










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.104 n.2 Pretoria Feb. 2014
IZINDABA
Activists warn: Don't fall victim to our HIV successes
Chris Bateman
Debating whether the end of AIDS is 'a reality or myth' (given the 33% global reduction in deaths over the past decade, and the hugely successful up-scaling of treatment and prevention in South Africa) is 'misleading and dangerous', warn local civil society activists and researchers.
Speaking at the launch of their review of the government's National Strategic Plan (NSP) for HIV, sexually transmitted infections (STIs) and tuberculosis (TB) (2012 - 2016), were the Treatment Action Campaign (TAC) and Section 27, plus groundbreaking leaders in antiretroviral therapy (ART) Médecins Sans Frontières (MSF) and leading HIV clinician Prof. Francois Venter. They were partially backed by Prof. Alan Whiteside, the outgoing head of the self-funded Health Economics and HIV/AIDS Research Division (HEARD) at the University of KwaZulu-Natal.
These bodies' views provide a cold and often unwelcome counterpoint to the national department of health (NDoH's) proud broadcasting of South Africa (SA's) dramatic AIDS turnaround, and the premature global political trend of claiming imminent victory over the pandemic. The debate came during the International Conference on AIDS and STIs in Africa (ICASA) held in Cape Town in early December.
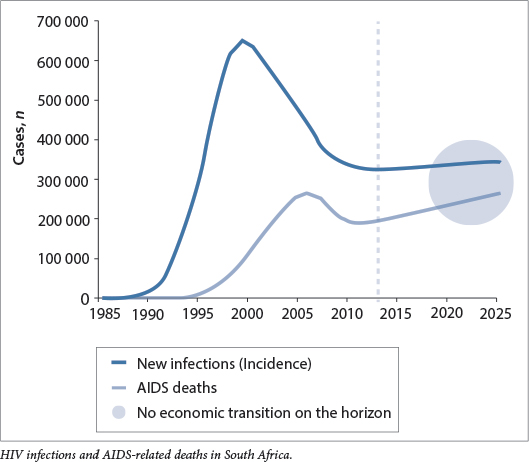
Whiteside defined an end to AIDS as zero new infections or adult transmission, 100% prevention of mother-to-child HIV infection and total medical and blood safety, concluding that this is unlikely. 'What's most likely is that it will become a low-level endemic disease, unless we come up with a vaccine or a cure. No-one living with AIDS? Certainly not in my lifetime. Everyone on treatment? Possible, but unlikely.'
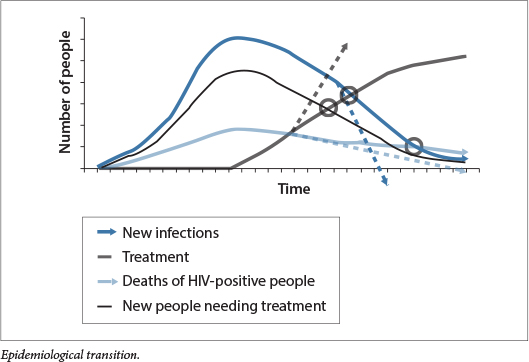
Touting what he called the 'economic transition theory', Whiteside said health is simply not on the global priority list, with neither enough resources nor political will available. SA, like several countries carrying similar, if lesser HIV burdens, is 'locked in an economic trap' with no economic transition apparent. International funding streams are uncertain, forcing countries like ours to plumb insufficient domestic resources. Ministries of health and finance live in a waking nightmare in which need for- treatment is always increasing while the rate of HIV infections stubbornly refuses to come down. Displaying graphs depicting 'advocacy and epidemiological transition points', Whiteside highlighted the intersection of the curve showing the numbers of people on treatment with that showing the number of- those needing treatment, commenting, 'We need to celebrate our real successes.' The second transition (or 'tipping') point will be where the number of people on treatment exceeds the number of new infections.

What is 'really interesting' is seeing how the more people are put on treatment, the lower the rates of death and new infection (especially with treatment as prevention) become. 'The intersecting lines move. Things happen faster and sooner than before, saving lives, money and time. That's when we start moving to the end of AIDS.' Whiteside said SA has lost four crucial years in which preventative measures weren't taken and now simply 'has to turn off the tap' of AIDS infection, while treatment remains crucial 'for medical, moral, ethical and economic reasons'.
'We're in control, but far from winning' Heywood
Mark Heywood of the TAC said that, for the first time, 'we can see that we're controlling the epidemic and it's not controlling us'. However, talking about the end of AIDS is 'misleading, potentially demobilising and irresponsible'. He appealed to UNAIDS to 'put this talk back in the can as quickly as possible'. He said that while a great deal had changed since the 1980s, the most recent (2012) United Nations report showed 2.3 million new infections and 1.6 million deaths worldwide, with 10 million Africans still waiting for treatment. Globally, HIV coverage of children remains half that of adults. While HIV is a virus, AIDS 'has always been about the conditions that facilitate the transmission of the virus', said Heywood. He identified obstacles such as sex work remaining criminalised, inequality and violence continuing unchecked, and stigma and discrimination, which he said are 'slightly lower, but still hinder us'.
He also warned that governments, riding the wave of AIDS successes, are pushing back civil society's hold on the reins of accountability at global and national level. Many structures, such as AIDS councils in many countries, have become 'ossified, corrupt and conservative' - a real problem because they are most often the gatekeepers of global funds. UNAIDS has fundamentally shifted the focus of its response paradigm from human rights to investment returns, overemphasising the biomedical approach while only paying lip service to a societal response.
Currently, non-govermental organisations (NGOs) are fighting for survival, thus lessening government accountability, while deeply socially entrenched and enduring problems facilitate the spread of AIDS. There is no guarantee of a steady exponential response to AIDS, Heywood stressed. 'We didn't campaign for a sufficient number of people to be on treatment, but for all people's right to be on treatment. At best we are nowhere near the end of AIDS. There are- dark clouds ahead. We have to determine the social and political determinants of AIDS and weaknesses in our health systems like drug stock-outs. Civil society is being corporatised and co-opted. I guess I have to apologise for being a spanner in the end-of-AIDS works!' he joked.

Learn how many are in care
SA's National Health Minister Dr Aaron Motsoaledi acknowledges 'logistical problems when it comes to drug distribution', but notes that sometimes stock-outs are caused by the drug industry. Another issue is the thorny and largely unquantified question of retention in care, which HIV activists allege that government is deliberately avoiding to put the best spin on its success so far. Motsoaledi responds: 'Look at our life expectancy figures that are increasing. I think they answer that question.'
With 2.4 million people on ART (up from 923 000 in 2009), 3 540 HIV treatment sites established (up from 490 in 2009), and 23 000 nurses able to initiate patients on treatment compared with 250 four years ago, activists and researchers agree that the health department should take a bow. However Heywood and Venter, in their NSP review, say the lack of monitoring and evaluation could prove the Achilles' heel of these major gains. They stress that the South
African National AIDS Council (SANAC) still has no evaluation framework in place, so there's no way of knowing how many people are dropping out of treatment, for whatever reason.
South Africa's national figures reflect the total number of people who have ever been initiated on treatment, but vitally fail to reveal the numbers of those currently in care. Says Heywood, 'We cannot continue not knowing that for very much longer. Without this knowledge, what we're accepting as truths could lead us into an entirely different space.'
Stock-outs burst treatment success bubble
Heywood said that while the TAC has received extensive praise for its role in battling denialism and forcing ART breakthroughs, recent experience has convinced him that government and SANAC believe that fight is now in the past, 'and it's all milk and honey - independent criticism should be muted. In fact, some provinces are showing a fierce intolerance of independence.'
He cited a raid on the SANAC office in Bloemfontein last year by Free State officials variously identifying themselves as either the Hawks or 'security from the Health MEC's office', in which several computers were 'confiscated'. Many members of the civil-society Stop Stock Outs coalition, who also serve on SANAC, operate from SANAC offices and had a pivotal role in exposing the fact that 54% of Free State facilities experienced drug stock-outs over the past three months.
The Free State's TAC leader also received anonymous death threats over the phone and was reassigned out of the province as a security precaution, Heywood revealed. He said the raid had been reported to Deputy President Kgalema Motlanthe via SANAC.
In September and October last year the TAC and Section 27, under the umbrella of the Stop Stock Outs coalition, released the results of a nationwide telephonic survey showing that one in five facilities (459 of 2 139 or 21%) reported a stock-out or shortage in the preceding three months. Half of these were still facing shortages at the time of the survey. Six out of the nine provinces had more than 17% of their facilities reporting shortages. Almost half of antiretroviral (ARV) stock-outs were of lamivudine, efavirenz or stavudine while the median duration of shortages was 30 days, ranging from one day to one year. In 20% of all facilities patients were sent home or referred elsewhere - without medicines.
The report - worse than many feared -rocked the public health sector because of its grave implications for the health system and patients, including drug resistance, decreased immunity, increased risk of opportunistic infections and higher overall transmission rates.
NHLS the key - Venter and Rees
Prof. Venter, Deputy Executive Director at the University of the Witwatersrand's Reproductive Health and HIV Institute, estimates that at every stage of HIV care (from the initial test, to receiving follow up CD4+ cell count results, to being placed on treatment) a staggering 50% of patients are lost. He cites studies showing that patients are more likely to fall out of the system between the time they are tested for HIV and the time they become eligible for treatment. Venter and his colleague Prof. Helen Rees make an impassioned plea in the NSP review for better use of data from the National Health Laboratory Service (NHLS) to understand how many people are falling off treatment, how many are virally suppressed and what their CD4+ cell counts are.
Venter lashed out at provinces for playing 'brinkmanship' with the NHLS by not paying their bills, and said the level of defensiveness when provinces are confronted with disturbing facts makes it difficult to hold them accountable. 'National [government] will admit to problems, but the minute you go down to the provinces, there's a problem,' he said. He said the NHLS is an invaluable ally in improving the performance of the NSP, and called it 'inexcusable' that it has been undermined by the provinces to the point where its services are in danger of being shut down.
Department responds
Dr Yogan Pillay, Deputy Director General of HIV/AIDS, TB and Maternal, Child and Women's Health at the NDoH scotched many of the activists' claims. He told Izindaba that his department's Tier.net system for monitoring the ARV rollout had 'back-captured' data from 1 600 facilities to 2004, including loss-to-follow-up, viral loads, CD4+ counts and viral suppression. His plan is to roll Tier.net out to all 3 000 public sector ART-providing facilities, 'in a virtual analogue of the TB register'.
South Africa's national figures reflect the total number of people who have ever been initiated on treatment, but vitally fail to reveal the numbers of those currently in care.
Using World Health Organization (WHO) registration guidelines, the department has migrated data from more than 1 600 facilities from Tier One (paper based) to Tier Two (electronic and easier to analyse). The next step (Tier Three) will provide an electronic medical record for each individual patient to allow clinicians to access their treatment history, wherever they present. 'We're now moving those facilities with a large number of patients to Tier Three, and within three years hope to embrace all our ART facilities,' said Pillay. He said that Tier Two is currently being 'bedded down' at facility level. Both the President's Emergency Plan For AIDS Relief (Pepfar) and the Global Fund are helping bankroll the hiring and training of data capturers. A full publication of 'how we are doing' is due shortly.
Regarding activists' claims about drug stock-outs, Pillay said the NDoH has been working with a wide cross-section of civil society organisations 'for a significant amount of time trying to solve the problems. To write a report as if this is not the case is a little bit disingenuous.'
He added, 'I'm not suggesting for a moment that there are no stock-outs, but the reports analysis and methodology overestimates the extent.' Pillay said monitoring systems are in place (via district pharmacists, provinces, the AIDS hotline and civil society, including the HIV Clinicians Society). There are a number of reasons for stock outs, not the least of which is the long supply chain. 'Nobody wants patients moving onto second- and third-line drugs, least of all us,' he added.
Asked to give examples of where the drug shortage survey was exaggerated, Pillay said 'just a few' include reporting stock-outs of 600 mg pills, when the same facility had identical 200 mg preparations (i.e. three pills dispensed instead of one), and alleging a shortage of stavudine when his staff are busy switching patients onto a replacement drug because of side-effects. 'To call these stock-outs is just confusing. My big concern, which I've conveyed to Mark (Heywood), is that if you make too big a deal out of stock-outs, patients will read this and simply stop bothering to come - and we'll end up with an unintended consequence, feeding into non-adherence.' Pillay added, 'We must work together to ensure there are no stock-outs.'
The battle is obviously far from over: provincial complacency, denialism and mistrust still drive death and sickness -though thankfully no longer on a holocaustlike scale. Meanwhile, however, engagement between previously implacable enemies comes as a welcome relief.

