










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSAMJ: South African Medical Journal
versão On-line ISSN 2078-5135
versão impressa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.104 no.1 Pretoria Jan. 2014
RESEARCH
Sexual lubricants in South Africa may potentially disrupt mucosal surfaces and increase HIV transmission risk among men who have sex with men
K B RebeI; G de SwardtII; P A Berman,III; H Struthers,IV; J A McIntyre,V, VI
IMB ChB, FCP (SA) DTM&H Anova Health Institute, Johannesburg and Cape Town, South Africa
IIBA (MW) Anova Health Institute, Johannesburg and Cape Town, South Africa
IIIBSc, MB ChB, MMed (Chem Path) Division of Chemical Pathology, Faculty of Health Sciences, University of Cape Town, South Africa
IVMSc, MBA Anova Health Institute, Johannesburg and Cape Town, South Africa
VMB ChB, FRCOG Anova Health Institute, Johannesburg and Cape Town, South Africa
VIMB ChB, FRCOG School of Public Health and Family Medicine, University of Cape Town, South Africa
ABSTRACT
BACKGROUND: Men who have sex with men (MSM) are at high risk for HIV acquisition and transmission. There is a high HIV-transmission potential associated with unprotected anal intercourse (UAI), which requires sexual lubrication for comfortable, non-traumatic anal sex. Lubricant distribution remains poor in many developing nations and MSM have been known to substitute a number of common household or food products to ensure comfortable anal sex. Concern has been raised about the potential toxicity of lubricants used during anal sex. Epithelial injury is related to the osmolality of the lubricant product.
OBJECTIVE: To analyse commercially available water-based sexual lubricant products to ascertain their osmolality and potential to cause rectal epithelial damage.
METHODS: The osmolality and glycerol concentration was determined for eight of the most frequently purchased water-based sexual lubricants and some commonly used household/food products.
RESULTS: Osmolality ranged from 270 - 9 440 mosmol/l (Lubrimaxxx Premium, containing phytosqualane, and JO H2O Water Based Lubricant, respectively). Seven (88%) of the commercial lubricants had high osmolalities, with two products approaching 10 000 mosmol/l, far in excess of serum which has an osmolality of ~280 mosmol/l.
CONCLUSION: The results of this study show that many of the top-selling brands of water-based sexual lubricants available in SA are hyperosmolar. Given that hyperosmolar products have been shown in vitro and in vivo to cause epithelial injury, they may have the potential to increase HIV acquisition and transmission, if they are used during UAI. Awareness needs to be raised about the mucosal safety of lubricants designed for use during anal sex.
Men who have sex with men (MSM) are at high risk for HIV acquisition and transmission and their HIV prevalence is higher than heterosexual men in their specific country settings.[1] The reasons for this are multifactorial but a major risk contributor is the high HIV-transmission potential associated with unprotected anal intercourse (UAI). Receptive UAI is approximately 16 times more likely to result in HIV transmission than unprotected vaginal intercourse due to the fact that the anal mucosa is thinner than vaginal mucosa and does not self-lubricate before or during intercourse.[2] The HIV transmission risk associated with UAI applies equally to women engaging in this sexual behaviour. Sexual lubrication is therefore required for comfortable, non-traumatic anal sex. Lubricant use has also been associated with lower rates of condom failure during anal sex among MSM.[3] The use of lubricants for anal sex by MSM ranges from 0% in some developing world MSM cohorts to >90% reported among MSM communities in the USA.[4,5]
Distribution of condoms and water-based sexual lubricants forms a cornerstone of MSM-targeted HIV prevention programmes globally. Since HIV prevention interventions have failed among MSM in many settings, there is a need to scale up existing evidence-based interventions and to explore new prevention technologies that may be effective in this high-risk group of men.[4,5] Lubricant distribution remains poor in many developing nations and MSM have been known to substitute a number of products to ensure comfortable anal sex. These include saliva, food products such as egg white, yoghurt, jelly and cooking oils and a variety of condom-incompatible products such as hand lotions, moisturisers and petroleum jelly. Since these products are not normally considered as sexual lubricants, they have not been assessed for safety in the rectum. An alternative product containing phytosqualane (derived from olives) as the active ingredient and called Lubrimaxxx Premium has recently been developed by Karl de L'Eau Natural Skincare, Cape Town, as a sexual lubricant.
The role of lubricants in preventing HIV gained new prominence after studies demonstrated that topical tenofovir-containing products (microbicides) could reduce HIV transmission.[6,7] Microbicides could be formulated as sexual lubricants and are considered acceptable as a potential HIV risk-reduction intervention by MSM if they can be used safely for anal sex.[8,9]
Concern has been raised about the potential toxicity of lubricants used during anal sex.[10] Epithelial injury is related to the osmolality of the lubricant product.[11] The main concern is that hyperosmolar water-based lubricants may denude rectal epithelium and increase secretion of fluid into the bowel (signalling epithelial injury). By compromising the integrity of anal mucosa, lubricant use without condoms may increase the risk of HIV transmission.[12] Complementary work investigating hypo- v. iso-osmolar enemas has shown that hyperosmolar products cause epithelial damage and that iso-osmolar products are superior.[13] Additionally, there is concern that the constituents of some commercially available sexual lubricants may increase local HIV replication.[14] These issues are not well publicised among key populations who use sexual lubricants for comfortable and pleasurable anal sex as well as to reduce their risk of HIV infection. Information on the potential toxicity of lubricant substitutes used by African MSM is unavailable, making education of affected key populations difficult.
Objective
We analysed commercially available water-based sexual lubricant products to ascertain their osmolality and potential to cause rectal epithelial damage. A phytosqualane-containing formulation, and low-fat yoghurt and egg white (common lubricant substitutes), were also assessed.
Methods
Eight of the most frequently purchased water-based sexual lubricants were sourced from a leading local adult shop, one of a chain of sex shops in South Africa (SA) and from a local non-profit organisation distributing lubricant to MSM. KY Jelly and common lubricant substitutes (egg white and low-fat yogurt) were also included in the analysis, as was the phytosqualane-containing product, Lubrimaxxx Premium. Lubricants were diluted 1/10 and 1/50 in deionised water for osmolality and glycerol measurement, respectively, using positive displacement pipettes. Samples with extremely high glycerol concentrations were diluted 1/500 to obtain readings within the linear range of the assay employed. Egg albumin and yoghurt were diluted 1/2 for measurement of osmolality. Osmolality was measured by the Division of Chemical Pathology at the University of Cape Town, SA, using a freezing point depression osmometer. Glycerol was measured using the enzymatic triglyceride channel on the Roche Modular analyser (Roche Diagnostics, Switzerland).
Results
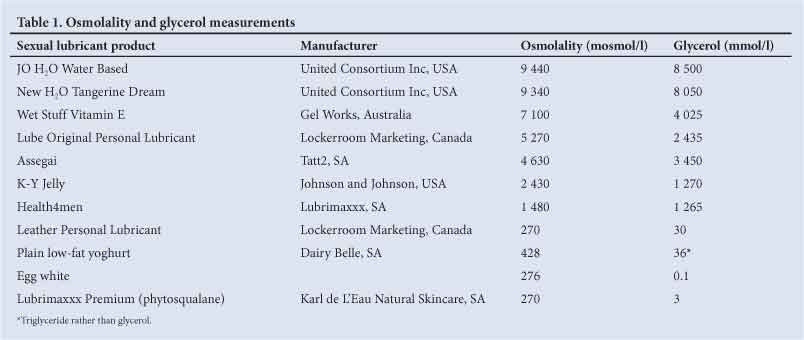
Osmolality and glycerol measurements are shown in Table 1. Osmolality ranged from 270 - 9440 mosmol/l (Lubrimaxxx Premium, containing phytosqualane and JO H2O Water Based Lubricant, respectively). Seven (88%) of the commercial lubricants had high osmolalities, with two products approaching 10 000 mosmol/l, far in excess of serum which has an osmolality of ~280 mosmol/l. Exceptions included Leather Personal Lubricant and Lubrimaxxx Premium. Egg white and low-fat yoghurt had osmolalities of 276 and 428 mosm/l, respectively. High osmolality could be attributed to glycerol and there was a strong direct correlation between osmolality and glycerol content on Wilcoxon matched pair analysis. (p=0.0033).
Discussion
The results of this study show that many of the top-selling brands of water-based sexual lubricants available in SA are hyperosmolar. Given that hyperosmolar products have been shown in vitro and in vivo to cause epithelial injury, they may have the potential to increase HIV acquisition and transmission, if they are used during UAI. This is particularly concerning since many at-risk MSM utilise these products in the belief that they provide protection from HIV infection by decreasing friction and resultant trauma to the rectal mucosa.
Lubricant substitutes vary in their safety. Phytosqualane-containing lubricants, egg white and plain (unflavoured) low-fat yoghurt are relatively isotonic and are therefore unlikely to cause the same epithelial injury seen following the use of very hyperosmolar lubricants. They could therefore be promoted in countries where proprietary lubricants are not freely available, as is the case in most African countries. Saliva is also commonly used as a lubricant substitute. This is potentially problematic since researchers have suggested that this might result in transmission of saliva-borne pathogens including herpes and hepatitis viruses.[8,15]
There is currently very little awareness among MSM in SA regarding lubricant safety. Manufacturers of sexual lubrication products are not required to offer product safety information, which results in the inability of users to assess their suitability. It has been demonstrated that currently available sexual lubricants do not have anti-HIV effects and some may even increase HIV replication.[14] Condom use among high-risk men remains inconsistent and therefore lubricant use in the absence of condoms is probably commonplace, a practice that may increase HIV transmission risk.[16]
Knowledge about HIV prevention technologies is generally low among MSM in SA. The work of organisations (such as the Anova Health Institute) that provide free MSM-targeted condoms and lubricants, and knowledge about utilisation of sexual lubricants, is increasing. Lubricant users must understand the risks and benefits of these products. Organisations such as the US Centers for Disease Control and the World Health Organization advocate the promotion of condom and lubricant use among MSM.[17,18]
Sexual lubricant safety is likely to gain importance as the search for a marketable microbicide product continues. Microbicides will need to be safe for vaginal and rectal use and their osmolality and potential mucosal toxicity are being evaluated. Organisations such as the International Rectal Microbicide Advocates (IRMA) are promoting this agenda.[19]
Recommendations
Awareness needs to be raised about the mucosal safety of lubricants designed for use during anal sex. This should include community-based work to educate MSM communities who are currently being encouraged to increase lubricant use. Information, education and communication (IEC) materials need to be developed and distributed that explain the medical concerns that arise when water-based sexual lubricants are used without condoms. Clearly, MSM-targeted HIV-risk-reduction messages must stress that lubricants should be used together with condoms. For MSM who use lubricants alone, advice should be given about the safer use of these products such as using silicone-based lubricants and avoiding high osmolality water-based products. Some lubricant substitutes such as egg white or yoghurt could be promoted, although this will have limited impact in countries where food insecurity is common and food products are more likely to be consumed than used for sexual safety. Phytosqualane-containing, water-based lubricants may offer a safe alternative to those that contain glycerine, provided they are not too costly. Healthcare workers providing sexual health services, inclusive of HIV counsellors, nurses and doctors, need to be sensitised to this issue to enable them to provide correct risk-reduction counselling to their patients. This information for providers and users of lubricants will need to be carefully managed to avoid a backlash against use of lubricant and microbicides in development.
Lastly, any future microbicide product that is promoted as an HIV-prevention intervention must be fully analysed to ensure safety by assessing any mucosal changes it may induce.
Study limitations
Only lubricant brands available from one major branch of adult shops and selling well in Cape Town during 2012, or available from Health4men, were included in this analysis. Popular lubricants used by MSM in other geographical settings have not been included. No analysis of the ingredients of the various assayed lubricants was performed and it is possible that some ingredients may interfere with osmolality analyses, although this is not likely. The ingredients and preservatives of the various lubricants have not been individually assessed for their mucosal toxicity. It is conceivable that a low osmolality lubricant may contain toxic additives, making it potentially more damaging to anal mucosa than suggested by its osmolality alone.
Acknowledgements. KBR and GdS conceived the idea. KBR undertook the literature search, GdS, JAM and HS contributed additional ideas and contributed to the manuscript. PAB designed and implemented the laboratory component of this work and contributed ideas to the manuscript. KBR, GdS, HS and JAM are supported in part by the US PEPFAR through USAID under the terms of Award No. 674-A-00-08-00009-00. The opinions expressed herein are those of the authors and do not necessarily reflect the views of USAID.
References
1. Baral SD. Elevated risk for HIV infection among men who have sex with men in low- and middle-income countries 2000-2006: A Systematic Review. PLoS Med 2007;4(12):1901-1911. [http://dx.doi.org/10.1371/journal.pmed.0040339] [ Links ]
2. Baggaley RF, White RG, Boily MC. HIV transmission risk through anal intercourse, systematic review, meta-analysis and implications for HIV prevention. Int J Epidemiol 2010;39(4):1048-1063. [http://dx.doi.org/10.1093/ije/dyq057] [ Links ]
3. Stone E, Heagerty P, Vittinghof E, et al. Correlates of condom failure in a sexually active cohort of men who have sex with men. J Acquir Immune Defic Syndr Hum Retroviral 1999;20(5):495-501. [http://dx.doi.org/10.1097/00042560-199904150-00013] [ Links ]
4. Rebe KB, Struthers H, de Swardt G, McIntyre JA. HIV prevention and treatment for South African men who have sex with men. S Afr Med J 2011;101(10):708-710. [ Links ]
5. Rebe KB, Semugoma P, McIntyre JA. New HIV prevention technologies and their relevance to MARPS in African epidemics. SAHARA J 2012;9(3):164-166. [http://dx.doi.org/10.1080/17290376.2012.744168] [ Links ]
6. Karim QA, Karim SSA, Frohlich JA, et al. Effectiveness and safety of tenofovir gel, an antiretroviral microbicide, for the prevention of HIV infection in women. Science 2010;329(5996):1168-1174. [http://dx.doi.org/10.1126/science.1193748] [ Links ]
7. Chateau ML, Denton PW, Swanson MD, McGowan I, Garcia JV Rectal transmission of transmitted/founder HIV-1 is efficiently prevented by topical 1% tenofovir in BLT humanized mice. PloS One 2013;8(3):e60024. [http://dx.doi.org/10.1371/journal.pone.0060024] [ Links ]
8. McGowan I. Rectal microbicides: Can we make them and will people use them? Aids Behav 2011;15(Suppl 1):S66-S71. [http://dx.doi.org/10.1007/s10461-011-9899-9] [ Links ]
9. McGowan I. Rectal microbicide development. Curr Opin HIV AIDS 2012;7(6):526-533. [http://dx.doiorg/10.1097/COH.0b013e3283582bc2] [ Links ]
10. Giebel S. Condoms and condiments: Compatibility and safety ofpersonal lubricants and their use in Africa. J Int AIDS Soc 2013;16:18531. [http://dx.doi.org/10.7448/IAS.16.L18531] [ Links ]
11. Adriaens E, Remon JP. Mucosal irritation potential of personal lubricants relates to product osmolality as detected by the slug mucosal irritation assay. Sex Transm Dis 2008;35(5):512-516. [http://dx.doiorg/10.1097/OLQ.0b013e3181644669] [ Links ]
12. Fuchs EJ, Lee LA, Torbenson MS, et al. Hyperosmolar sexual lubricant causes epithelial damage in the distal colon: Potential implication for HIV transmission. J Infect Dis 2007;195(5):703-710. [http://dx.doi.org/10.1086/511279] [ Links ]
13. Leyva FJ, Bakshi RP, Fuchs EJ, et al. Isoosmolar enemas demonstrate preferential gastrointestinal distribution, safety, and acceptability compared with hyperosmolar and hypoosmolar enemas as a potential delivery vehicle for rectal microbicides. AIDS Res Hum Retroviruses 2013;29(11):1487-1495. [http://dx.doi.org/10.1089/AID.2013.0189] [ Links ]
14. Begay O, Jean-Pierre N, Abraham CJ, et al. Identification ofpersonal lubricants that can cause rectal epithelial cell damage and esnhance HIV type 1 replication in vitro. AIDS Res Hum Retroviruses 2011;27(9):1019- 1024. [http://dx.doi.org/10.1089/AID.2010.0252] [ Links ]
15. Butler LM, Osmond DH, Jones AG, Martin JN. Use of saliva as a lubricant in anal sexual practices among homosexual men. J Acquir Immune Defic Syndr 2009;50(2):162-167. [http://dx.doi.org/10.1097/QAI.0b013e31819388a9] [ Links ]
16. Lane T, Raymond F, Dladla S, et al. High HIV prevalence among men who have sex with men in Soweto, South Africa: Results from the Soweto men's study. Aids Behav 2009;15(3):626-634. [http://dx.doi.org/10.1007/s10461-009-9598-y] [ Links ]
17. US Centers for Disease Control and Prevention. Sexually Transmitted Diseases Treatment Guidelines. Atlanta, CDC: 2006;55:1-100. http://www.cdc.gov/std/treatment/2006/default.htm (accessed 21 November 2013). [ Links ]
18. World Health Organization. Prevention and Treatment of HIV and Other Sexually Transmitted Infections Among Men Who Have Sex With Men and Transgender People. Recommendations for a Public Health Approach 2011. 2 July 2012. http://www.who.int/hiv/pub/guidelines/msm_guidelines2011/en/ (accessed21 November 2013). [ Links ]
19. IRMA. International Rectal Microbicides Advocates. http://www.rectalmicrobicides.org (accessed 21 November 2013). [ Links ]
 Correspondence:
Correspondence:
K B Rebe
(rebe@anovahealth.co.za)
Accepted 17 September 2013


{kind=link}