










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSAMJ: South African Medical Journal
versão On-line ISSN 2078-5135
versão impressa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.104 no.2 Pretoria Fev. 2014
RESEARCH
Maintaining wellbeing for South Africans receiving ART: The burden of pain and symptoms is greater with longer ART exposure
L FarrantI; L GwytherII; N DinatIII; K MmolediIV; N HattaV; R HardingVI
IMB BCh, Dip HIV Man (SA), MPhil Pall Med; School of Public Health and Family Medicine, University of Cape Town, South Africa
IIMB ChB, FCFP, MSc; School of Public Health and Family Medicine, University of Cape Town, South Africa
IIIMD, FCOG, MPhil Pall Med; Wits Palliative Care, School of Internal Medicine, University of the Witwatersrand, Johannesburg, South Africa
IVRN, MPH, Dip Pall Med; Wits Palliative Care, School of Internal Medicine, University of the Witwatersrand, Johannesburg, South Africa
VRN; Wits Palliative Care, School of Internal Medicine, University of the Witwatersrand, Johannesburg, South Africa
VIPhD; School of Public Health and Family Medicine, University of Cape Town, South Africa. Department of Palliative Care, Cicely Saunders Institute, King's College London, UK
ABSTRACT
BACKGROUND: Physical and psychological symptom burden among people with HIV infection is associated with poor quality of life, poorer treatment adherence, viral rebound and risk behaviour. Symptomatology has not been investigated among outpatients in sub-Saharan Africa.
OBJECTIVE: To measure the seven-day period prevalence, burden and correlates of pain and other physical and psychological symptoms among HIV patients receiving antiretroviral therapy (ART).
METHODS: This was a cross-sectional self-report study. A total of 378 patients were interviewed using validated tools in three South African public sector clinics.
RESULTS: The most prevalent symptoms were feeling sad (64%), feeling irritable (61.6%), worry (60.8%), numbness and tingling in hands/ feet (59.8%), and sexual problems (51%). In multivariate analysis, later disease stage was associated with worse psychological symptom burden (ß=0.359; 95% confidence interval (CI) 0.202 - 0.516; p<0.001), global symptom burden (ß=0.365; 95% CI 0.204 - 0.526; p<0.001) and number of symptoms (3=0.308; 95% CI 0.150 - 0.465; p<0.001). Those receiving treatment for a greater number of years also reported higher burden for physical (3=0.083; 95% CI 0.037 - 0.129; p<0.001), psychological (3=0.068; 95% CI 0.019 - 0.117; p=0.007) and global symptoms (ß=0.065; 95% CI 0.016 - 0.115; p=0.010), and a greater number of symptoms (ß=0.081; 95% CI 0.032 - 0.130; p=0.001).
CONCLUSIONS: The data reveal a high symptom burden despite treatment. Detailed symptom assessment and control continues to be required in the era of treatment.
Evidence from high-income settings has shown that HIV patients experience a high physical and psychological symptom burden in the presence of antiretroviral therapy (ART).[1,2] This symptom burden has been associated with sexual risk-taking, [3] poor adherence, [4] treatment switching[5] and viral rebound.[6]
HIV patients perceive that their symptoms remain untreated. [7,8] This perception is supported by evidence that physicians detect threefold fewer HIV-related symptoms than their patients report.[9] Doctors tend to overlook the assessment of pain and other treatable symptoms, instead focusing on symptoms that are physically measurable such as fever and weight loss, and are more likely to ask about symptoms in HIV patients perceived to be severely ill.[10]
The World Health Organization (WHO) advocates pain and symptom control as an essential component of HIV clinical care.[11] A significant proportion of patients receiving ART experience drug toxicities such as peripheral neuropathy and gastrointestinal problems,[12] requiring drug discontinuation or treatment change within, and between, classes of ART.[13] Investigation into prevalence and correlates of HIV-related symptoms is required to inform clinical practice and thereby improve clinical outcomes and quality of life in the presence of ART. [14,15]
The vast majority of data on pain and symptom prevalence have been reported from the pre-ART era in patients in high-income countries with AIDS-defining illnesses. As there are fewer treatment options available in low- and middle-income countries, adherence must be optimised and movement between classes of drugs minimised.
Given the relationship between symptom burden, poor adherence, treatment switching and viral rebound, symptom data are urgently needed to inform patient assessment and management in Africa.
The prevalence and high burden/high frequency of symptoms for patients receiving ART and those not receiving ART have been reported previously.[16] We report the seven-day period prevalence, burden and correlates of pain, and other physical and psychological symptoms, among HIV patients receiving ART in three public sector HIV clinics in South Africa (SA).
Methods
Study design
The study design was cross-sectional self-report with additional clinical data extracted from patient records.
The study was approved by the Committee for Research in Human Subjects (Medical) at the University of the Witwatersrand and by the Human Research Ethics Committee of the University of Cape Town.
Setting
The research was conducted in the outpatient adult HIV treatment clinics within three academic hospitals in Johannesburg, SA, which adhere to the most recent SA national ART guidelines. At the time of data collection, the clinics had implemented the recent change in the national guidelines to initiate ART in patients with a CD4+ count <200 cells/µl, regardless of stage; those with a CD4+ count <350 cells/µl and pregnant or co-infected with tuberculosis (TB); those who are WHO stage 4 regardless of CD4+ count and all patients with drug-resistant TB.[17]
Recruitment
Inclusion criteria accounted for HIV outpatients aged 18 years or older receiving ART and able to give informed consent to participate in data collection in one of the three most common languages: English, isiZulu and Sesotho. Simple random sampling was used by inviting every fifth patient attending the clinic to participate, on days selected at random over an eight-month period in 2009 - 2010. Informed consent was obtained from participants.
Data collection
Data were collected using self-report (demographics, symptom prevalence and burden) and extraction of data from files (CD4+ count at treatment initiation, time since treatment initiation, most recent CD4+ count, most recent viral load, whether the patient had switched treatment, WHO disease stage). The seven-day period prevalence and associated burden of symptoms was measured using the Memorial Symptom Assessment Scale Short Form (MSAS-SF).[18] The MSAS-SF measures 28 physical and four psychological symptoms and provides three subscale indices of Physical Symptom Distress (MSAS-Phys), Psychological Symptom Distress (MSAS-Psych) and Global Distress Index (MSAS-GDI).[14] Each of these three subscales has a possible score range of 0 - 4. The MSAS-SF has been widely used in HIV populations.[1,2,19,20] Finally, the research nurse scored the patient on the Karnofsky Performance Scale, which is a measure of physical performance scored from 0 (dead) to 100 (normal) in bands of 10[21] and is a commonly used measure of performance in HIV populations.[22]
Owing to potential literacy limitations in the population sampled, a research nurse read aloud each self-reported question and recorded the response to reduce any potential bias through mixed self-completion and researcher-administered questionnaires. Information and consent forms and the questionnaire were translated from English into isiZulu and Sesotho by forward and back translation and the interview was conducted in the patient's language of choice.
Analysis
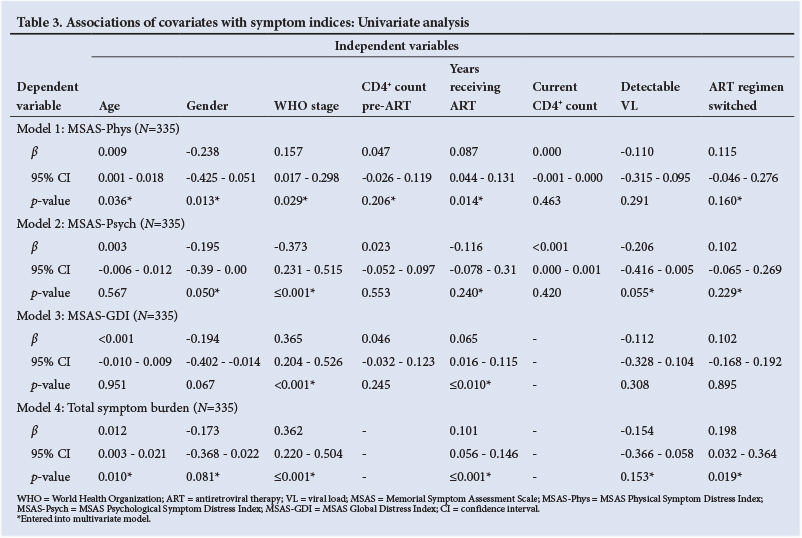
Descriptive data were generated for the sample characteristics. The most common symptoms have been previously reported.[16] The MSAS-SF subscales and total number of symptoms were calculated. Subsequently, the following analyses were conducted. Univariate linear regression analyses were conducted to test the association of independent covariates with the following four dependent variables: (i) MSAS-Phys; (ii) MSAS-Psych; (iii) MSAS-GDI; and (iv) total symptom burden. Each of these four dependent variables formed a separate model in the subsequent multivariate analyses described below. As the burden scores were not normally distributed (data plotting showing a left-skew), they were transformed into tertiles.
Independent variables entered in univariate analysis were: age (continuous); gender (two levels of male/female); WHO stage (three levels of stage 1, 2, 3 or 4); CD4+ count at ART initiation transformed into quartiles; whether the patient had switched ART regimen (two levels: yes/no); current viral load (two levels: detectable/not detectable); current CD4+ count (continuous); and time receiving ART (years).
Following each univariate regression, multivariate regressions models were constructed. Independent variables from the univariate analyses above were entered into the multivariate model if significant- at the 25% level.[23] For each independent variable, the unstandardised ß coefficient and the 95% confidence interval (CI) were calculated. For each multivariate model, the F-value for the model and the r2 were calculated. Cases with missing data were excluded from the multivariate models. All analyses were conducted using SPSS (version 19).
Results
Sample characteristics
A total of 378 patients participated (Table 1). The mean age of the patients was 40.3 years, the majority were female (76.2%) and of black ethnicity (98.1%). Participants had been receiving treatment for an average of three years and had a current average CD4+ count of 355.85 cells/µl (standard deviation (SD) ±219.26). According to the latest results available in the participants' records, around one-quarter of the sample (n=99; 28.6%) did not have viral suppression, and almost half (n=172; 45.5%) had switched ART regimen.

Symptomatology
The mean number of symptoms (of a possible total of 32) was 10.05 (SD ±5.66; range 1 - 28). The symptom prevalence and burden are presented in descending order of prevalence in Table 2. Three of the four psychological symptoms (sad, irritable and worrying) were among the ten most prevalent symptoms. The ten symptoms with the highest burden (i.e. scored using the worst two response categories) were: numbness and tingling in the hands/feet (37% of whole sample); feeling irritable (36.8%); problems with sexual interest or function (35.1%); worry (34.4%); not looking like myself (34.4%); feeling sad (30.7%); pain (29.1%); weight loss (24.8%); sweats (22.7%); and feeling nervous (20.6%).
Regression analyses: Associations with symptom burden indices
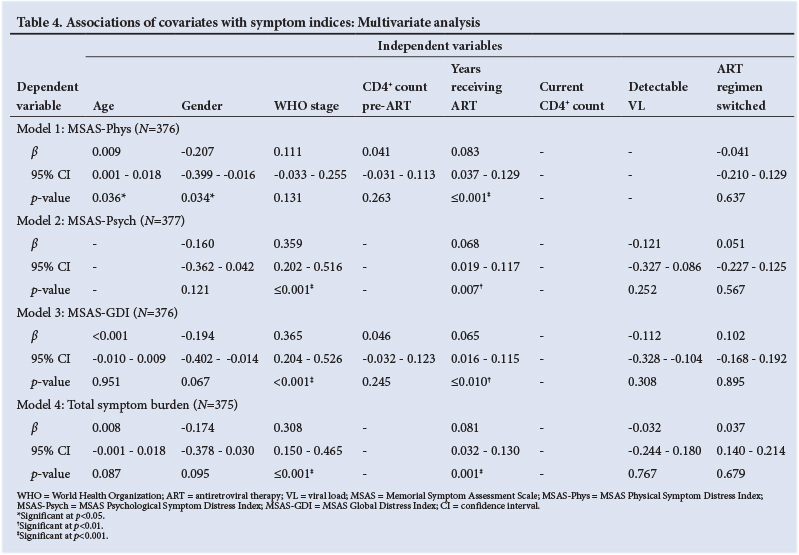
The univariate analysis is presented in Table 3. In multivariate analysis (Table 4), for the first model (MSAS-Phys; F=4.878; p<0.001; r2=8%) the following independent associations were identified. Higher physical symptom distress was associated with greater age (ß=0.009; 95% CI 0.001 - 0.018; p=0.036); female gender (ß=-0.207; 95% CI -0.399 - -0.016; p=0.034); and greater number of years receiving ART (ß=0.083; 95% CI 0.037 - 0.129; p<0.001). For the second model (MSAS-Psych; F=6.967; p<0.001; r2=9%), higher psychological distress was associated with later WHO stage-(ß=0.359; 95% CI 0.202 - 0.516; p<0.001) and greater number of years receiving treatment (ß=0.068; 95% CI 0.019 - 0.117; p=0.007). For the third model (MSAS-GDI; F=5.152; p<0.001; r2=10%), higher global symptom distress was associated with later WHO stage (ß=0.365; 95% CI 0.204 - 0.526; p<0.001) and greater number of years receiving ART (ß=0.065; 95% CI 0.016 - 0.115; p=0.010). For the fourth model (total symptom distress, model F=6.407; p<0.001; r2=10%), higher total symptom distress was associated with later WHO stage (ß=0.308; 96% CI 0.150 - 0.465; p<0.001) and greater number of years receiving ART (ß=0.081; 95% CI 0.032 -0.130; p=0.001).
Discussion
These data reveal a high prevalence and burden of symptoms among HIV patients receiving ART in SA, which persists despite relatively good physical function and the majority having been receiving treatment for several years. Seven symptoms were scored in the worst two categories of burden by around one-third of the sample, and these symptoms were psychological and physical, including a symptom indicative of peripheral neuropathy as well as other pain and sexual dysfunction.
There were a number of associations with symptom burden. Although greater age and female gender were associated with physical symptom distress, a consistent relationship was identified between worse symptom indices and greater number of years receiving ART. This may be related to the greater number of years of having HIV infection, and to the toxicity of treatment. In addition to clinician monitoring of patient wellbeing when beginning treatment, these data suggest that those who are treatment-experienced should have their symptom burden assessed alongside measurement of virological efficacy. Although there was a high symptom burden for the whole sample, the data also suggest that those with more advanced disease (as measured by WHO staging) may experience a greater burden.
A systematic review has demonstrated that palliative care can effectively control these burdensome problems in HIV populations.[24] It is essential that clinical medicine takes account of patient self-reported problems to improve quality of care.[25] Our data on pain and symptom prevalence, and associated distress, support the Joint United
Nations Programme on HIV/AIDS (UNAIDS) and WHO policy that palliative care is necessary throughout the HIV disease trajectory alongside ART.[11,26] In light of the data suggesting that uncontrolled symptoms adversely affect quality of life[8,27] and are associated with poor adherence,[4] sexual risk-taking,[3] treatment switching[5] and viral rebound,[6] we recommend that clinicians regularly assess their patients' physical and psychological self-reported symptoms.
Study limitations
There were a number of methodological limitations to our study. Firstly, the cross-sectional nature of the design meant that we could not draw causal relationships to symptom burden. Second, the reliance on file data, rather than collecting new primary data on clinical outcomes, may have introduced some inaccuracy.
Conclusion
Within Africa, symptom prevalence data have been reported in newly diagnosed HIV patients preparing for treatment,[19] and among patients with advanced disease.[1,20] Our study has built on the small body of prior evidence on prevalence and correlates of symptom burden in African patients[28-30] and supports prior findings that symptoms persist despite ART. Our data indicate that, alongside treatment to prolong life, clinical care should include detailed assessment and control of pain and symptoms to maximise quality of life and treatment benefit. In particular, our data suggest that although all patients should have their symptoms assessed regularly and controlled, those who have spent a longer time receiving ART, and those with more advanced disease, may require greater attention.
Acknowledgements
We thank the patients who participated, the management and staff of Wits Palliative Care, Nthabiseng Clinic at Chris-Hani Baragwanath Academic Hospital, Themba Lethu Right-to-Care Clinic at Helen Joseph Hospital, and the HIV Clinic at Charlotte Maxeke Johannesburg Academic Hospital.
References
1. Harding R, Lampe FC, Norwood S, et al. Symptoms are highly prevalent among HIV outpatients and associated with poor adherence and unprotected sexual intercourse. Sex Transm Infect 2010;86(7):520-524. [http://dx.doi.org/10.1136/sti.2009.038505] [ Links ]
2. Harding R, Molloy T, Easterbrook P, Frame K, Higginson IJ. Is antiretroviral therapy associated with symptom prevalence and burden? Int J STD AIDS 2006;17(6):400-405. [http://dx.doi.org/10.1258/095646206777323409] [ Links ]
3. Harding R, Clucas C, Lampe FC, et al. Behavioral surveillance study: Sexual risk taking behaviour in UK HIV outpatient attendees. AIDS Behav 2012;16(6):1708-1715. [http://dx.doi.org/10.1007/s10461-011-0023-y] [ Links ]
4. Sherr L, Lampe F, Norwood S, et al. Adherence to antiretroviral treatment in patients with HIV in the UK: A study of complexity. AIDS Care 2008;20(4):442-448. [http://dx.doi.org/10.1080/09540120701867032; [ Links ]
5. Sherr L, Lampe F, Norwood S, et al. Successive switching of antiretroviral therapy is associated with high psychological and physical burden. Int J STD AIDS 2007;18(10):700-704. [http://dx.doi.org/10.1258/095646207782193821] [ Links ]
6. Lampe FC, Harding R, Smith CJ, Phillips AN, Johnson M, Sherr L. Physical and psychological symptoms and risk of virologic rebound among patients with virologic suppression on antiretroviral therapy. J Acquir Immune Defic Syndr 2010;54(5):500-505. [http://dx.doi.org/10.1097/QAI.0b013e3181ce6afe] [ Links ]
7. Karus D, Raveis VH, Alexander C, et al. Patient reports of symptoms and their treatment at three palliative care projects servicing individuals with HIV/AIDS. J Pain Symptom Manage 2005;30(5):408-417. [http://dxdoi.org/10.1016/j.jpainsymman.2005.04.011] [ Links ]
8. Harding R, Molloy T. Positive futures? The impact of HIV infection on achieving health, wealth and future planning. AIDS Care 2008;20(5):565-570. [http://dx.doi.org/10.1080/09540120701867222] [ Links ]
9. Justice AC, Chang CH, Rabeneck L, Zackin R. Clinical importance of provider-reported HIV symptoms compared with patient-report. Med Care 2001;39(4):397-408. [http://dx.doi.org/10.1097/00005650-200104000-00010] [ Links ]
10. Larue F, Fontaine A, Colleau SM. Underestimation and undertreatment of pain in HIV disease: Multicentre study. BMJ 1997;314(7073):23-28. [http://dx.doi.org/10.1136/bmj.314.7073.23] [ Links ]
11. World Health Organization. HIV/AIDS Topics: Palliative Care 2006. Geneva: WHO, 2006. http://www.who.int/hiv/topics/palliative/PalliativeCare/en/ (accessed 19 December 2013). [ Links ]
12. Heath KV, Montaner JS, Bondy G, Singer J, O'Shaughnessy MV, Hogg RS. Emerging drug toxicities of highly active antiretroviral therapy for human immunodeficiency virus (HIV) infection. Curr Drug Targets 2003;4(1):13-22. [ Links ]
13. Dieleman JP, Jambroes M, Gyssens IC, et al. Determinants of recurrent toxicity-driven switches of highly active antiretroviral therapy. The ATHENA Cohort. AIDS 2002;16(5):737-745. [http://dx.doi.org/10.1097/00002030-200203290-00009] [ Links ]
14. Selwyn P. Why should we care about palliative care for AIDS in the era of antiretroviral therapy? Sex Transm Infect 2005;81:2-3. [http://dx.doi.org/10.1136/sti.2004.011585] [ Links ]
15. The untapped potential of palliative care for AIDS. Lancet 2003;362(9398):1773. [ Links ]
16. Farrant L, Gwyther L, Dinat N, Mmoledi K, Hatta N, Harding R The prevalence and burden of pain and other symptoms among South Africans attending highly active antiretroviral therapy (HAART) clinics. S Afr Med J 2012;102(6):499-500. [ Links ]
17. National Department of Health, South African National AIDS Council. The South African Antiretroviral Treatment Guidelines 2010. Pretoria: NDoH, 2010. http://www.uj.ac.za/EN/CorporateServices/ioha/ Documentation/Documents/ART%20Guideline.pdf (accessed 11 December 2013). [ Links ]
18. Chang VT, Hwang SS, Feuerman M, Kasimis BS, Thaler HT. The Memorial Symptom Assessment Scale Short Form (MSAS-SF). Cancer 2000;89(5):1162-1171. [http://dx.doi.org/10.1002/1097-0142(20000901)89:5<1162::AID-CNCR26>3.0.CO;2-Y] [ Links ]
19. Wakeham K, Harding R, Bamukama-Namakoola D, et al. Symptom burden in HIV-infected adults at time of HIV diagnosis in rural Uganda. J Palliat Med 2010;13(4):375-380. [http://dx.doi.org/10.1089/ jpm.2009.0259] [ Links ]
20. Harding R, Selman L, Agupio G, et al. Prevalence, burden, and correlates of physical and psychological symptoms among HIV palliative care patients in sub-Saharan Africa: An international multicenter study J Pain Symptom Manage 2012 Jul;44(1):1-9. [http://dxdoi.org/10.1016/j.jpainsymman.2011.08.008] [ Links ]
21. Schag CC, Heinrich RL, Ganz PA. Karnofsky performance status revisited: Reliability, validity, and guidelines. J Clin Oncol 1984;2(3):187-193. [ Links ]
22. Morgan EE, Iudicello JE, Weber E, et al. Synergistic effects ofHIV infection and older age on daily functioning. J Acquir Immune Defic Syndr 2012 61(3):341-348. [http://dx.doi.org/10.1097/QAI.0b013e31826bfc53] [ Links ]
23. Altman DG. Practical Statistics for Medical Research. London: Chapman and Hall, 1991. [ Links ]
24. Harding R, Karus D, Easterbrook P, Raveis VH, Higginson IJ, Marconi K. Does palliative care improve outcomes for patients with HIV/AIDS? A systematic review of the evidence. Sex Transm Infect 2005;81(1):5-14. [http://dx.doi.org/10.1136/sti.2004.010132] [ Links ]
25. Dawson J, Doll H, Fitzpatrick R, Jenkinson C, Carr AJ. The routine use of patient reported outcome measures in healthcare settings. BMJ 2010;340:c186. [http://dx.doi.org/10.1136/bmj.c186] [ Links ]
26. Joint United Nations Programme on HIV/AIDS. AIDS: Palliative Care: UNAIDS Technical Update. Geneva: UNAIDS, 2000. http://apps.who.int/medicinedocs/en/d/Jh2930e/ (accessed 11 December 2013). [ Links ]
27. Harding R, Clucas C, Lampe FC, et al. What factors are associated with patient self-reported health status among HIV outpatients? A multi-centre UK study of biomedical and psychosocial factors. AIDS Care 201234(8):963-971. [http://dx.doi.org/10.1080/09540121.2012.668175] [ Links ]
28. Mphahlele NR, Mitchell D, Kamerman PR. Pain in ambulatory HIV-positive South Africans. Eur J Pain 2012;16(3):447-458. [http://dx.doi.org/10.1002/j.1532-2149.2011.00031.x] [ Links ]
29. Peltzer K, Phaswana-Mafuya N. The symptom experience of people living with HIV and AIDS in the Eastern Cape, South Africa. BMC Health Serv Res 2008;8:271. [http://dx.doi.org/10.1186/1472-6963-8-271] [ Links ]
30. Namisango E, Harding R, Atuhaire L, et al. Pain among ambulatory HIV/AIDS patients: Multicenter study of prevalence, intensity, associated factors, and effect. J Pain 2012;13(7):704-713. [http://dx.doi. org/10.1016/j.jpain.2012.04.007] [ Links ]
 Correspondence:
Correspondence:
L Farrant
lindsayfarrant0074@yahoo.co.uk
Accepted 9 September 2013.


{kind=link}
{kind=link}
{kind=link}