










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSAMJ: South African Medical Journal
versión On-line ISSN 2078-5135
versión impresa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.104 no.5 Pretoria may. 2014
CONTINUING MEDICAL EDUCATION
ARTICLE
Down-staging of breast cancer in the pre-screening era: Experiences from Chris Hani Baragwanath Academic Hospital, Soweto, South Africa
N MuruganI; C DickensII; P PisaIII; V McCormackII; M JoffeIV; J JacobsonV; H CubaschI
IMB ChB, FCS (SA). Breast Unit, Department of Surgery, Chris Hani Baragwanath Academic Hospital, Soweto, South Africa
IIPhD. Section of Environment and Radiation, International Agency for Research on Cancer, Lyon, France
IIIPhD. MRC/Wits Developmental Pathways for Health Research Unit, Department of Paediatrics, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IVPhD. Breast Unit, Department of Surgery, Chris Hani Baragwanath Academic Hospital, Soweto, South Africa
VMBA, PhD. Department of Epidemiology, Mailman School of Public Health, Columbia University, New York, USA
ABSTRACT
We aimed to investigate the stage of breast cancer at first diagnosis and assess possible determinants of late-stage presentation. A consecutive series of women with newly diagnosed breast cancer at Chris Hani Baragwanath Academic Hospital (CHBAH), Soweto, South Africa were analysed. We retrospectively reviewed electronic patient records. Data were extracted for: (i) stage and year at diagnosis; (ii) travel distance (estimated straight-line distance from GPS-coded residential address to CHBAH); (iii) receptor subtypes; and (iv) age of patient. Generalised linear models were applied to estimate risk ratios for late- v. early-stage disease.
Of the patients (N=1 071) studied, the mean age was 55 years and 90% were black Africans. Patients who lived >20 km from the hospital (n=347; 61.8%) presented with late-stage disease (stage 3/4) compared with 50.2% who lived <20 km from the hospital (n=724; p=0.02). The majority of patients (74%) >70 years of age who lived >20 km away presented with advanced breast cancer. However, in younger patients, age showed no clear association with stage at presentation. Travel distance was an important predictor of later-stage disease at diagnosis, which was more noticeable in elderly patients. Patients with more aggressive triple-negative and HER2+ tumours presented with later-stage disease.
The incidence and mortality rates of breast cancer in Africa have risen rapidly in recent years.[1] Women in sub-Saharan Africa (SSA) have some of the lowest incidence rates of breast cancer worldwide. However, the disproportionately high mortality rate reflects the poor survival in these developing countries.[1,2] A significant contributor to the observed poor survival rates seems to be an advanced stage of disease at first diagnosis. Predictive factors may include a lack of early detection programmes, poor healthcare infrastructure and suboptimal availability of and adherence to timely treatment.
Population growth alone will lead to an estimated 119 918 new cases of breast cancer by 2030 in SSA.[2] The changing reproductive choices of African women, particularly the postponement of child bearing and prolonged birth intervals, represent a shift towards increased breast cancer profiles and an overall burden of disease.[2] We aimed to investigate the stage of breast cancer at first diagnosis and assessed possible determinants of late-stage presentation.
Methods
Setting and patients
Chris Hani Baragwanath Academic Hospital (CHBAH), the largest public tertiary referral hospital in South Africa, has a catchment area of ~3 million people from Soweto and a surrounding region of 60 km. The hospital's Batho Pele Breast Unit, a member of the International Breast Centres Network, has grown steadily since its inception in 2000. Approximately 600 outpatients visit the unit per month, with up to 25 new breast cancer cases being diagnosed. In 2006, an electronic clinical data system was established to facilitate oncological decision making for newly diagnosed patients. For the purpose of this study, retrospective data of consecutively diagnosed women from October 2006 to January 2012 were analysed. The stage and year at diagnosis (primary tumour (T), regional lymph nodes (N), distant metastasis (M) (TNM) staging was converted to Manchester staging) were documented. In our breast unit, the majority of patients do not undergo routine mammographic screening and are symptomatic at diagnosis. Patients receive standard diagnostic and multimodality treatment with surgery, chemotherapy, radiotherapy, and hormonal blockade in keeping with international guidelines. Treatment decisions are taken by a multidisciplinary team of surgeons, radiologists, medical oncologists, radiation oncologists and palliative care physicians.
Statistical analysis
Possible contributing factors to stage at diagnosis were assessed using general linear models (GLMs). Factors such as age, race, distance to central hospital and tumour receptor subtype were treated as independent variables. Stage at diagnosis was the dependent variable. GLMs were utilised to estimate the risk ratios for late- v. early-stage disease.
Results
Table 1 shows the comprehensive characteristics of breast cancer patients diagnosed at CHBAH during October 2006 - January 2012.

A total of 1 071 patients were included in this analysis. Ninety per cent were black African women and their mean age ± SD at diagnosis was 55.4±14.3 years. Overall, 54% of patients presented with late-stage disease (stage 3/4).
The travel distance was calculated as the shortest straight-line distance from the patient's reported residential address to CHBAH using GPS-coded co-ordinates. Of the patients, 45% and 95% resided within 10 km and 50 km of the hospital, respectively. Most patients lived in Soweto, an average travelling distance of 7.5±4.0 km, with residence clusters near Katlehong (23.9±4.0 km), Orange Farm and Sebokeng (28.5±6.0 km) and Vanderbijlpark (47.5±2.7 km) (Fig. 1).
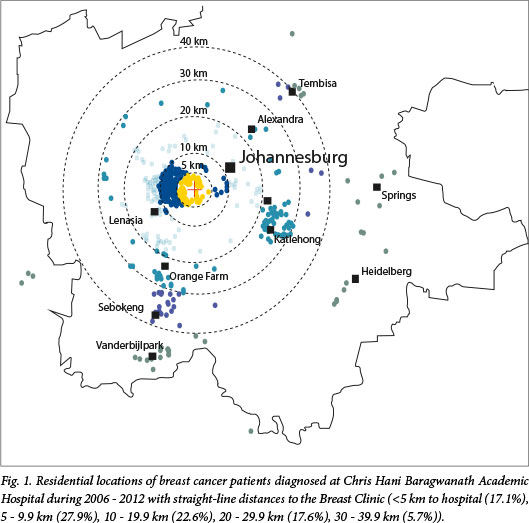
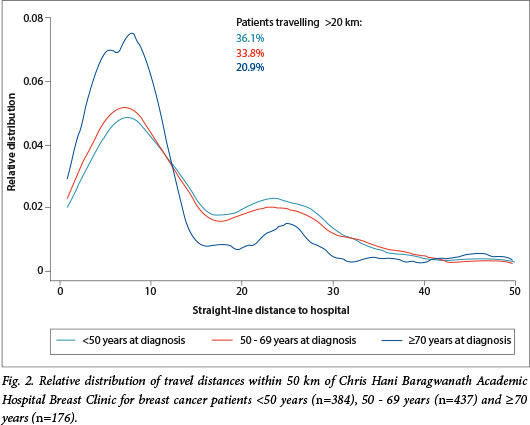
Of the patients who lived >20 km from the hospital, 347 (61.8%) presented with late-stage disease (stage 3/4) compared with 724 (50.2%) who lived within 20 km (p=0.02).[3] Advanced stage at diagnosis was particularly common (74%) in patients >70 years living >20 km away. Notably, there were few elderly patients >70 years from distances >20 km in this series. This could indicate that these especially vulnerable patients cannot reach the hospital. The relative distribution of travel distances within 50 km of CHBAH Breast Clinic for breast cancer patients <50 years (n=384), 50 - 69 years (n=437) and >70 years (n=176) are shown in Fig. 2.
In this series, 67% of tumours were oestrogen- and/or progesterone-positive, with only 21% being of the poorer prognosis triple-negative subtype. As expected, patients with more aggressive triple-negative and HER2+ tumours presented with later-stage disease (Fig. 3).

The majority of patients were referred by primary healthcare clinics, with an estimated 18% being self-referrals. There was an encouraging down-staging of disease (i.e. diagnosis at an earlier stage) observed when stage at diagnosis was plotted against year at diagnosis. From 2008 onwards, compared with baseline 2006 - 2007 data, the proportion of late-stage disease decreased from 71% to 48% (Fig. 4).

No significant correlation between stage and age was observed, with the exception of the very old who presented with more advanced disease (Fig. 5).

Discussion
The current study investigated stage of breast cancer at initial diagnosis and assessed the possible determinants of late-stage presentation. The main findings showed that among the 1 071 patients analysed the mean age was 55 years and 90% were black Africans. Of the patients who lived >20 km from the hospital, 347 (61.8%) presented with late-stage disease (stage 3/4) compared with 50.2% who lived <20 km from the hospital (n=724; p=0.02). The majority of patients >70 years (74%) who lived >20 km away, presented with advanced breast cancer. We assume that many elderly patients cannot reach the hospital.
Stage at diagnosis, particularly in developing countries, is a strong predictor of breast cancer survival,[3] and understanding the determinants of delay in diagnosis is essential for controlling this increasing burden. The current study provides evidence for the potential down-staging of breast cancer in a South African peri-urban setting in the absence of population-wide mammographic screening. The observed decline in the proportion of late-stage breast cancer over this 5-year period suggests that down-staging was observed in the absence of routine screening, probably owing to improved access and heightened awareness.
South Africa is undergoing rapid transition characterised by a high prevalence of HIV infection and the emergence of non-communicable diseases, including cancer. The majority of patients cannot afford private medical care and are treated in the state healthcare system, making them vulnerable to all the failings of the existing infrastructure. The journey of a woman with breast cancer in South Africa varies greatly from patient to patient. Typically, in the public sector, it involves the woman noticing symptoms and taking the initiative to seek help in the healthcare system. She often has to navigate past multiple healthcare levels before reaching a histological diagnosis and receiving definitive care.
CHBAH is a tertiary-level public sector hospital and, as such, is the third tier in the hierarchy of the healthcare system. Primary healthcare clinics and local general practitioners are usually the first tier of this referral structure, followed by secondary level district hospitals.[4] Some patients (18% in this study) choose to bypass the system and present themselves directly to hospital, facilitated by the fact that the Breast Clinic at CHBAH is a walk-in clinic.
Delays in reaching CHBAH may be due to patient and health-system factors. At the patient level, personal (awareness) and sociocultural and economic factors may lead to delays. Our study showed that a travel distance >20 km from the Breast Clinic was a significant predictor of the stage of disease at first presentation. Distance-associated hurdles adversely affected older patients. For patients who had to travel greater distances, the financial burden associated with travelling to hospital represented a significant barrier to optimal care.[5] The minimum weekly wage for an average domestic worker in South Africa is approximately R320. A round trip to hospital may consume 5 - 14% of a woman's weekly income, before loss of working hours is taken into account. In addition, many of these women have responsibilities as primary family caregivers and therefore have to make arrangements for child/grandchild minding prior to clinic or hospital visits.
Increased travel distance is also likely to affect the post-diagnosis experience of a breast cancer patient as it may influence treatment access and compliance. Repeated cycles of chemotherapy, radiotherapy and post-surgical follow-up visits invariably have a significant financial impact on the patient, and travel-associated barriers may increase as the patient becomes weaker.
Another notable finding was that 66.6% of the patients were diagnosed with oestrogen and/or progesterone receptor-positive tumours, with only 21.5% of cancers being triple-negative. The predominance of these luminal A and B tumours, with a better prognosis, and the strong down-staging trend observed over the study period, suggest that late-stage diagnosis in similar settings is driven to a greater extent by non-biological determinants rather than by an aggressive, rapidly growing tumour.
It is important to acknowledge the socio-cultural factors and personal barriers to presentation, especially when considering the proximally located patients with more immediate access to CHBAH, who presented with advanced disease. Understanding the underlying causes of these additional barriers is essential if there is to be a feasible possibility of initiating improved strategies. Lack of education, lack of knowledge of symptoms, lack of breast awareness, fear of treatment and cultural beliefs may all be detrimental contributing factors in our setting. There might also be an inherent distrust of conventional western treatment thought to interfere with indigenous remedies. Additionally, primary healthcare facilities are generally perceived as having long waiting times, ineffective service and inexperienced staff.
In conclusion, breast awareness in general has significantly increased in the past few years, with various media campaigns with regard to breast cancer, including walkathons and articles in women's magazines. This may partly account for breast cancer down-staging in the absence of population-wide routine mammographic screening. In addition, the CHBAH Breast Unit is easily accessible, with an open-door walk-in policy. Understanding the various factors that contribute to diagnostic delay is particularly relevant in the South African public healthcare sector and may enable interventions, ensuring that more cancers are diagnosed at an earlier stage and improved survival.
References
1. Sankaranarayanan R, Swaminathan R, Lucas EB, eds. Cancer Survival in Africa, Asia, the Caribbean, and Central America. Lyon, France: International Association of Cancer Registries, 2011:305. [ Links ]
2. Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer 2010;127(12):2893-2917. [http://dx.doi.org/10.1002/ijc.25516] [ Links ]
3. Dickens C, Joffe M, Jacobson J, et al. Diagnostic delays and residential distance to hospital in a periurban South African setting. Int J Cancer (submitted). [ Links ]
4. Jemal A, Bray F, Forman D, et al. Cancer burden in Africa and opportunities for prevention. Cancer 2012;118:4372-4384. [http://dx.doi.org/10.1002/cncr.27410] [ Links ]
5. Wright SV An investigation into the causes of absconding among black African breast cancer patients. S Afr Med J 1997;87:1540-1543. [ Links ]
 Corresponding author:
Corresponding author:
N Murugan
(nivs6ster@gmail.com)

