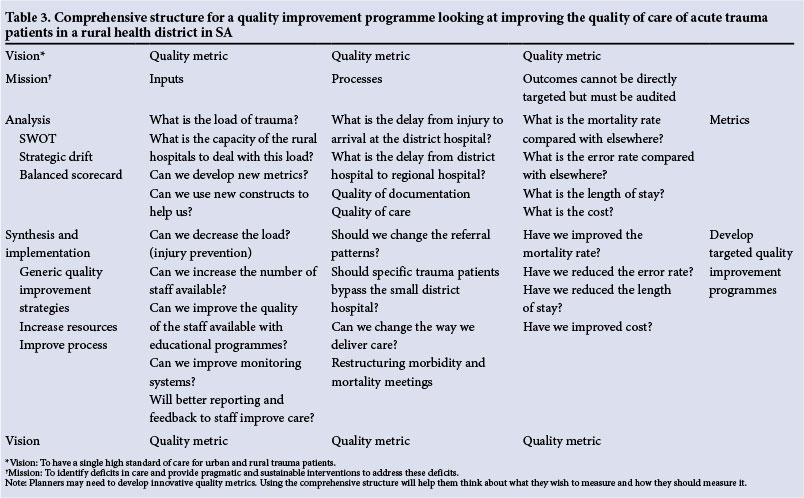
A comprehensive strategic planning structure for healthcare systems
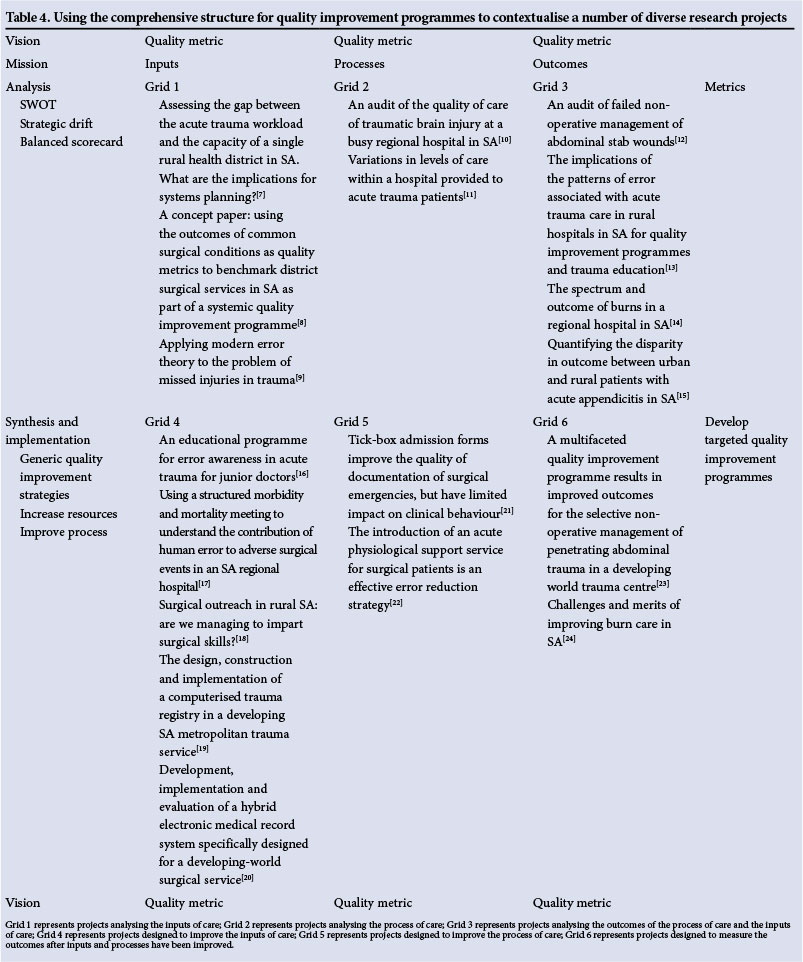
I have developed an overarching structure or grid (Table 3) that allows planners to contextualise the strategic planning process against the various components of the healthcare system, to plan accordingly, and to evaluate improvements over time. It integrates the planning process, the components of the system, and quality metrics. The structure comprises a composite grid with an x axis and a y axis. Along the y axis are the components of the strategic planning process (analysis, synthesis and implementation), and along the x axis are the three components of a healthcare system (inputs, processes, outcomes). Within each cell of the grid there is room for the appropriate strategic planning tool as well as the specific quality improvement intervention, and for the appropriate metric. The model allows a planner to identify each metric according to its role in the strategic planning process and according to the component of the system it is measuring. Above and below the grid are columns for the mission and vision of the organisation. These should inform each grid. Table 3 attempts to show how the grid could be used to situate each tool, intervention or metric according to the stage of the strategic planning process and the component of the healthcare system it is addressing. Planners can situate each planning tool in its appropriate grid. Each proposed intervention can also be placed in a grid according to whichever component of the system it is intended to address. Table 4 illustrates how such a structure may be used in practice to contextualise data from a number of sources in rural trauma and acute care.
Applying the grid to the Pietermaritzburg Metropolitan Trauma Service (PMTS)
Since its inception in 2006, the PMTS in KwaZulu-Natal Province, South Africa (SA), has run a research and a quality improvement programme aimed at uplifting trauma care at Edendale Hospital and in the rural Sisonke health district. This programme is a multifaceted one, as it is obvious that no single intervention will address all the deficits in trauma and acute surgical care in our system. The grid structure has helped to contextualise all programmes within an overarching structure. This is represented in Table 4, which places a number of research projects into context. Commencing by measuring the resources available to deal with trauma and the burden of disease,[7] I then adopted a number of theoretical constructs, taken from fields outside surgery, and used them to both measure quality of care and to inform potential interventions. These theoretical constructs included error theory and the idea of developing a suitable quality marker for surgery.[8,9] These systems were used to assess the quality of care in the area.[10-15]
Once this situational analysis was done, I moved on to the stage of synthesis of strategies and interventions, introducing educational programmes and refinement of morbidity and mortality meetings with the intention of driving quality improvement;[16,17] a number of innovative registries, which allowed us to capture data for research and to quantify the burden of disease and the outcome more accurately;[18,19] use of the data from these registries to further inform morbidity and mortality meetings and educational initiatives; and a surgical outreach programme (that has run for over a decade), designed to uplift surgical care in the rural hospitals of western KwaZulu-Natal.[20]
The grid structure helped in understanding the role of this latter programme and auditing its efficacy in transferring skills to the district hospitals. There are ongoing efforts to refine the process of care by developing burns teams, trauma teams and acute physiological support teams.[21,22] The last introduction was an innovative attempt to provide improved care to surgical patients who were deemed to be too sick for the general ward but too well for the intensive care unit.[22]
Ongoing audit has revealed some successes and some failures.[23,24] The grid enabled contextualisation of each research project and each intervention within the overarching system, and closure of the loop between research and strategy.
Conclusion
I have developed a grid structure that integrates the strategic planning process, the associated strategic planning tools, a model of the healthcare system, and the many quality metrics available to measure components of the system as they relate to acute care. As shown, each step in the strategic planning process and each individual quality metric can be placed within the grid to provide a system-wide overview. I believe that this grid will facilitate the development and implementation of successful quality improvement programmes in a variety of settings in the SA healthcare system.
References
1. Souba WW, Weitekamp MR, Mahon JF. Political strategy, business strategy, and the academic medical center: Linking theory and practice. J Surg Res 2001;100(1):1-10. [http://dx.doi.org/10.1006/jsre.2001.6249] [ Links ]
2. Glickman SW, Bagget KA, Krubert CH, et al. Promoting quality: The health-care organization from a management perspective. Int J Qual Health Care 2007;19(3):341-348. [http://dx.doi.org/10.1093/intqhc/mzm047] [ Links ]
3. Jacobs T, Shepherd J, Johnson G. Strengths, weaknesses, opportunities and threats (SWOT) analysis. In: Ambrosini V, Johnson G, Scholes K, eds. Exploring Techniques of Analysis and Evaluation in Strategic Management. London: Prentice Hall, 1998:122-133. [ Links ]
4. Kaplan RS, Norton DP. The balanced scorecard - measures that drive performance. Harv Bus Rev 1992;70(1):71-79. [ Links ]
5. Donabedian A. The quality of care. How can it be assessed? JAMA 1988;260(12):1743-1748. [http://dx.doi.org/10.1001/jama.260.12.1743] [ Links ]
6. Mainz J. Defining and classifying clinical indicators for quality improvement. Int J Qual Health Care 2003;15(6):523-530. [http://dx.doi.org/10.1093/intqhc/mzg081] [ Links ]
7. Clarke DL, Aldous C, Thomson SR. Assessing the gap between the burden of trauma in Sisonke District and the surgical capacity of the district hospitals: What are the implications for planning? Eur J Trauma Emerg Surg 2014;40(3):303-308. [http://dx.doi.org/10.1007/s00068-013-0369-0] [ Links ]
8. Clarke DL, Gouveia J, Thomson SR, Muckart DJ. Applying modern error theory to the problem of missed injuries in trauma. World J Surg 2008;32(6):1176-1182. [ Links ]
9. Clarke DL, Kong VY, Handley J, Aldous C. A concept paper: Using the outcomes of common surgical conditions as quality metrics to benchmark district surgical services in South Africa as part of a systemic quality improvement programme. S AfT J Surg 2013;51(3):84-86. [http://dx.doi.org/10.7196/SAJS.1476] [ Links ]
10. Alexander T, Fuller G, Hargovan P, Clarke DL, Muckart DJ, Thomson SR. An audit of the quality of care of traumatic brain injury at a busy regional hospital in South Africa. S Afr J Surg 2009;47(4):120-122,124-126. [ Links ]
11. Stewart WW, Farina Z, Clarke DL, Thomson SR. Variations in levels of care within a hospital provided to acute trauma patients. S Afr J Surg 2011;49(4):194-198. [ Links ]
12. Clarke DL, Allorto NL, Thomson SR. An audit of failed non-operative management of abdominal stab wounds. Injury 2010;41(5):488-491. [http://dx.doi.org/10.1016/j.injury.2009.10.022] [ Links ]
13. Clarke DL, Aldous C, Thomson SR. The implications of the patterns of error associated with acute trauma care in rural hospitals in South Africa for quality improvement programs and trauma education. Injury 2013;45(1):285-288. [http://dx.doi.org/10.1016/j.injury.2013.04.011] [ Links ]
14. Allorto NL, Oosthuizen GV, Clarke DL, Muckart DJ. The spectrum and outcome of burns in a regional hospital in South Africa. Burns 2009;35(7):1004-1008. [http://dx.doi.org/10.1016/j.burns.2009.01.004] [ Links ]
15. Kong VY, van der Linde S, Handley J, Aldous C, Clarke DL. Quantifying the disparity in outcome between urban and rural patients with acute appendicitis in South Africa. S Afr Med J 2013;103(10):742-745. [http://dx.doi.org/10.7196/SAMJ.7109] [ Links ]
16. Aldous C, Searle R, Clarke DL. An error awareness program for junior doctors. African Journal of Health Professions Education 2014;6(2):161. [http://dx.doi.org/10.7196/AJHPE.350] [ Links ]
17. Clarke DL, Furlong H, Laing GL, Aldous C, Thomson SR. Using a structured morbidity and mortality meeting to understand the contribution of human error to adverse surgical events in a South African regional hospital. S Afr J Surg 2013;51(4):122-126. [http://dx.doi.org/10.7196/SAJS.1537] [ Links ]
18. Clarke DL, Aldous C. Surgical outreach in rural South Africa: Are we managing to impart surgical skills? S Afr Med J 2013;104(1):57-60. [http://dx.doi.org/10.7196/SAMJ.7252] [ Links ]
19. Laing GL, Bruce JL, Aldous C, Clarke DL. The design, construction and implementation of a computerized trauma registry in a developing South African metropolitan trauma service. Injury 2014;45(1):3-8. [http://dx.doi.org/10.1016/j.injury.2013.05.013] [ Links ]
20. Laing GL, Bruce JL, Skinner DL, Allorto NL, Clarke DL, Aldous C. Development, implementation and evaluation of a hybrid electronic medical record system specifically designed for a developing world surgical service. World J Surg 2014;38(6):1388-1397. [http://dx.doi.org/10.1007/s00268-013-2438-2] [ Links ]
21. Laing GL, Bruce JL, Clarke DL. Tick-box admission forms improve the quality of documentation of surgical emergencies, but have limited impact on clinical behavior. S Afr Med J 2014;104(6):435-438. [http://dx.doi.org/10.7196/SAMJ.7673] [ Links ]
22. Clarke DL, Kong VY, Naidoo LC, Furlong H, Aldous C. The introduction of an acute physiological support service for surgical patients is an effective error reduction strategy. Int J Surg 2013;11(9):989-992. [http://dx.doi.org/10.1016/j.ijsu.2013.06.003] [ Links ]
23. Laing GL, Skinner DL, Bruce JL, Bekker W, Oosthuizen GV, Clarke DL. A multi faceted quality improvement programme results in improved outcomes for the selective non-operative management of penetrating abdominal trauma in a developing world trauma centre. Injury 2014;45(1):327-332. [http://dx.doi.org/10.1016/j.injury.2013.08.021] [ Links ]
24. Allorto N, Clarke DL. Merits and challenges in the development of a dedicated burn service at a regional hospital in South Africa. Published online 20 August 2014. http://dx.doi.org/10.1016/j.burns.2014.07.021 [ Links ]
 Correspondence:
Correspondence:
D L Clarke
damianclar@gmail.com
Accepted 18 August 2014


{kind=link}
{kind=link}
{kind=link}