










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSAMJ: South African Medical Journal
versión On-line ISSN 2078-5135
versión impresa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.104 no.2 Pretoria feb. 2014
RESEARCH
Attitudes to organ donation among some urban South African populations remain unchanged: A cross-sectional study (1993 - 2013)
H R EtheredgeI; R E TurnerII; D KahnIII
IMSc (Med); Health Communication Research Unit, University of the Witwatersrand, Johannesburg, South Africa
IIMSc (Nursing); Department of Nursing, Faculty of Medicine and Health Sciences, Stellenbosch University, Parow, Cape Town, South Africa
IIIMB ChB, FCS (SA), ChM; Department of Surgery, Faculty of Health Sciences, University of Cape Town, South Africa
ABSTRACT
BACKGROUND: A 1993 paper in the SAMJ suggested that public attitudes to organ donation in South Africa were positive. However, statistics reveal a decline in the annual number of transplants in this country.
OBJECTIVE: To repeat the 1993 survey as far as possible and determine whether public attitudes to organ donation in some South African populations have changed over the past 20 years.
METHODS: The 1993 study was replicated in 2012 to generate a current data set. This was compared with the raw data from the 1993 study, and an analysis of percentages was used to determine variations.
RESULTS: Generally attitudes to organ donation have not changed since 1993, remaining positive among the study population. However, individuals are significantly more hesitant to consider donating the organs of a relative without being aware of that person's donation preference. Individuals in the black African study population are currently more willing to donate kidneys than in 1993 (66% v. 81%; p<0.0001), but less willing to donate a heart (64% v. 38%; p<0.0001), a liver (40% v. 34%; p<0.036) and corneas (22% v. 15%, p<0.0059).
CONCLUSIONS: Publicity campaigns aimed at raising awareness of organ donation should emphasise the importance of sharing donation preferences with one's family in order to mitigate discomfort about making a decision on behalf of another. These campaigns should be culturally and linguistically sensitive. The study should be repeated in all populations over time to continually gauge attitudes.
Transplantation is available in almost all major centres around the world. The principles are fairly standardised and outcomes are generally good. Transplantation is currently considered the treatment of choice for most patients with end stage organ failure. South Africa (SA) has an established track record in transplantation, as well as a network of active transplant programmes.[1]
One of the major challenges in transplantation, both internationally and locally, is the shortage of donor organs. Several factors are thought to contribute to this problem in SA, including lack of public awareness about organ donation. Numerous strategies have been employed in an attempt to address this problem. These include promotions and advertising in the lay media and education programmes in schools and other institutions.[1] Despite these efforts, the overall number of transplants performed each year has decreased.[1] Of particular concern is a decrease in the consent rate among families of brain-dead potential donors, from 55% in 1991 to 50% in 2001 and 32% in 2011.[2]
The question arises whether the decline in the consent rate for organ donation is related to changes in the attitudes of the general public towards transplantation. In a 1993 survey,[3] the majority of the study population expressed a willingness to donate both their own organs and the organs of a family member after death, should the circumstances arise.
The aim of the present study was to repeat the 1993 survey as far as possible to ascertain whether public attitudes to organ donation in certain sectors of SA have changed. A cross-sectional study design and statistical analysis were employed.
Historical background
Before 1994, segregation and discrimination on the basis of ethnicity in SA were widespread. Since then, several basic characteristics of SA have changed.[4] These changes pose challenges for time-based replication studies, the present study included. The 1993 study (hereafter referred to as study 1) forms the baseline data for the current analysis. It surveyed the attitudes of two SA populations, black African and white, to organ transplantation.[3] Individuals of Indian, Asian or mixed race origin were not included. At the time of study 1, political segregation in the country provided a unique opportunity to explore the views of two distinct socioeconomic groups within a single demographic area. The white group represented a developed population, while the black African group represented developing-world views.[4]
The 2012 study (hereafter referred to as study 2), which forms the comparison data set, was drawn from a representative sample of the SA urban population. It pays heed to population diversity, with sample size and demographics calculated according to census data. Study 2 is therefore not subject to the limitations of study 1. It is estimated that 21% of individuals living in urban areas are members of a medical scheme and accessing healthcare in the private sector, which is comparable to healthcare in developed countries.[5] The remainder (79%) access healthcare in the state-run public sector, which provides services more similar to those of developing countries. These figures can be extrapolated to the study 2 population. The views of the study population reported in study 2 therefore also represent both a First-World and a developing-world perspective on attitudes toward organ donation, albeit through a different stratification of variables.
Methods
The research was approved by the human research ethics committees of the University of the Witwatersrand (M120532), the University of Cape Town (309/2012) and Stellenbosch University (WITS 2).
Study 1
Data for study 1 were obtained during a collection period from 1987 to 1990. A quantitative methodology was employed. A structured, interviewer-administered questionnaire was utilised to measure attitudes among a sample of 2 125 South Africans. The sample was derived from both urban and rural areas, and only black African and white individuals were invited to participate. The fieldwork was undertaken by TNS, a market research company, as part of a larger general market research survey. TNS fieldworkers were trained by one of the researchers and supervised by field managers. Individuals were approached to participate on a 'door-to-door' basis. All the questionnaires were anonymous, and the nature of the fieldwork process ensured that no individual participant could be identified. Age, gender, race, first language, geographical region and economic status were recorded for each participant.
The questions asked of participants were:
- Would you accept an organ for transplant if you needed one?
- Would you be willing to have your own organs donated to other people after you die if circumstances allow it?
- If a close family member had a fatal accident, would you be willing to donate his or her organs if circumstances allow it?
- Which organs would you be willing to donate (heart, lungs, liver, kidney, pancreas, cornea)?
Study 2
Data for study 2 were obtained in 2012. The same market research company conducted the fieldwork. Techniques used were identical to those of study 1, with the exception of sampling. Study 2 comprised a representative sample of 1 048 adults in the five major SA metropolitan areas. Metropolitan areas are typically wealthier than rural areas, and they are also home to a large migrant workforce from the rest of the country and further afield.[6] Written informed consent was obtained from all participants once they had agreed to take part and before administration of the questionnaire. All the questionnaires were anonymous, and the nature of the fieldwork process ensured that no individual participant could be identified.
Data were captured, cleaned and converted into SPSS format by TNS. The data were- analysed using SAS version 9.3.7. [7] Data from study 1 were compared with those from study 2 using an analysis of percentages. Only data from the black African and white population groups were used for the comparison, as there were no data for the other groups in study 1. Furthermore, a large body of literature suggests that attitudes towards organ donation differ according to ethnic classification, and owing to data coding in the first study, this was the only way to compare the two data sets.
Study population
Figs 1 and 2 illustrate the demographics of the samples from the two studies. Although there were differences across samples, these were not deemed to be significant and a comparison was still possible.


Results
There were 2 125 participants in study 1 compared with 1 048 in study 2. In the black-African cohort, the gender, age, language and regional distributions were similar across the studies. In the white cohort, there were relatively more females, more English-speaking respondents and more respondents from Gauteng in study 1.
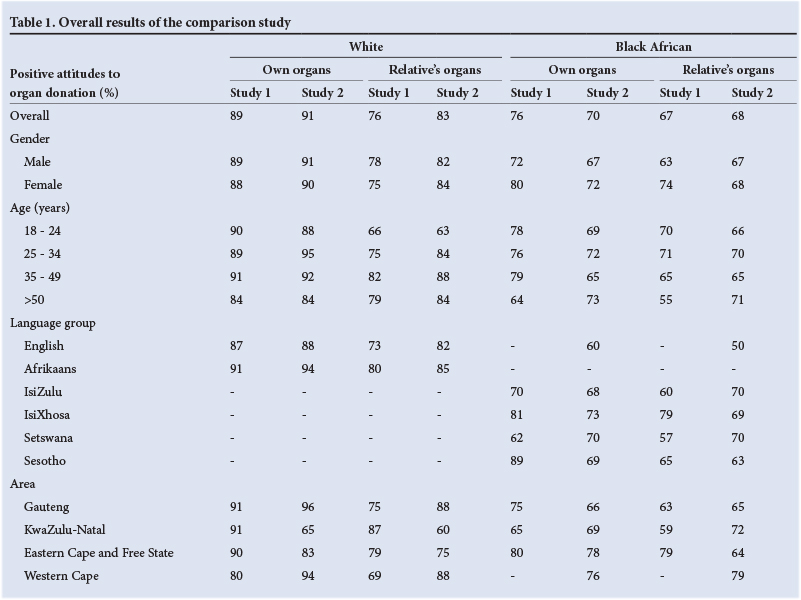
Across the two samples, the majority of respondents held positive views about organ donation. Most (70 - 91%) appeared willing to potentially donate their own organs (Table 1). Many (67 - 83%) also expressed willingness to donate the organs of a relative. It appeared that these attitudes had remained largely unchanged over the past two decades.
Across the two studies, there was no difference between male and female respondents with regard to willingness to have their own organs donated and to donate the organs of a relative (Table 1).
Among white respondents, age did not influence willingness to donate their own organs or to donate the organs of a relative. This was consistent across both studies. However, among black African respondents, older respondents (>50 years) were more willing to donate the organs of a relative in study 2 than in study 1 (71% v. 55%; p=0.049) (Table 1).
There were some differences in attitudes towards organ donation in terms of language (Table 1). Black African IsiZulu-speaking participants were more willing to donate the organs of a relative in study 2 than in study 1 (70% v. 60%; p<0.0001). In contrast, black African IsiXhosa-speaking respondents were less willing to donate the organs of a relative in study 2 (69% v. 79%; p=0.026). There were no significant differences in attitudes towards organ donation in English-and Afrikaans-speaking respondents between the two studies.
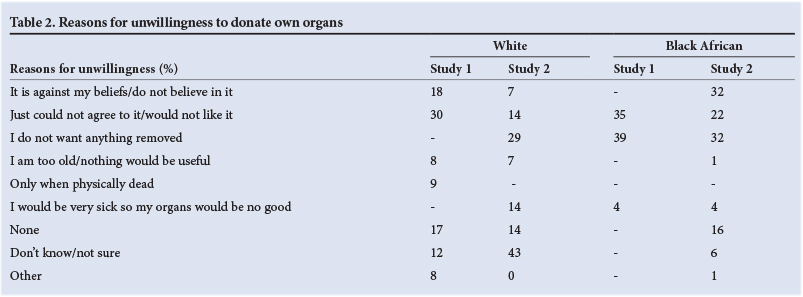
Overall, 11% of white respondents and 24% of black African respondents in study 1 indicated that they would be unwilling to donate their own organs, compared with 9% and 30%, respectively, in study 2. The reasons for unwillingness are shown in Table 2, and included 'it is against my beliefs', 'just could not agree to it', and 'I do not want anything removed'.
Overall, 23% of white respondents and 32% of black African respondents in study 1 expressed an unwillingness to donate the organs of a relative, compared with 17% and 31%, respectively, in study 2 (Table 1). These differences are not significant. The respondents who indicated unwillingness to donate the organs of a relative were asked why this was the case (Table 3). In study 1, 24% of the white respondents and 29% of the black African respondents indicated that 'it is not up to me to decide', 'it is not my responsibility', or 'it is not my body'. In study 2 this reasoning increased to 60% for the white respondents (p<0.0001) and to 41% for the black African respondents (p<0.0001). Religious or cultural beliefs were also cited to a greater extent by the black African respondents in study 2 (9% v. 28%; p<0.001). Black African respondents were also concerned about keeping the body intact after death, with 12% of the respondents in study 1 feeling uneasy about the perceived damage to the body, compared with 22% in study 2 (p=0.0056). One per cent of the white respondents in study 1 reasoned that the relative 'might not like to be an organ donor', and this increased to 20% in study 2 (p<0.0001). Many white respondents (44%) in study 2 indicated that the wishes of the deceased were very important. This increased from 17% in study 1 (p=0.003).
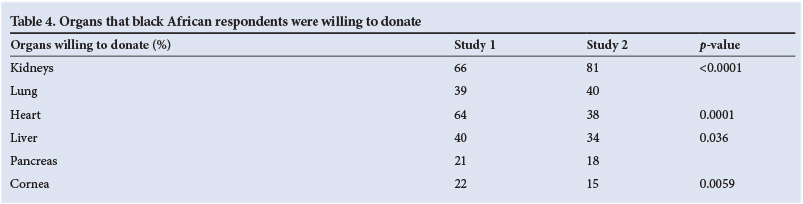
Black African respondents were more willing to donate kidneys in study 2 (66% v. 81%; p<0.0001), but less willing to donate a heart (64% v. 38%; p<0.0001), a liver (40% v. 34%; p<0.036) and corneas (22% v. 15%; p<0.0059) (Table 4).
Discussion
Evidentially, there is no significant difference in expressed attitudes of the study populations towards organ donation over the period analysed. Study 2 reveals that the majority of the population studied still felt positive, with many respondents willing to donate their own organs and those of a relative should circumstances allow. Although it cannot be formally analysed, it appears that the white population is still more willing to donate organs, their own and those of a relative, than the black African population. This may be because the white cohort is better informed and educated than their black African counterparts, despite rapid urbanisation since democracy in 1994.[8] We noted some changes with regard to donating the organs of relatives. All participants appeared as willing to donate the organs- of relatives in study 2 as they were in study 1. However, across the two studies there were notable changes in the justifications for unwillingness to do so. Members of both the black African and the white populations expressed reluctance to make a decision on behalf of another person. In both populations, this sentiment was expressed significantly more often in study 2. There are several hypothetical explanations for this shift in reasoning. For instance, a better educated and more rights-aware population may prize autonomy and free agency more than their counterparts in study 1. [9] This is especially relevant in the healthcare context, where patient-centred care has overtaken a more traditional, paternalistic approach.[10] The decision to donate organs on another's behalf may therefore seem objectionable. Another possibility is that migration and immigration have broken down familial proximity, and thus traditional lines of communication,[9] so individuals are not as familiar with the sentiments of their relatives as they were 20 years ago. Furthermore, and in spite of many families being geographically dispersed, family structure in African culture appears to play an important role. Decision making is the purview of the elders, and other family members may be unwilling to make decisions on donation without elder approval.[11] In practice, we have often observed that family members who are asked to consider organ donation are unaware of the wishes of their relatives.
SA has an opt-in system of organ donation. This means that organs of a deceased individual may not be donated without informed consent from the next of kin. This applies even when the individual is a registered organ donor.[1] In an attempt to mitigate low donor numbers, some countries have adopted presumed consent systems whereby all individuals are presumed willing organ donors unless they have complied with formal processes to express unwillingness to donate organs.[12] It may be argued that adopting a presumed consent system in SA could alleviate factors regarding disinclination to donate the organs of a relative, as familial consent would not necessarily be sought. We postulate, however, that a presumed consent system would not be workable in the SA context, as it is not consistent with fundamental SA freedoms, including religious and cultural freedom, as well as informed consent and its corollary, informed refusal. A presumed consent policy could jeopardise these rights, as it is currently unlikely to be possible to disseminate sufficient information to constitute an 'informed' refusal owing to communication limitations posed by language and literacy barriers as well as access to information. Furthermore, practice in countries with presumed consent suggests that relatives have the final say as to whether organs are to be donated. [12] More should be done to influence communication about organ donation among family members.
Looking at organs that participants are willing to donate, it is interesting to note that black African respondents reported a greater willingness to donate kidneys in the current study than in 1993. We cannot definitively attribute the cause of this shift to any specific factor or factors, which may include knowing someone who has received a kidney transplant[13] or be related to advertising campaigns regarding living kidney donation. However, kidney transplantation has also been portrayed negatively in the SA press.[14] A similar case in Germany led to a sharp decline in living organ donation.[15]
A decrease in willingness to donate heart, liver and corneas was expressed by the black African population. This is consistent with cultural beliefs that emphasise the role of the ancestors after death, and the notion that the body should remain intact for spiritual reasons.'111 However, there may be more subtle reasons for the shift. Hearts are sometimes imbued with mythologies that might influence perceptions. Furthermore, heart transplantation may be considered an option only for the more affluent, so it is not prominent among black Africans, many of whom are less wealthy than whites. For instance, in Gauteng Province the only heart transplant centre is in the private sector, requiring that individuals are members of a medical scheme, or pay for clinical management. [1] Negative sentiments about liver transplantation may be linked to perceptions of the liver and alcoholism, which is a source of contention in SA society.[16]
Recommendations
This research presents a comparison of attitudes towards organ donation in sections of the SA population. It is recommended that the study be repeated to include the Asian, Indian and mixed-race populations after a suitable time lapse in order to continually gauge attitudes - the 2012 data would serve as the baseline for groups not included in the 1993 study. It is also recommended that the study be repeated in a rural population.
Our previous research suggests that television advertising is one of the most effective ways of communicating information about organ donation to the SA public.[13] It is recommended that lobbying organisations consider family communication regarding preferences- for donation as a message that must be widely disseminated. This may assist in improving consent rates, as relatives will not feel they are making a decision on behalf of a loved one without knowing their preferences. Demographic factors such as language and literacy levels of the target population should be carefully considered for such campaigns to dispel some of the negative sentiment found in this research.
The authors are of the opinion that some of the content in SA organ donation campaigns is not clear. While a discussion of this is beyond the scope of this paper, the advertisement by the Australian Government[17] provides a good example of clear, concise promotional advertising in support of organ donation.
Acknowledgements
The authors gratefully acknowledge TNS for assistance with field work, as well as Astellas Transplant and Roche for unrestricted educational grants.
References
1. Organ Donor Foundation of South Africa. Statistics, How we create public awareness, Transplant centres in South Africa. 2013. http://www.odf.org.za (accessed 18 September 2013). [ Links ]
2. Kahn D, McCurdie F, Michaelides A. Socioeconomic factors, as well as race, impact on consent rates for organ donation. Proceedings of the 25th Southern African Transplantation Society Congress, 29 July - 2 August 2013. Durban: South African Transplant Society, 2013. [ Links ]
3. Pike RE, Odell JA, Kahn D. Public attitudes to organ donation in South Africa. S Afr Med J 1993;83(2):91-94. [ Links ]
4. Ozler B. Not separate. Not equal. Poverty and inequality in post-apartheid South Africa. Econ Dev Cult Change 2007;55(3):487-529. [ Links ]
5. Statistics South Africa. General Household Survey 2011. Pretoria: Statistics South Africa, 2011. http://www.statssa.gov.za/Publications/P0318/P0318April2012.pdf (accessed 24 January 2013). [ Links ]
6. Health Systems Trust. Forty Million South Africans without Medical Aid. Durban: Health Systems Trust, 2009. http://www.hst.org.za/publications/forty-million-south-africans-without-medical-aid (accessed 24 January 2013). [ Links ]
7. SAS Institute Inc. SAS Software, Version 9.3 for Windows. Cary, NC: SAS Institute Inc., 2002. [ Links ]
8. Statistics South Africa Census 2011. Pretoria: Statistics South Africa, 2012. http://www.statssa.gov.za/Publications/P03014/P030142011.pdf? (accessed 11 September 2013). [ Links ]
9. Schulze C. Press Release: Racial transformation not 'complete failure'. 12 September 2013. Johannesburg: South African Institute of Race Relations, 2013. http://www.sairr.org.za/media/media-releases/PRESS%20RELEASE%20-%20Racial%20transformation%20not%20complete%20failure.pdf/view (accessed 11 September 2013). [ Links ]
10. Little P, Everitt H, Williamson I, et al. Preferences of patients for patient centred approach to consultation in primary care: Observational study. BMJ 2001;322(7284):468. 'http://dx.doi. org/10.1136/bmj.322.7284.4681 [ Links ]
11. Kometsi KJ, Louw J. Deciding on cadaveric organ donation in black African families. Clin Transplant 1999;13(6):473-478. 'http://dx.doi.org/10.1034/j.1399-0012.1999.130606.xj [ Links ]
12. Abadie A, Gay S. The impact of presumed consent legislation on cadaveric organ donation: A crosscountry study. Health Econ 2006;25(4):599-620. 'http://dx.doi.org/10.1016/j.jhealeco.2006.01.003; [ Links ]
13. Etheredge HR, Turner RE, Kahn D. Public attitudes to organ donation amongst a sample of urban-dwelling South African adults: A 2012 study. Clin Transplant 2013;27(5):684-692. 'http://dx.doi.org/10.1111/ctr.122001 [ Links ]
14. Sidley P. South African doctors arrested in kidney sale scandal. BMJ 2005;331(473):1. 'http://dx.doi.org/10.1136/bmj.331.7515.4731 [ Links ]
15. Schmidt F. Organ donation in Germany hindered by transplant scandal (Online). Bonn: Deutsche Welle (German National News Channel), 2013. http://www.dw.de/organ-donation-in-germany-hindered-by-transplant-scandal/a-17027343 (accessed 16 September 2013). [ Links ]
16. Govender JP. The proposed banning of alcohol advertising in a developing economy. Economics and Behavioural Studies 2013;5(4):210-220. [ Links ]
17. Australian Government. 2012. Organ Donation Advert. http://www.youtube.com/watch?v=C8FYC8lMopA (accessed 28 January 2013). [ Links ]
 Correspondence:
Correspondence:
D Kahn
delawir.kahn@uct.ac.za
Accepted 17 October 2013.


{kind=link}
{kind=link}
{kind=link}
{kind=link}