










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.104 n.6 Pretoria Jun. 2014
RESEARCH
Identification of a common founder couple for 40 South African Afrikaner families with Parkinson's disease
G GeldenhuysI; B GlanzmannII; D LombardIII; S BoolayIV; J CarrV; S BardienIV
IPhD.Division of Applied Mathematics, Department of Mathematical Sciences, Faculty of Science, Stellenbosch University, Stellenbosch, South Africa
IIMSc. Division of Molecular Biology and Human Genetics, Faculty of Medicine and Health Sciences, Stellenbosch University, Tygerberg, South Africa
IIIBCur. Division of Neurology, Faculty of Medicine and Health Sciences, Stellenbosch University, Tygerberg, South Africa
IVPhD. Division of Molecular Biology and Human Genetics, Faculty of Medicine and Health Sciences, Stellenbosch University, Tygerberg, South Africa
VMB ChB, PhD. Division of Neurology, Faculty of Medicine and Health Sciences, Stellenbosch University, Tygerberg, South Africa
ABSTRACT
BACKGROUND: Afrikaners are a unique ethnic group in South Africa (SA) with well-documented ancestral records spanning a period of over 350 years. They are mainly descended from Dutch, German and French settlers to SA in the 17th and 18th centuries. Today several disorders in this population occur at relatively high frequencies as a result of founder effects.
OBJECTIVE: To determine whether a founder effect for Parkinson's disease (PD) is present in the Afrikaner population.
METHODS: Study participants were recruited from the Movement Disorders Clinic at Tygerberg Hospital in Cape Town, SA, and from support groups of the Parkinson's Association of South Africa. Standard methods for genealogical research in SA on hereditary diseases were used including interviews and searches in sources such as state archives, the Huguenot Museum in Franschhoek, marriage and baptismal records, and tombstone inscriptions.
RESULTS: For 40 of the PD families, there was only a single most recent ancestral couple common to all of the families. On average there are between three and four ancestral lines to the founder couple per proband (range 1 -14).
CONCLUSION: If genetic studies confirm the presence of a founder effect for PD in Afrikaners, this would imply that there is a large number of individuals from this ethnic group who may potentially be at risk of developing this debilitating condition. This study illustrates and reinforces the concept that genealogical analysis is a powerful tool for identification of founder effects for various disorders in the Afrikaner population.
Afrikaners in South Africa (SA) are a recognisable group with a relatively small gene pool and excellent family records over a period of >350 years. The foundations of this group were laid mainly from 1652 until 1807. Afrikaners are derived from settlers from The Netherlands (roughly one-third), Germany (slightly less than one-third) and France (roughly one-quarter), with smaller contributions from other countries, imported slaves and indigenous peoples,[1] the exact proportions differing for each present-day Afrikaner. To illustrate this, a 'deconstruction' of one specific Afrikaner individual who has an incomplete ancestral chart of 926 individuals shows contributions of 37.5% from The Netherlands, 27.4% from Germany and 26.4% from France in his make-up, with 2.2% from people 'van die Kaap' ('from the Cape', an expression which usually refers to female slaves born in the Cape), 1.9% from Britain and the rest from other countries.[2] There could be a perception that in isolated areas such as the Gamkaskloof more frequent intermarriages might have had an influence on the occurrence of hereditary diseases. However, there is no clear evidence that the people in these areas differed significantly from those in less isolated rural Afrikaner communities.[3]
Several disorders among Afrikaners occur at relatively high frequencies due to founder effects.[3,4] A founder effect results when a small subset of a large population establishes a new population. The new population may differ significantly from the original population, both in terms of its genotypes and phenotypes. In the case of Afrikaners, the disorders that occur at an unusually high frequency may indicate that the original Dutch, French and German colonists who settled in the Cape carried those disease-causing genes at high frequency. In some cases the diseases can be traced back to specific founder couples, e.g. for familial colonic polyposis,[4,5] porphyria variegata,[6] progressive familial heart block,[7] Huntington's disease (HD),[8] osteogenesis imperfecta,[9] pseudoxanthoma elasticum (PXE),[10] schizophrenia,[11] long QT syndrome[12,13] and Fanconi's anaemia.[14]
Given the evidence of founder effects for other disorders in the Afrikaner population, we sought to determine whether a founder effect for Parkinson's disease (PD) also occurs in this population. PD is a debilitating neurodegenerative condition arising as a result of the progressive loss of dopaminergic neurons in the brainstem associated with proteinaceous inclusions termed Lewy bodies. Cardinal clinical features include resting tremor, rigidity, bradykinesia, postural instability and responsiveness to levodopa. A genetic aetiology has been found in ~10 - 15% of PD cases and a number of genes (and corresponding proteins) have been implicated, including parkin, PINK1 (PTEN-induced putative kinase 1), DJ-1 (DJ-1), SNCA (α-synuclein), LRRK2 (leucine-rich repeat kinase 2), VPS35 (vacuolar protein sorting 35) and EIF4G1 (eukaryotic translation initiation factor 4 γ1).
For the genetic forms of PD, both autosomal dominant (AD) and autosomal recessive (AR) patterns of inheritance are evident. Our research team has been investigating the genetic causes of PD in local SA populations since 2007. Noting that a significant proportion of our PD patients were self-identified as Afrikaner, we undertook a genealogical study to investigate the presence of a possible founder effect for PD.
Methods
Study participants were recruited from the Movement Disorders Clinic at Tygerberg Hospital in Cape Town, SA, and from various support group meetings around SA of the Parkinson's Association of South Africa. All study participants gave written informed consent. When the genealogical study was started in June 2009, 193 PD probands had been recruited, and of these approximately one-third (62/193; 32.1%) were self-identified as Afrikaner. Afrikaner probands were selected for further genealogical analysis on the basis of having a young age at onset of PD (mostly <60 years) and a positive family history of the condition (at least one first-, second- or third-degree relative presenting with similar symptoms).
By February 2013, 48 Afrikaner families had been investigated and for each of these a proband was chosen for whom an ancestral chart was drawn. Methods that have become standard in SA genealogical research on hereditary diseases were used.[11,13] These include interviews with probands and their relatives, and searches in various sources such as state archives, the Huguenot Museum in Franschhoek, marriage and baptismal records, death notices, published genealogies, tombstone inscriptions, voters' rolls, telephone directories and the internet. It is well known that the three mainstream Afrikaans churches, the Nederduitse Gereformeerde Kerk, the Gereformeerde Kerk and the Nederduitsch Hervormde Kerk van Afrika, keep detailed records of marriages and baptisms. Many of these records are available in film or microfiche form at the Genealogical Institute of South Africa in Stellenbosch.
Results
In the initial stages of the research the ancestral charts were drawn as completely as possible. For most of the families, their ancestors can be traced back for at least eight generations. A single ancestral chart for one proband could therefore contain at least 511 individuals, corresponding to the eight generations ancestral to the proband.
After the genealogical trees of the first 12 families were constructed, it emerged that there was a single ancestral couple common to these families. This couple (couple A) married in SA in 1668. The husband was born in The Netherlands and came to SA in 1661. The wife was born in Germany in 1655, and she and her parents came to SA in the late 1650s.
For the remaining families, the genealogical research concentrated on finding at least one line of descent from couple A to the proband. For 40 of the PD probands, at least one such line of descent was found that confirmed ancestry to couple A. On average, there are between three and four ancestral lines for each PD proband, ranging from a minimum of one line to a maximum of 14 lines. From a genealogical viewpoint this is strong evidence of a possible founder effect for PD, with couple A as the founder couple. For the remaining 8/48 families investigated, the information provided was insufficient to determine their ancestry for more than three or four generations, and their relationship to the founder couple is therefore unknown.
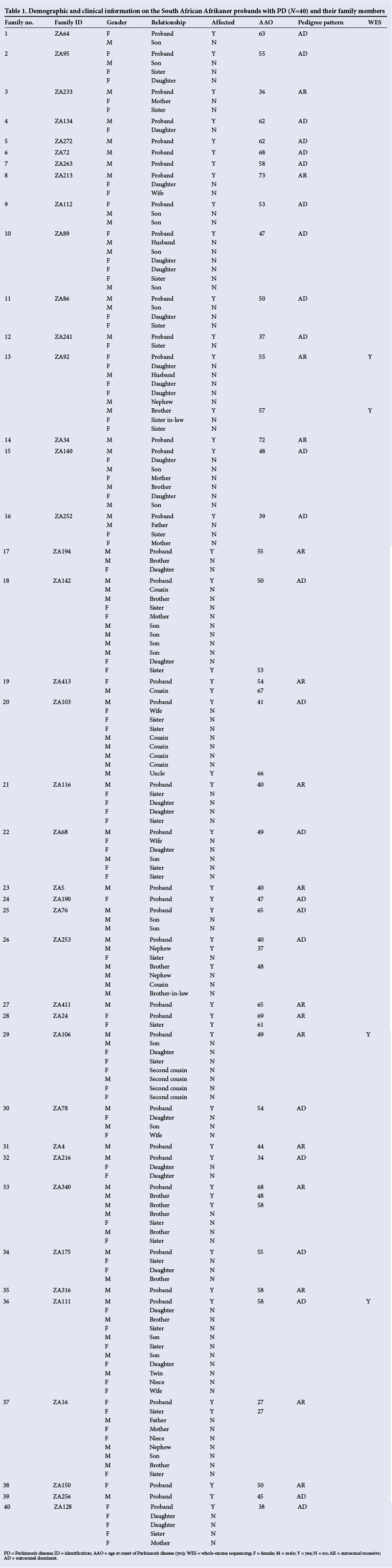
Selected lines of descent from the founder couple to the 40 probands are shown in Fig. 1. Although couple A had 12 children, the pedigree shows only the five children for whom there are lines of descent to the PD patients in this study. It should be noted that since a single proband may have many different ancestral lines to the founder couple, this diagram may potentially be drawn in many different ways. A summary of the available demographic and clinical information for these 40 families is provided in Table 1. In these families, both AD and AR patterns of inheritance are evident, based on currently available information. Also, it is plausible that reduced penetrance and marriage to spouses with a family history of PD could influence the pattern of inheritance observed within specific families.
Discussion
In the present study, we were able to show that 40 Afrikaner PD probands are descended from a common founder couple. After this couple was identified in the first 12 families examined, links to the couple could also be established in an additional 28 families in which there was sufficient genealogical information to trace ancestry.
Since some progenitors of Afrikaners, e.g. the Van der Merwe and Ferreira progenitors, have large numbers of present-day descendants it has been suggested that any two present-day Afrikaners might share these progenitors as ancestors.[2] However, this proposal appears not to be correct. In our database there are only two lines of descent from the Ferreira progenitor, and both are linked to the same proband. To put our results in perspective, these genealogical findings were compared with other genealogical data that we have available on Afrikaners for long QT syndrome.[12] Of the 22 families who were shown to share a founder couple for this disorder, 12 complete and ten partial ancestral charts were drawn. In the 12 complete ancestral charts only four were found with ancestral lines to couple A.
Given that the total number of male and female progenitors for the Afrikaner population for the period from 1657 until 1806 was ~4 000,[15] the probability that any randomly selected group of 40 Afrikaners would share a common founder couple appears to be remote. We conclude that it is unlikely that couple A's relationship to our 40 families is a chance finding, and that couple A is likely to be the founder couple for PD in the present-day Afrikaner population.
Notably, couple A has also been referred to as the founder couple for HD, lipoid proteinosis, PXE and schizophrenia in the Afrikaner population.[2] However, this statement can be questioned by referring to the original published literature for each of these disorders. In the case of HD, it is actually the eldest daughter of couple A who was shown to be the founder mother of this disorder in SA.[8] With regard to lipoid proteinosis, a study conducted in the Namaqualand region of SA proposed that a brother and his sister who were born early in the 18th century are the common ancestors of present-day lipoid proteinosis patients.[16] This implies that it is the siblings' parents, and not couple A, who are the founder couple of lipoid proteinosis. For the recessive condition PXE, genetic analysis of the families identified three mutations that are associated with distinct haplotypes. This suggests that these families are derived from at least three founder couples, one of these being couple A.[10,17] With regard to schizophrenia, 87 affected individuals have been shown to be linked to a single founder couple,[11] but there is no documented evidence that couple A is the founder couple.
We acknowledge that to confirm our hypothesis of a founder effect for PD in SA, identification of the underlying genetic cause is needed. To this end, high-density genome-wide single-nucleotide polymorphism genotyping will be used to provide additional support for the genealogical data. It has previously been shown that distantly related affected individuals who share the same causal mutation will also share large genomic regions surrounding it.[18] Moreover, 3/40 probands and one affected sibling (from families labelled ZA92, ZA106 and ZA111) (Table 1) have been selected for whole-exome sequencing (WES), a technique that involves the screening of all coding regions of the genome for pathogenic mutations. The WES data are in the process of being analysed using bioinformatics analysis and genetic studies to identify the causative mutation in these families.
There is evidence for the presence of founder effects for PD in a number of different populations, including the North African Arab, Basque and Ashkenazi Jewish populations. In the North African Arab population upwards of 30% of PD patients have been shown to harbour the LRRK2 G2019S mutation, and all these individuals share a common haplotype.[19] This same mutation is also present at a relatively high frequency (~20%) in Ashkenazi Jews, implicating a founder effect for the mutation which occurred in the Near East at least 4 000 years ago.[20] In Norway, G2019S mutation carriers could be traced back 10 generations to a common Norwegian ancestor couple living between 1580 and 1650.[21] Similarly, the LRRK2 R1441G mutation has been found in ~20% of familial PD patients from the Basque ethnic group but is rare outside Spain, and it is hypothesised that this mutation originated in the Basque population in about the 7th century.[22]
If genetic studies confirm the presence of a founder effect for PD in Afrikaners, this would imply that there is a large number of individuals from this ethnic group who may potentially be at risk of developing this debilitating condition. It is therefore imperative to identify the underlying causative mutations to be able to offer the options of pre-symptomatic and carrier testing with the appropriate genetic counselling to these individuals. In conclusion, given the extent and depth of ancestral information that is available on Afrikaners, genealogical analysis is a powerful tool for identification of genetic founder effects for various disorders in this particular population.
Acknowledgements. We thank the patients and their families for their participation in this study; without their willing assistance this research would not have been possible. We acknowledge the Harry Crossley Foundation, the South African Medical Research Council and Stellenbosch University for financial support.
References
1. De Bruyn GFC. [Die samestelling van die AfTikanervolk]. Tydskrifvir Geesteswetenskappe 1976;15:39-42. [ Links ]
2. Greeff JM. Deconstructing Jaco: Genetic heritage of an Afrikaner. Ann Hum Genet 2007;71(5):674-688. [http://dx.doi.org/10.1111/j.1469-1809.2007.00363.x] [ Links ]
3. Botha MC, Beighton P. Inherited disorders in the Afrikaner population of southern Africa, Part II. Skeletal, dermal and haematological conditions; the Afrikaners of Gamkaskloof; demographic considerations. S Afr Med J 1983;64(17):664-667. [ Links ]
4. Botha MC, Beighton P. Inherited disorders in the Afrikaner population of southern Africa, Part I. Historical and demographic background, cardiovascular, neurological, metabolical and intestinal conditions. S Afr Med J 1983;64(16):609-612. [ Links ]
5. Louw JH, Torrington M. Familial polyposis of the colon: A condition illustrating the importance of genealogy in medicine. Familia 1968;5:42-47. [ Links ]
6. Dean G. The Porphyrias: A Study of Inheritance and Environment. 2nd ed. London: Pitman, 1971. [ Links ]
7. Brink AJ, Torrington M. Progressive familial heart block - two types. S Afr Med J 1977;52(2):53-59. [ Links ]
8. Hayden MR, Hopkins HC, Macrae M, Beighton PH. The origin of Huntington's chorea in the Afrikaner population of South Africa. S Afr Med J 1980;58(5):197-200. [ Links ]
9. Knoll DP, de Vries WN, de Wet WJ. [Genealogie van 'n familie met osteogenesis imperfecta: Die stamregister van Pieter Willem Adriaan Piek]. Familia 1988;25:46-64. [ Links ]
10. Le Saux O, Beck K, Sachsinger C, et al Evidence for a founder effect for pseudoxanthoma elasticum in the Afrikaner population of South Africa. Hum Genet 2002;111(4-5):331-338. [http://dx.doi.org/10.1007/s00439-002-0808-1] [ Links ]
11. Karayiorgou M, Torrington M, Abecasis GR, et al. Phenotypic characterization and genealogical tracing in an Afrikaner schizophrenia database. Am J Med Genet B Neuropsychiatr Genet 2004;124B(1):20-28. [http://dx.doi.org/10.1002/ajmg.b.20090] [ Links ]
12. Brink PA, Criotti L, Corfield V, et al. Phenotypic variability and unusual clinical severity of congenital long QT Syndrome in a founder population. Circulation 2005;112(17):2602-2610. [http://dx.doi.org/10.1161/CIRCULATIONAHA.105.572453] [ Links ]
13. Geldenhuys G. [Genealogiese navorsing oor die lang QT sindroom.] Capensis 3 2009:14-29. [ Links ]
14. Tipping AJ, Pearson T, Morgan NV, et al. Molecular and genealogical evidence for a founder effect in Fanconi anemia families of the Afrikaner population of South Africa. Proc Natl Acad Sci USA 2001;98(10):5734-5739. [http://dx.doi.org/10.1073/pnas.091402398] [ Links ]
15. Heese JA. [Die Herkoms van die Afrikaner 1657-1867.] Kaapstad: AA Balkema, 1971. [ Links ]
16. Van Hougenhouck-Tulleken W, Chan I, Hamada T, et al. Clinical and molecular characterization of lipoid proteinosis in Namaqualand, South Africa. Br J Dermatol 2004;151(2):413-423. [http://dx.doi.org/10.1111/j.1365-2133.2004.06076.x] [ Links ]
17. Torrington M, Viljoen DL. Founder effect in 20 Afrikaner kindreds with pseudoxanthoma elasticum. S Afr Med J 1991;79(1):7-11. [ Links ]
18. Van der Zwaag PA, van Tintelen JP, Gerbens F, et al. Haplotype sharing test maps genes for familial cardiomyopathies. Clin Genet 2011;79(5):459-467. [http://dx.doi.org/10.1111/j.1399-0004.2010.01472.x] [ Links ]
19. Benamer HT, de Silva R LRRK2 G2019S in the North African population: A review. Eur Neurol 2010;63(6):321-325. [http://dx.doi.org/10.1159/000279653] [ Links ]
20. Lesage S, Patin E, Condroyer C et al; French Parkinson's Disease Genetics Study Group. Parkinson's disease-related LRRK2 G2019S mutation results from independent mutational events in humans. Hum Mol Genet 2010;19(10):1998-2004. [http://dx.doi.org/10.1093/hmg/ddq081] [ Links ]
21. Johansen KK, Hasselberg K, White LR, Farrer MJ, Aasly JO. Genealogical studies in LRRK2-associated Parkinson's disease in central Norway. Parkinsonism Relat Disord 2010;16(8):527-530. [http://dx.doi.org/10.1016/j.parkreldis.2010.05.005] [ Links ]
22. Mata IF, Hutter CM, González-Fernández MC, et al. Lrrk2 R1441G-related Parkinson's disease: Evidence of a common founding event in the seventh century in Northern Spain. Neurogenetics 2009;10(4):347-353. [http://dx.doi.org/10.1007/s10048-009-0187-z] [ Links ]
 Correspondence:
Correspondence:
S Bardien
(sbardien@sun.ac.za)
Accepted 26 February 2014.


{kind=link}
{kind=link}