










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSAMJ: South African Medical Journal
versión On-line ISSN 2078-5135
versión impresa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.104 no.1 Pretoria ene. 2014
RESEARCH
Prevalence and incidence of symmetrical symptomatic peripheral neuropathy in patients with multidrug-resistant TB
F ConradieI, II; T MabiletsaIII; M SefokaIII; S MabasoIII; R LouwIV; D EvansV; A van RieVI
IMB ChB Clinical HIV Research Unit, Department of Medicine, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
IIMB ChB Right to Care, Johannesburg, South Africa
IIIRight to Care, Johannesburg, South Africa
IVMB ChB. Sizwe Tropical Disease Hospital, Gauteng Department of Health, Johannesburg, South Africa
VD Biomed. Health Economics and Epidemiology Research Office, Department of Medicine, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa
VIMD, PhD Department of Epidemiology, University of North Carolina, Chapel Hill, USA
ABSTRACT
BACKGROUND: Symptomatic symmetrical peripheral neuropathy (SSPN) is common in patients with HIV infection. It is also a common adverse event associated with both tuberculosis (TB) treatment and antiretroviral therapy (ART), particularly stavudine. While tenofovir is the one of recommended first-line nucleotide reverse transcriptase inhibitors (NRTIs), there is a risk of nephrotoxicity when using tenofovir together with the aminoglycosides needed to treat multidrug-resistant (MDR) TB. Thus, stavudine is often chosen as a treatment option for the HIV-infected MDR TB patient.
OBJECTIVE: To assess whether use of stavudine both before and during treatment for MDR TB increased the prevalence and incidence of SSPN.
METHOD: MDR TB patients at Sizwe Tropical Disease Hospital were examined for signs of prevalent SSPN. Age, gender, HIV status, alcohol use, TB and HIV treatment regimens both prior to admission and current, and concomitant medications were recorded.
RESULTS: In this cohort of 246 patients, we found that 24.4% of patients with MDR TB had SSPN at time of admission for treatment of MDR TB. They were more likely to be HIV-infected (odds ratio (OR) 3.21; 95% CI 1.25 - 8.21) and tended to have longer (>7 months) exposure to stavudine (OR 1.81; 95% CI 0.90 - 3.63). Incident SSPN occurred in 17% of patients and was associated with older age (hazard ratio (HR) 3.00; 95% CI 1.30 - 6.89) and exposure to terizidone (HR 2.98; 95% CI 0.94 to 4.61) or, to a lesser extent, with stavudine (crude HR 1.62; 95% CI 0.65 - 4.01) in the first 6 months of MDR TB treatment. This common adverse event emphasises the need for the development of less toxic drugs for the treatment of MDR TB.
South Africa (SA) has the fourth-highest incidence of multidrug-resistant (MDR) TB worldwide![1] with significant numbers of patient co-infected with HIV At present, treatment of MDR TB is characterised by toxic medications, given for prolonged periods of time, and which have poorer efficacy than those used for drug-sensitive TB.
One of the mainstays of MDR TB treatment, the aminoglycosides, can cause tubular necrosis[2] which results in functional nephrotoxicity.[3] For patients who are co-infected with MDR TB and HIV, the National Department of Health guidelines recommend they be started on antiretroviral therapy (ART) irrespective of their CD4+ count. These guidelines also suggest the use of a tenofovir-based first-line ART regimen, which is associated with renal dysfunction. Because tenofovir-related nephrotoxicity is characterised by proximal tubular cell dysfunction,[4] there is concern that the cumulative action of aminoglycosides and tenofovir may put patients at risk of renal failure. Zidovudine can be an alternative for tenofovir but the high incidence of anaemia in this population often precludes its use. Consequently, stavudine is often used in HIV-infected patients with MDR TB. However, the use of 30 mg stavudine twice daily for 6 months during the injectable intensive phase could potentially result in mitochondrial toxicity and symptomatic symmetrical peripheral neuropathy (SSPN). We report on the prevalence and incidence of SSPN in a cohort of MDR TB patients admitted to an inpatient facility in Gauteng Province, and assess the effect of stavudine.
Methods
Sizwe Tropical Disease Hospital is the referral facility for MDR TB treatment in Gauteng Province, South Africa. Patients are admitted here if they have resistance to isoniazid (INH) and rifampicin confirmed either by line probe assay or culture and drug sensitivity testing. All patients receive HIV counselling and testing and are managed according to national guidelines.[5]
Criteria for enrolment in this prospective cohort were a confirmed diagnosis of MDR TB, ability and willingness to provide written informed consent and being 18 years or older.
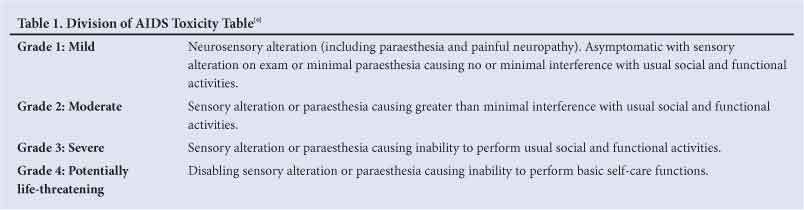
At admission, consenting patients were asked about symptoms of, and were examined for signs of, prevalent SSPN. The examination was conducted by the medical officer and included an assessment of fine-touch, pin-prick and vibration sense. Participants were considered to have SSPN if they had at least one symptom (burning, pain, numbness, or pins and needles) or one clinical sign of neuropathy (reduced vibration sense or absent ankle reflexes) in both legs. The grading was according to the Division of AIDS Toxicity Table (see Table 1).[6]
The results were not confirmed by nerve conduction studies, as the expertise and equipment needed are not available on site, and infection control concerns precluded transporting a patient to another site. Participants were assessed for incident peripheral neuropathy weekly for the first 4 weeks and monthly thereafter.
Age, gender, HIV status, alcohol use, TB and HIV treatment regimens both prior to admission and current, and concomitant medications were recorded. The association between potential risk factors and prevalent SSPN was estimated using odds ratio (OR) with 95% confidence intervals (CIs). Factors associated with incident SSPN were estimated as hazard ratios (HRs) using Cox proportional hazard models.
Ethical approval for the study was granted by the Human Research Ethics Committee of the University of the Witwatersrand.
Results
Between August 2009 and August 2011, 284 adults with MDR TB were admitted to Sizwe Tropical Disease Hospital, of whom 246 (87%) consented to participate in the study. Median age was 37 years and 54% were female; 81% were HIV-infected with median CD4+ count of 200.5 cells/µl (interquartile ratio (IQR) 98.75 - 267.25). Few (3.3%) patients reported excessive alcohol use. At admission, 35.7% (n=88) were already on ART. Median duration of exposure to stavudine was 7.4 months (IQR 2.2 - 24.5) and median exposure time to INH was 6 months (IQR 3 - 6).
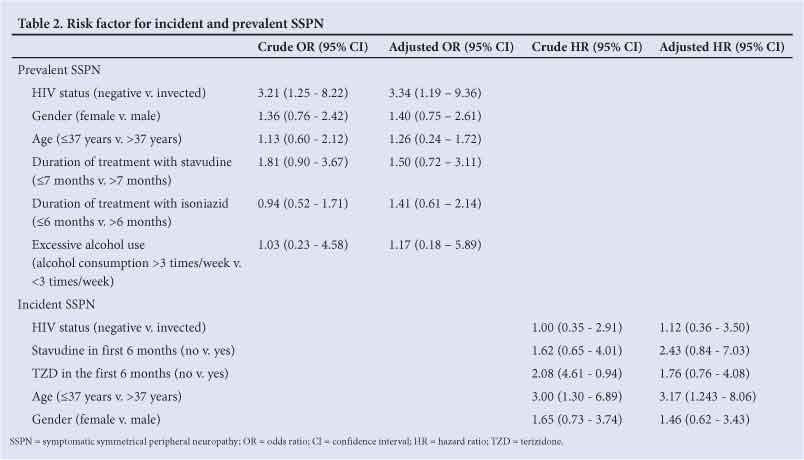
Sixty (24.4%) patients had SSPN at time of admission. In bivariate analysis, prevalent SSPN cases were more likely to be HIV-infected (OR 3.21; 95% CI 1.25 - 8.21) and tended to have longer (>7 months) exposure to stavudine (OR 1.81; 95% CI 0.90 - 3.63). However, they were similar to those without prevalent SSPN with regards to gender (OR 1.36; 95% CI 0.76 - 2.42), excessive alcohol use (OR 1.03; 95% CI 0.23 - 4.58) ), age above 37 years (OR 1.12; 95% CI 0.60 - 2.12), and duration of exposure to INH for >6 months (OR 0.94; 95% CI 0.52 - 1.71) (Table 2). HIV infection remained significantly associated with prevalent SSPN in multivariate analysis (adjusted OR) 3.34; 95% CI 1.19 - 9.36).
The 186 patients free of SSPN at baseline were followed up for a median of 452 days, (IQR 312 to 628 days). Thirty-one (16.7%) developed incident SSPN after a median of 40 days (IQR 23 - 108) days), corresponding to an incidence rate of 12.9 per 100 person-years. Incident SSPN was associated with older age (HR 3.00; 95 CI 1.30 - 6.89) and tended to be associated with exposure to terizidone (HR 2.98; 95% CI 0.94 - 4.61) or stavudine (Crude HR 1.62; 95% CI 0.65 - 4.01) in the first 6 months of MDR TB treatment. Incident SSPN was not associated with HIV infection (HR 1.00; 95% CI 0.36 - .91). In multivariate analysis, older age remained an independent risk factor for incident SSPN (adjusted HR 3.174; 95% CI 1.243 - 8.06).
Discussion
SSPN was common among patients admitted for MDR TB treatment, with a prevalence of 24.4% and incidence rate of 12 per 100 person-years.
We found that HIV infection was independently associated with prevalent SSPN, but was not associated with incident SSPN. HIV- associated SSPN has been associated with low CD4+ count and a high viral load, suggesting a possible reduction in risk when ART is initiated early.[7]
Duration of exposure to INH prior to admission was not associated with increased prevalence of SSPN in our cohort. However, the frequency of INH-associated SSPN has been shown to be mediated by HIV infection, with HIV-infected TB patients having a fourfold higher risk.[8] INH-associated SSPN is also dose-related, with 2 - 12% of patients receiving 3 - 5 mg/kg/day INH developing SSPN, compared with 44% of those receiving 16 - 24 mg/kg/day.[9] We could not assess the effect of INH dosage in this cohort as only 4 patients received a high dose of INH for treatment of MDR TB.
Exposure to stavudine is a well-documented risk factor for SSPN[10,11] and tended to increase the risk of SSPN in our study cohort. However, compared with the risk of renal disease, this was not considered to be sufficient reason not to use stavudine.
Terizidone may further increase the risk of INH-associated SSPN as it inhibits pyridoxine activity.[9] Terizidone-associated nervous system toxicities have been reported, usually within the first 2 weeks, but rarely include SSPN. In our cohort, exposure to terizidone tended to increase the risk of incident SSPN, but this was not statistically significant.
Study limitations
Very ill and confused patients could not provide consent and were excluded, which may have led to an underestimation of the rate of SSPN. The diagnosis of SSPN was based on clinical examination only, as we did not have the capacity to perform electrophysiological studies.
References
1. World Health Organization. Multidrug and extensively drug-resistant TB (M/XDR-TB): 2010 global report on surveillance and response. Geneva: WHO, 2010. http://whqlibdoc.who.int/publications/2010/9789241599191_eng.pdf (accessed 28 February 2013). [ Links ]
2. Mingeot-Leclercq MP, Tulkens PM. Aminoglycosides: Nephrotoxicity. Antimicrob Agents Chemother 1999;43(5):1003-1012. [ Links ]
3. Walker RJ, Duggin GG. Drug nephrotoxicity. Ann Rev Pharmacol Toxicol 1988;28:331-345. [ Links ]
4. Fernandez-Fernandez B, Montoya-Ferrer A, Sanz AB, et al. Tenofovir nephrotoxicity: 2011 update. AIDS Research and Treatment. 2011, Article ID 354908. [http://dx.doi.org/10.1155/2011/354908] [ Links ]
5. South African Department of Health. Management of Drug Resistant Tuberculosis: Policy Guidelines. Pretoria: NDoH, 2012. http://www.doh.gov.za/docs/policy/2012/TBpolicy.pdf (accessed 27 August 2013). [ Links ]
6. US National Institute of Allergy and Infectious Diseases Division of AIDS. The Division of AIDS Table for Grading the Severity of Adult and Pediatric Adverse Events. Bethesda: DAIDS, 2004. http://rsc.tech-res.com/Document/safetyandpharmacovigilance/Table_for_Grading_Severity _of_Adult_Pediatric_Adverse_Events.pdf (accessed 2 September 2013). [ Links ]
7. Childs EA, Lyles RH, Selnes OA, et al. Plasma viral load and CD4 lymphocytes predict HIV-associated dementia and sensory neuropathy. Neurology 1999;52(3):607-613. [ Links ]
8. Marks DJ, Dheda K, Dawson R, Ainslie G, Miller RF. Adverse events to antituberculosis therapy: Influence of HIV and antiretroviral drugs. Int J STD AIDS 2009;20:339-345. [http://dx.doi.org/10.1258/ijsa.2008.008361] [ Links ]
9. van der Watt JJ, Harrison TB, Benatar M, Heckmann JM. Polyneuropathy, anti-tuberculosis treatment and the role of pyridoxine in the HIV/AIDS era: A systematic review. In J Tuberc Lung Dis 2011;15(6):722-728. [http://dx.doi.org/10.5588/ijtld.10.0284] [ Links ]
10. Evans, SR, Ellis RJ, Chen H, et al. Peripheral neuropathy in HIV: Prevalence and risk factors. AIDS 2011;25(7):919-928. [http://dx.doi.org/10.1097/QAD.0b013e328345889d] [ Links ]
11. Wadley AL, Cherry CL, Price P, Kamerman PR. HIV neuropathy risk factors and symptom characterization in stavudine-exposed South Africans. J Pain Symptom Manage 2011;41(4):700-706. [http://dx.doi.org/10.1016/j.jpainsymman.2010.07.006] [ Links ]
 Correspondence:
Correspondence:
F Conradie
(fconradie@witshealth.co.za)
Accepted 30 October 2012


{kind=link}
{kind=link}