










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSAMJ: South African Medical Journal
versión On-line ISSN 2078-5135
versión impresa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.104 no.3 Pretoria mar. 2014
FORUM
CLINICAL PRACTICE
Clinical Access to Bedaquiline Programme for the treatment of drug-resistant tuberculosis
F ConradieI; G MeintjesII; J HughesIII; G MaartensIV; H FerreiraV; S SiwenduVI; I MasterVII; N NdjekaVIII
IFrancesca Conradie is a researcher at the School of Clinical Medicine, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IIGraeme Meintjes is Associate Professor at the Institute of Infectious Disease and Molecular Medicine and Department of Medicine, University of Cape Town, South Africa
IIIJennifer Hughes is a medical officer for Médecins Sans Frontières, Khayelitsha, Cape Town, South Africa
IVGary Maartens is Head of the Division of Clinical Pharmacology, Department of Medicine, University of Cape Town, South Africa
VHannetjie Ferreira is a medical officer at the MDR/XDR TB Unit, Klerksdorp/Tshepong Complex, North West Province, South Africa
VISweetness Siwendu is a medical officer at Metro TB Hospital Complex at Brooklyn Chest Hospital, Cape Town, South Africa
VIIDr Iqbal Master is a clinical manager at the MDR TB Unit, King Dinuzulu Hospital Complex, Durban, South Africa
VIIINorbert Ndjeka is Director of the Drug-Resistant TB, TB & HIV, National TB Control & Management, National Department of Health, South Africa
ABSTRACT
While clinical disease caused by drug-sensitive Mycobacterium tuberculosis (MTB) can usually be treated successfully, clinical disease caused by drug-insensitive MTB is associated with a poorer prognosis. In December 2012, a new drug, bedaquiline, was approved by the US Food and Drug Administration. This article documents the process whereby the National Department of Health, Right to Care and Médecins Sans Frontières obtained access to this medication for South Africans who might benefit from subsequent implementation of the Clinical Access to Bedaquiline Programme.
While clinical disease caused by drug-sensitive Mycobacterium tuberculosis (MTB) can usually be treated successfully, clinical disease caused by drug-insensitive MTB is associated with a poorer prognosis. In December 2012, a new drug, bedaquiline, was approved by the US Food and Drug Administration (FDA) for the treatment of multidrug-resistant (MDR) tuberculosis (TB). In a review paper, the four goals of a compassionate use/early access programme for new TB drugs are outlined: to protect patients; to minimise the risk of treatment failure and emergence of resistance; to exercise fairness; and to comply with regulatory guidance.[1] This article documents the process whereby the National Department of Health (NDoH), Right to Care (a US Agency for International Development-funded non-governmental organisation) and Médecins Sans Frontières (MSF) obtained access to this medication for South Africans who might benefit from subsequent implementation of the Clinical Access to Bedaquiline Programme (CAP). Attention was paid to the regulatory framework, fairness and protection of patients while being cognisant of the need to prevent emergence of resistance to bedaquiline.
Setting
In South Africa (SA), 14 161 cases of MDR-TB were documented in 2012. The proportion of MDR-TB cases with additional resistance to a quinolone and a second-line injectable, i.e. extensively drug resistant TB (XDR-TB), is estimated at 10.9% (N=1 545)[2] with an ill-defined proportion being 'pre-XDR-TB', i.e. MDR with resistance to either a quinolone or a second-line injectable. While the outcomes of patients with pre-XDR-TB have not been well documented, the outcomes of XDR-TB are poor. In a retrospective cohort study at four designated XDR-TB provincial treatment facilities in SA between August 2002 and February 2008, 195 adult patients with culture-proven XDR-TB were analysed; 21 patients died before initiation of any treatment, 174 patients (82 with HIV infection) were treated, and 62 (36%) patients died during follow-up. Sputum culture conversion was achieved in only 33/174 (19%) patients.[3]
There are several new classes of TB drugs becoming available, including bedaquiline, which is a diarylquinoline. Bedaquiline offers a new mechanism of anti-TB action by specifically inhibiting mycobacterial adenosine triphosphate synthase.[4] In December 2012, the FDA granted accelerated approval for bedaquiline based on two phase 2 studies involving 440 people with drug-resistant TB (DR-TB). The first trial was a randomised, double-blind, placebo-controlled trial with bedaquiline and an optimised background regimen. The second was an open-label trial. Bedaquiline, when given with other existing MDR-TB drugs, increased the proportion of people whose sputum cultures converted to negative after 2 and 6 months of treatment. Bedaquiline, when given with other existing MDR-TB drugs, also reduced the time to sputum culture conversion, offering the possibility of a shorter treatment duration in the future. Bedaquiline is currently only commercially available in the US and is not yet registered by the SA Medicines Control Council (MCC). In the interim, some patients with few other treatment options, and before the drug's approval in their countries, have been offered bedaquiline through an early access programme put in place by the manufacturer, Janssen Pharmaceutica.
Under controlled compassionate use programmes and early access trials, several countries including SA have made bedaquiline available for patients with XDR- or pre-XDR-TB. In an expanded access programme (EAP) model, a clinician requests a drug for a named individual patient based on a specific clinical access guidance document. In an EAP, patients can be enrolled and offered access to the medication if they meet specific eligibility criteria. Based on this model, MDR-TB patients who have limited treatment options have been allowed access to bedaquiline as part of an individually tailored treatment regimen in a CAP in SA.
Key aspects of the CAP
Exercise of fairness
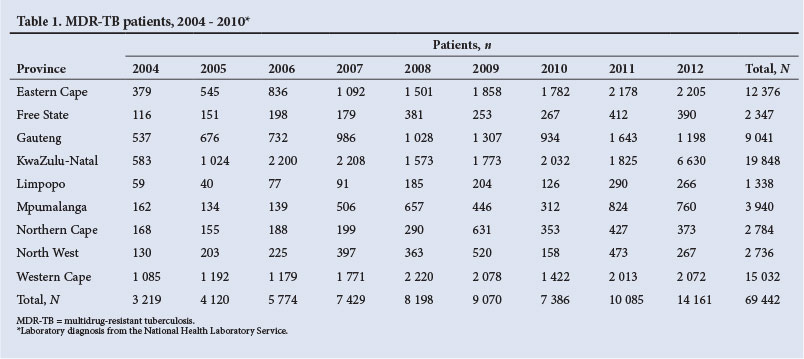
SA has nine provinces, all having MDR-/XDR-TB treatment facilities but with differing MDR-/XDR-TB burdens (Table 1). According to the National Health Laboratory Service, in KwaZulu-Natal, 11 393 diagnoses of MDR-TB were made between 2004 and 2010 and in the same time period 782 diagnoses were made in Limpopo.
To ensure equitable access to bedaquiline by selected XDR- or pre-XDR-TB patients, there should ideally be a clinical site in each province offering the programme.
Initially, four sites were approved by the MCC to begin the programme, based on results of clinical research. However, this excluded other, less well-resourced provinces. Additional sites in all the remaining provinces have since been identified for expansion of the project.
To prepare all future sites, good clinical practice training was provided to at least two members of staff from the selected MDR-/ XDR-TB facilities. Strict adherence to the guidance document was stressed as the newer sites were not all experienced in conducting research. Once trained, the TB directorate of the NDoH set up an official start-up meeting at each of the sites.
Protection of patients
The principle underpinning protection of participating patients is their ability and capacity to make autonomous decisions and to give informed consent. Both the CAP and the informed consent document were approved by each site's research ethics committee prior to the start of the programme and enrolment of participants.
A potential safety risk identified in the development of bedaquiline, in common with moxifloxacin and clofazimine that are included in MDR-TB treatment regimens, was the prolongation of the QTc interval on electrocardiogram (ECG) with associated risks of life-threatening ventricular arrhythmias and sudden death. Thus, built into the CAP is rigorous ECG monitoring with only sites capable of adhering to this being permitted to enrol patients.
Regulatory guidance
Clinical research sites that were involved in the phase 2 clinical trials of bedaquiline were approached first to implement a compassionate use programme for bedaquiline. A requirement to participate was that the patients who accessed the drug were treated within the national TB programme, thus ensuring that the new drug is supported by other quality assured and approved second-line TB drugs.
In November 2011, the compassionate use programme was presented to the MCC by the MDR-TB directorate of the NDoH. The MCC was concerned at that time that the drug was not registered by any other regulatory authorities. They requested that the protocol be amended and implemented as a clinical trial, with appropriate safety monitoring, and with the TB directorate of the NDoH being responsible for sponsorship.
In collaboration with Right to Care and MSF, a CAP for SA was drafted by the NDoH based on the compassionate use framework. In December 2012, the CAP was approved by the MCC.
Minimise the risk of treatment failure
Bedaquiline is a new TB drug with a novel mode of action. The old adage of never adding a single drug to a failing regimen is important to reduce the risk of developing acquired resistance. An SA clinical advisory committee was therefore established, comprising a number of experts in the treatment of MDR-/XDR-TB. This virtual committee operates by e-mail consensus, with all new cases being discussed, and three members, other than the proposing responsible clinician, approving the use of bedaquiline as part of an appropriate regimen. Regimens for individual patients accessing bedaquiline through the programme are individualised and tailored according to the patient's TB susceptibility pattern, treatment history and exposure to other TB drugs, and other individual factors. Key roles of the committee are to ensure that bedaquiline is used only when other TB drugs known to be effective, or are likely to be effective, are available to be used in the patient's regimen. The committee advises on an optimal treatment regimen for each case.
Once approval from the local team is obtained, the responsible physician submits a patient summary to the Janssen Global Programme Manager who then co-ordinates clinical approval by Janssen, at the hands of a panel of clinical experts, and communicates the decision back to the responsible physician for each site. In parallel, approval is obtained from the MCC on a Section 21 or named-patient basis.
Discussion
This initiative has had a number of far-reaching consequences. Firstly, patients with DR-TB that has a poor prognosis are being offered expedited access to a novel drug in a safe and controlled environment. Secondly, the model that has been established may prove useful in the future for other new TB agents.
While much public attention has been paid to MDR-TB in the last 5 years, it remains under-researched. The programme has expanded the capacity for research that does not exist currently in most MDR-TB facilities.
It bears noting that evidence for the regimen used in the current national TB treatment programme is based on expert opinion and not on clinical trial data. Cohort data from Van Deun et al.[5]demonstrated the efficacy of a seven-drug combination, 9-month course of treatment for MDR-TB. This so called 'Bangladesh' regimen consists of high-dose isoniazid, high-dose gatifloxacin, kanamycin, prothionamide, ethambutol, pyrazinamide and clofazimine given for only 9 months and is now being compared with the standard 18 - 24-month regimen in The Evaluation of a Standardised Treatment Regimen of Anti-Tuberculosis Drugs for Patients with Multidrug-Resistant Tuberculosis (STREAM), an International Union Against Tuberculosis and Lung Disease sponsored, non-inferiority clinical trial. This is the first of a number of trials aimed at establishing more effective, safer and shorter MDR-TB regimens using newly available drugs. The CAP in SA has provided the initial training and back-up for such clinical trials in the future.
Finally, HIV co-infection with TB is very common in SA. National HIV guidelines mandate the expedited initiation of antiretroviral therapy in any patient with MDR-/XDR-TB. Data on concomitant antiretroviral use with bedaquiline will emerge following imple-menation of the programme.
Conclusion
There remains much work to be done to find a new effective, safe and evidence-based treatment regimen for MDR-/XDR-TB. Bedaquiline must form part of a long-term strategy aimed at combatting DR-TB. Other drugs that might include linezolid - an oxazalidinone that is also used for the treatment of resistant Gram-positive infections -and clofazimine - a drug used for the treatment of leprosy - must be added to develop regimens for the treatment of XDR- and pre-XDR-TB. The CAP in SA has resulted in both access to treatment with a novel drug for patients with DR-TB and enhancement of research capacity.
1. Horsburgh CR, Haxaire-Theeuwes M, Wingfield C, et al. Compassionate use of and expanded access to new drugs for drug-resistant tuberculosis. Int J Tuberc Lung Dis 2013;17(2):146-152. [http://dx.doi.org/10.5588/ijtld.12.0017] [ Links ]
2. World Health Organization. Global Tuberculosis Report 2013. Geneva: WHO, 2013. http://www.who.int/tb/publications/global_report/en/ (accessed 10 July 2013). [ Links ]
3. Dheda K, Shean K, Zumla A, et al. Early treatment outcomes and HIV status of patients with extensively drug-resistant tuberculosis in South Africa: A retrospective cohort study. Lancet 2010;375(9728):1798-1807. [http://dx.doi.org/10.1016/S0140-6736(10)60492-8] [ Links ]
4. Diacon AH, Pym AS, Grobusch M, et al. The diarylquinolone TMC 207 for the treatment of multidrug-resistant tuberculosis. N Engl J Med 2009;369(23):2397-2405. [http://dx.doi.org/10.1056/NEJMoa0808427] [ Links ]
5. Van Deun A, Maug AK, Salim MA, et al. Short, highly effective, and inexpensive standardized treatment of multidrug-resistant tuberculosis. Am J Respir Crit Care Med 2010;182(5):684-692. [http://dx.doi.org/10.1164/rccm.201001- 0077OC] [ Links ]
 Corresponding author:
Corresponding author:
F Conradie
(fconradie@witshealth.co.za)
Accepted 19 July 2013.


{kind=link}