










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.104 n.10 Pretoria Oct. 2014
RESEARCH
Detecting virological failure in HIV-infected Tanzanian children
E M MgeleaI; R KisengeII; S AboudIII
IMD, MMed. Department of Paediatrics and Child Health, Muhimbili University of Health and Allied Sciences, Dar es Salaam, Tanzania
IIMD, MMed, PhD. Department of Paediatrics and Child Health, Muhimbili University of Health and Allied Sciences, Dar es Salaam, Tanzania
IIIMD, PhD. Department of Microbiology and Immunology, Muhimbili University of Health and Allied Sciences, Dar es Salaam, Tanzania
ABSTRACT
BACKGROUND: The performance of clinical and immunological criteria to predict virological failure in HIV-infected children receiving antiretroviral therapy (ART) is not well documented.
OBJECTIVE: To determine the validity of clinical and immunological monitoring in detecting virological failure in children on ART.
METHODS: A total of 218 children were included in the study. All were from care and treatment clinics in Dar es Salaam, Tanzania. Their mean age was 10.6 years, 122 (56.0%) were males, and the mean time on ART was 40.9 months. The study was conducted from August 2011 to March 2012. Data on sociodemographic and clinical characteristics and immunological and virological failure were based on World Health Organization definitions. Blood samples were collected for CD4+ T-cell count and viral load tests.
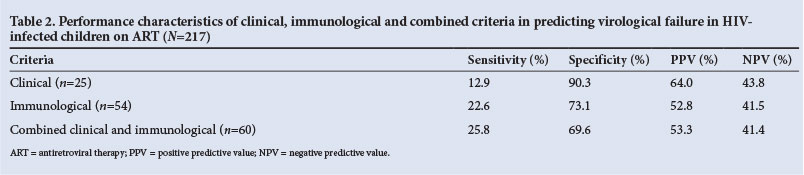
RESULTS: Of 217 children with available viral load results, 124 (57.1%) had virological failure (>400 copies/mL), 25.0% immunological failure and 11.5% clinical failure. The sensitivity, specificity, positive predictive value and negative predictive value of clinical criteria were 12.9%, 90.3%, 64.0% and 43.8%, respectively, those for immunological criteria 22.6%, 73.1%, 53.3% and 41.4%, and those for the combination of clinical and immunological monitoring 25.8%, 69.9%, 53.3% and 41.4%. Children who received nevirapine (NVP)-based regimens were two times more likely (odds ratio 2.0; 95% confidence interval 1.20 - 3.64) to have virological failure than those on efavirenz and protease inhibitor-based regimens.
CONCLUSIONS: The study demonstrated poor performance of currently recommended clinical and immunological criteria for monitoring HIV-infected children on ART. Moreover, children on NVP-based regimens had a higher risk of developing virological failure than those on other regimens.
Globally, it is estimated that 3.4 million children under the age of 15 years are living with HIV and AIDS, the majority residing in sub-Saharan Africa and southern and southeastern Asia.[1] In Tanzania, the exact number infected with HIV is unknown. However, 130 000 - 160 000 children are eligible for antiretroviral therapy (ART).[2] The use of ART in Tanzania increased from <1% of those meeting eligibility criteria in 2004 to 26% in 2012.[3]
The World Health Organization (WHO) advocates a public health approach to ART, recognising the potential role of plasma HIV-1 RNA testing but recommending clinical and immunological monitoring in resource-constrained countries such as Tanzania.[4,5] It has been shown that there are challenges related to the use of clinical and immunological parameters to detect virological failure in adults receiving ART. The delay in recognition may result in increased acquisition of HIV drug-resistant mutations as well as increased morbidity and mortality.[6] However, there may be no clear benefit to routine measurement of viral load to ascertain virological failure in adults.[7] Data on clinical and immunological monitoring to detect virological failure in children are limited. Where methods for detecting virological failure are available, they are not affordable. The aim of the current study was therefore to determine the validity of clinical and immunological monitoring in detecting virological failure among Tanzanian HIV-infected children on ART.
Methods
Study design and population
A cross-sectional, health facility-based study was conducted from August 2011 to March 2012. A total of 218 HIV-infected children on ART were included. All were from care and treatment clinics in Dar es Salaam, the sites involved being Muhimbili National Hospital, Temeke, Amana, Mwananyamala, Infection Disease Control (IDC) and Sinza. The mean age of the children was 10.6 years (range 1 -16), and 122 (56.0%) were males. The mean duration of time on ART was 40.9 months. The cohort group involved those who had been receiving ART for >6 months. Ethical approval was obtained from the Senate Research and Publications Committee of Muhimbili University of Health and Allied Sciences, Dar es Salaam. Written informed consent was obtained from the parents/guardians.
Sociodemographic and clinical characteristics including start date of ART, type of ART regimen, WHO HIV disease stage and incidence of opportunistic infections were recorded. Clinical failure was defined as new or recurrence of WHO HIV disease stage III or IV events after ≥6 months of ART.[2] Immunological failure was defined as a CD4+ count below baseline after at least 6 months of ART or a drop in the CD4+ count to <30% of the peak level. To confirm the clinical and/or immunological failures, virological failure was defined as a viral load >400 copies/mL in children receiving ART for ≥6 months.
CD4+ counts and HIV viral loads
Blood samples were collected for determination of CD4+ T-cell counts (FACSCalibur system, Becton Dickinson, USA) and viral load tests (Roche Cobas Amplicor HIV-1 RNA monitor version 1.5 assay, Roche Diagnostics, USA). The assay detection limit using standard protocol testing was 400 - 750 000 copies/mL, and a viral load <400 copies/mL indicated good response to ART. Testing was performed at the Department of Microbiology and Immunology laboratory, Muhimbili University of Health and Allied Sciences, Dar es Salaam.
Statistical analysis
Data were analysed using the Statistical Package for Social Scientists (SPSS) version 17.0, and sensitivity, specificity and predictive values of clinical and immunological criteria were calculated. Viral load was used as a reference method. The χ2 test was used to assess association between virological failure and clinical and immunological failures, opportunistic infections, ART regimen and WHO HIV disease stage. A p-value of <0.05 was considered statistically significant. Logistic regression analysis was performed to determine the predictors associated with virological failure. Odds ratios (ORs) and 95% confidence intervals (CIs) are presented as the risk estimator.
Results
A total of 218 children on ART were included in the study. Of these, 122 (56.0%) were males. The largest age group was 11 - 15-year-olds (80 children, 36.7%). The mean age for the group as a whole was 10.6 years (range 1 - 16), and the mean duration of time on ART was 40.9 months. One hundred and fifty-three (70.2%) and 53 (23.4%) children were in WHO HIV disease stages III and IV, respectively (Table 1). One hundred and forty-seven (67.4%) were on nevirapine (NVP)-based regimens. Eighty-five (39.0%) had a history of opportunistic infections while on ART. Pulmonary tuberculosis was the most common opportunistic infection reported.

The median viral load was log 3.0. Twenty-five (11.5%) and 54 (25.0%) children had clinical and immunological failures, respectively, and 60 (27.5%) had both clinical and immunological failures. The sensitivity, specificity, positive predictive value (PPV) and negative predictive value of clinical, immunological and combined monitoring are summarised in Table 2. Immunological monitoring had a higher sensitivity (22.6% v. 12.9%) but lower specificity (73.1% v. 90.3%) than clinical criteria. Combined clinical and immunological criteria had higher sensitivity but lower specificity in detecting virological failure (Table 2).
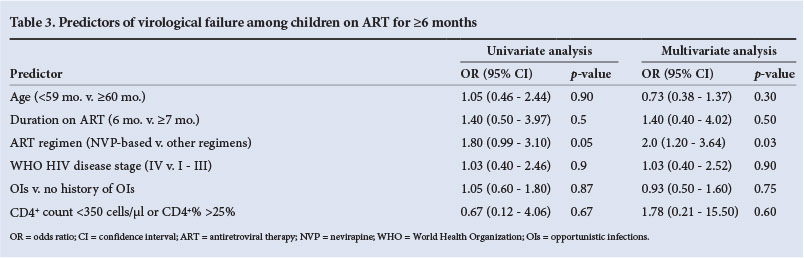
To assess the association of certain immunological and clinical variables with virological failure in this cohort, we performed univariate and multivariate analysis. The use of NVP was a predictor for virological failure (Table 3), showing a two times higher risk than other regimens (OR 2.0; 95% CI 1.20 - 3.64; p=0.03).
Discussion
Proper monitoring of children on ART is key to preventing emergence of HIV drug resistance, but it can be challenging in resource-limited settings. In this study, we showed that the proportion of children on ART with virological failure was highest, followed by immunological and clinical failure. Clinical and immunological criteria showed poor sensitivity and specificity for detection of virological failure in children on ART, and all the children had a detectable viral load despite being on ART for ≥6 months (the defined period for viral suppression to an undetectable level). NVP-based regimens were independent significant predictors of virological failure in children on ART.
The rate of virological failure in this study was high (57%) compared with those reported in previous studies: 20% in Thailand,® 26% in Uganda,[9] 32% in the Kilimanjaro region, Tanzania,![10] and 50% in Cote d'Ivoire.[11] The differences observed between the current and previous studies could be explained by the different viral load cut-off points used, e.g. >1 000 copies/mL to indicate virological failure was used in the Thailand study. The Uganda study was a prospective cohort study as opposed to our cross-sectional study, which could have resulted in closer medical attention and monitoring of participants. However, the participants in the two studies were of similar ages.
Some of reasons for the low sensitivity of immunological criteria for virological failure in HIV-infected children on ART have been found to be opportunistic infections, individual variation, and evidence that HIV-specific CD4+ T cells increase when the viral load increases.[121 Immunological criteria were two times more sensitive than clinical criteria in the current and previous studies, supporting the concept that immunological failure occurs earlier than clinical failure.[13] When a combination of clinical and immunological criteria was used, the sensitivity and specificity to predict virological failure were 25.8% and 69.9%, respectively. The combination of clinical and immunological criteria therefore had higher sensitivity but relatively low specificity in predicting virological failure, i.e. the combination of the two criteria offers a better chance of predicting virological failure than a single criterion, but at the expense of lower specificity.
Our findings are in agreement with those of previous studies conducted elsewhere. In a prospective cohort study of children aged <16 years in South Africa by Davies et al.,!14] the sensitivity of immunological criteria was 10.0%, with a PPV of 42.0%, and immunological criteria were therefore unable to identify children on ART who were failing virologically. A study to determine the performance of combined clinical and immunological criteria by Lynen et al.[15] showed that combining clinical and immunological criteria resulted in sensitivity of 29 - 33%, which is comparable to the current study findings. A recent study from Thailand by Bunupuradah et al.[16] examining the accuracy of immunological failure in predicting virological failure in HIV-infected children on first-line ART showed that immunological failure had a sensitivity of 20.4% and specificity of 93.9% in predicting the virological failure, comparable to our study.
Our study and previous studies from Uganda and Thailand,!8,91 showed that children on NVP-based regimens were more likely to have virological failure than those on efavirenz and protease inhibitor-based regimens. In the current study, more than two-thirds of the children received NVP-based regimens. There is evidence that use of single-dose NVP prophylaxis during labour leads to selection of NVP-resistant strains.[17] Pre-exposure of children to NVP via their mothers as part of prevention of mother-to-child transmission of HIV may have predisposed to drug resistance and therefore virological failure; however, we did not examine this effect. Furthermore, in the current study most children received an NVP-based regimen. Since it was a cross-sectional study, it was not possible to establish the trend of viral suppression and viral rebound occurring over a period of time. In addition, since viral load assessment is not a routine investigation in resource-limited settings such as ours, baseline viral load samples were not available for testing in this study.
In conclusion, we showed that the proportion of virological failure was the highest (57.1%), followed by immunological (25.0%) and clinical failure (11.5%). Children who were on NVP-based regimens had a higher risk of developing virological failure than those on other regimens. The study demonstrated poor performance of currently recommended clinical and immunological criteria to monitor HIV-infected children on ART. Expanding access to viral load testing may improve outcomes for children on ART in Tanzania and help doctors make informed decisions on treating HIV-infected children.
Acknowledgements. We thank the parents/guardians of the HIV-infected children on ART for consenting to participate in the study. Sincere thanks to Fauster Mgaya, Betty Mchaki and Theofrida Tembo for sample processing and testing in the lab. Special thanks to the Muhimbili University of Health and Allied Sciences, Dr Guerino Chalamila and Prof. Sylvia Kaaya of Management and Development for Health, and Prof. Ferdinand Mugusi (International Clinical, Operational and Health Sciences Research Training Award) for their technical and financial support of this valuable work.
References
1. UNAIDS. Aids Epidemic Update. November 2010. http://www.unaids.org/documents/20101123_GlobalReport_em.pdf (accessed 1 September 2014). [ Links ]
2. World Health Organization. Antiretroviral Therapy of HIV Infection in Infants and Children: Towards Universal Access: Recommendations for a Public Health Approach - 2010 Revision. Geneva: World Health Organization, 2010. http://www.who.int/hiv/pub/guidelines/art/en/ (accessed 1 September 2014). [ Links ]
3. World Health Organization/UNICEF/UNAIDS. Global Update on HIV Treatment 2013: Results,Impact and Opportunities, Geneva: WHO, 2013. http://www.unaids.org/en/media/unaids/contentassets/documents/unaidspublication/2013/20130630_treatment_report_en.pdf (accessed 1 September 2014). [ Links ]
4. Kawo G, Kalokola F, Fataki M, et al. Prevalence of HIV type 1 infection, associated clinical features and mortality among hospitalized children in Dar es Salaam, Tanzania. Scand J Infect Dis 2000;32(4):357-363. [http://dx.doi.org/10.1080/003655400750044917] [ Links ]
5. UNAIDS. Epidemiological fact sheet on HIV and AIDS: United Republic of Tanzania. 2009. http://data.unaids.org/pub/report/2009/jc1700_epi_update_2009_en.pdf (accessed 1 September 2014). [ Links ]
6. World Health Organization. Antiretroviral Therapy for HIV Infection in Infants and Children: Towards Universal Access. 2009. www.who.int/hiv/pub/paediatric/paed-prelim-summary.pdf (accessed 1 September 2014). [ Links ]
7. Meya D, Spacek LA, Tibenderana H, et al. Development and evaluation of a clinical algorithm to monitor patients on antiretrovirals in resource-limited settings using adherence, clinical and CD4 cell count criteria. J Int AIDS Soc 2009;12:3. [http://dx.doi.org/10.1186/1758-2652-12-3] [ Links ]
8. Jittamala PPT, Chaiinseeard S, Sirisanthana V, et al. Predictors of virologic failure and genotypic resistance mutation patterns in Thai children receiving non-nucleoside reverse transcriptase inhibitor-based antiretroviral therapy. Pediatr Infect Dis J 2009;28(9):826-830. [http://dx.doi.org/10.1097/INF.0b013e3181a458f9] [ Links ]
9. Kamya MR, Mayanja-Kizza H, Kambugu A, et al. Predictors of long-term viral failure among Ugandan children and adults treated with antiretroviral therapy. J Acquir Immune Defic Syndr 2007;46(2):187-193. [http://dx.doi.org/10.1097/QAI.0b013e31814278c0] [ Links ]
10. Emmett SD, Cunningham CK, Mmbaga BT, et al. Predicting virologic failure among HIV-1-infected children receiving antiretroviral therapy in Tanzania: A cross-sectional study. J Acquir Immune Defic Syndr 2010;54(4):368-375. [http://dx.doi.org/10.1097/QAI.0b013e3181cf4882] [ Links ]
11. Fassinou PEN, Rouet F, Laguide R, et al. Highly active antiretroviral therapies among HIV-1-infected children in Abidjan, Cote d'Ivoire. AIDS 2004;18(14):1905-1913. [http://dx.doi.org/10.1097/00002030-200409240-00006] [ Links ]
12. Scott ZA, Beaumier CM, Sharkey M, et al. HIV-1 replication increases HIV-specific CD4+ T cell frequencies but limits proliferative capacity in chronically infected children. J Immunol 2003;170(11S):5786-5792. [http://dx.doi.org/10.4049/jimmunol.170.11.5786] [ Links ]
13. Aldous JL, Haubrich RH. Defining treatment failure in resource-rich settings. Curr Opin HIV AIDS 2009;4(6):459-466. [http://dx.doi.org/10.1097/COH.0b013e328331dea5] [ Links ]
14. Davies MA, Boulle A, Eley B, et al. Accuracy of immunological criteria for identifying virological failure in children on antiretroviral therapy. Trop Med Int Health 2011;16(11):1367-1371. [http://dx.doi.org/10.1111/j.1365-3156.2011.02854.x] [ Links ]
15. Lynen L, van Griensven J, Elliott J. Monitoring for treatment failure in patients on first-line antiretroviral treatment in resource-constrained settings. Curr Opin HIV AIDS 2010;5(1):1-5. [http://dx.doi.org/10.1097/COH.0b013e3283333762] [ Links ]
16. Bunupuradah T, Puthanakit T, Kosalaraksa P, et al Immunologic and virologic failure after first-line NNRTI-based antiretroviral therapy in Thai HIV-infected children. AIDS Res Ther 2011;8:40. [http://dx.doi.org/10.1186/1742-6405-8-40] [ Links ]
17. Cunningham CK, Dorenbaum A, Mofenson L, Culnane M, Sullivan JL, and the PACTG 316 Team. Genotypic resistance analysis in women participating in PACTG 316 with HIV-1 RNA >400 copies/ml. Presented at the 8th Conference on Retroviruses and Opportunistic Infections, 4-8 February 2001, Chicago, USA. [ Links ]
 Correspondence:
Correspondence:
E M Mgelea
(drmgelea@gmail.com)
Accepted 26 June 2014


{kind=link}
{kind=link}