










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSAMJ: South African Medical Journal
versão On-line ISSN 2078-5135
versão impressa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.104 no.1 Pretoria Jan. 2014
RESEARCH
Extrapulmonary tuberculosis among adults: Experience at Chris Hani Baragwanath Academic Hospital, Johannesburg, South Africa
A S Karstaedt
MB BCh, MMed Division of Infectious Diseases, Department of Medicine, Chris Hani Baragwanath Hospital and University of the Witwatersrand, Johannesburg, South Africa
ABSTRACT
BACKGROUND: Extrapulmonary tuberculosis (EPTB) occurs in 15 - 20% of immunocompetent and 20 - 70% of HIV-infected patients with tuberculosis. There are few recent incidence data for EPTB.
METHODS: Adults (N=2 963) with culture-proven EPTB seen over 2 years at Chris Hani Baragwanath Academic Hospital, the main referral hospital serving Soweto, Johannesburg, South Africa, were retrospectively studied for pattern and incidence.
RESULTS: The commonest sites of EPTB were the pleura (39.1%), lymph nodes (31.0%), blood (21.8%), meninges (7.3%), and peritoneum (2.9%). Disseminated tuberculosis occurred in 25.0%. The median age was 33 years (range 18 - 87 years). Males comprised 53.2% overall, with a female majority in the peritonitis group. For Soweto, the incidence of adult EPTB was 88.6/100 000 population, rising to 139.4/100 000 and 125.7/100 000 in the 25 - 34-year and 35 - 44-year age groups, respectively. There was no secondary peak in the elderly (17.9/100 000).
CONCLUSIONS: This retrospective cohort showed a high incidence of EPTB, most marked in the 25 - 44-year age group. Culture of extrapulmonary sites is of importance to confirm diagnosis of tuberculosis and to ensure antituberculosis drug susceptibility testing.
Extrapulmonary tuberculosis (EPTB) occurs in 15 - 20% of immunocompetent and 20 - 70% of HIV-infected patients with tuberculosis (TB).[1] There are few recent incidence data for EPTB. In the USA, incidence rates were 5.93/100 000 population in black males in Tennessee and 209/100 000 among Somalis in Minnesota.[2,3] In Sao Paulo, Brazil, the incidence of pleural TB was 3.8/100 000.[4] Incidence rates for EPTB from sub-Saharan Africa, where high rates of co-infection with human immunodeficiency virus (HIV) and TB exist, are lacking. The diagnosis of EPTB is more difficult than that of pulmonary TB because fewer bacilli are present and specimen material in extrapulmonary sites of disease is less easily accessible. While TB diagnosis rests on at least one of the triad of mycobacterial culture, histopathology and suggestive clinical criteria, only culture offers an unequivocal result. Positive mycobacterial culture results are reported as 79% and 82% in separate studies from the USA, and as 14% in Brazil.[2-4] In Soweto in 2001, 30% of 990 patients had EPTB.[5] This paper describes the frequency of culture-proven EPTB over a 2-year study period and documents the incidence of EPTB among adults in Soweto according to age.
Methods
Study site
Chris Hani Baragwanath Academic Hospital, a 2 700-bed public sector university hospital, is the main referral hospital serving Soweto, Johannesburg, South Africa.
Patient population
A retrospective cohort study of adult patients >18 years of age with culture-confirmed tuberculosis in an extrapulmonary site was performed from April 2001 to March 2003. Age, gender and address were noted. HIV serostatus was available for patients with TB meningitis and those with TB bacteraemia.
Microbiology
The central TB laboratory of the National Health Laboratory Service, Johannesburg, utilised liquid culture media, namely BACTEC 13A or BACTEC MYCO/F Lytic (Becton Dickinson), or solid media (Lowenstein-Jensen), depending on the source of the specimen.
Ethics
The study was approved by the Committee for Research on Human Subjects of the University of the Witwatersrand, Johannesburg.
Results
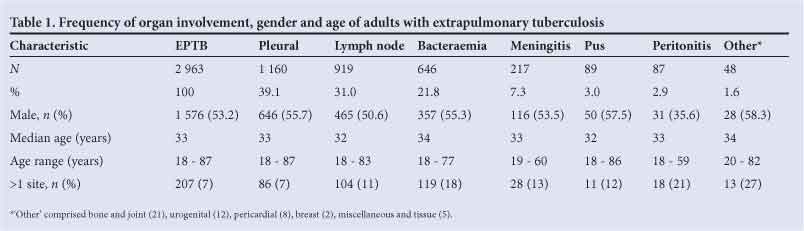
Over the 2-year period of the study, 2963 adults had Mycobacterium tuberculosis cultured from 3 166 extrapulmonary sites (Table 1). The commonest sites were the lymph nodes and pleura, which together accounted for nearly 70% of specimens. A positive TB smear was documented in 370 lymph nodes (40.3%). Disseminated disease (bacteraemia or >1 extrapulmonary organ) was present in 742 patients (25.0%). The site of origin in the 'pus' group was not specified and probably comprised peripheral lymph nodes, superficial skin and soft tissue and deep organ abscesses, and empyema. Males predominated, with gender parity among patients with lymphadenitis and a female preponderance in those with peritonitis. The median age of 33 years was similar across all disease groups. Of the 217 patients with meningitis, 127 (58.5%) were HIV-infected (12 were not tested). Of patients with TB bacteraemia for whom hospital records were available, HIV infection was established in 227 (35%); only 1 patient was known not to be infected with HIV. (It should be noted that while many more had been tested for HIV, the results had in many cases not been documented and had been deleted from the laboratory database.) There were 37 patients aged >65 years (of whom 25 (67.6%) were male); pleural involvement was evident in 22 specimens (59.5%), bacteraemia in 8, lymphadenopathy in 6, and liver involvement, abscess and urinary tract infection in 1 each (2 patients had 2 specimens).
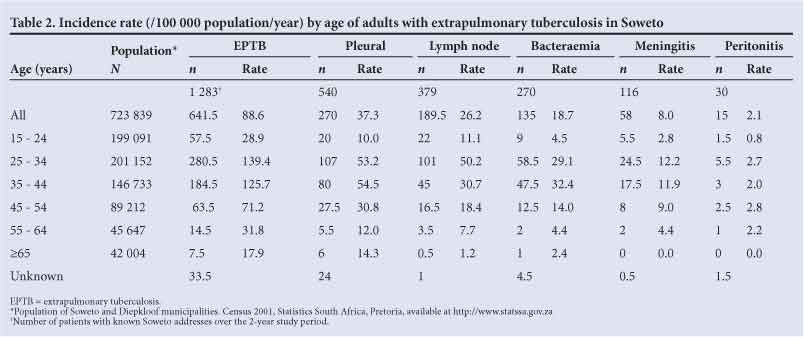
The annual incidence of EPTB by age is presented in Table 2. Of the 2963 patients, 1283 (43.3%) were documented to have addresses in Soweto and 915 (30.9%) had no address available; the remaining patients had been referred to Chris Hani Baragwanath Academic Hospital for diagnostic work-up. The incidence of EPTB in adults based on culture was 88.6/100 000 population, reaching 139.4 and 125.7/100 000, respectively, for 25 - 34-year-olds and 35 - 44-year-olds. There was no secondary peak in the elderly.
Discussion
In this study in a large urban referral hospital with high tuberculosis and HIV prevalence rates, there was an incidence of EPTB of 88.6/100 000 population based on positive TB culture obtained from extrapulmonary sources. This is a minimum estimate of the incidence of EPTB. It would have excluded patients with EPTB in whom the TB diagnosis was made by other diagnostic criteria, from whom an extrapulmonary specimen was not obtained, or in whom the diagnosis was not suspected. Moreover, culture positivity would have varied according to bacillary load. Rates of EPTB were especially high in the 25 - 44-year age group, in which the highest HIV population rates would be expected. The incidence was nevertheless lower than in Somalis in Minnesota, in whom EPTB was commoner than pulmonary tuberculosis and HIV seroprevalence was low. The Soweto incidence of pleural tuberculosis is much higher than that in Brazil.[3,4]
Culture, the most reliable method of diagnosis, depends on specimens being taken. Histological examination is helpful, but there is a wide differential diagnosis for granulomatous disease. These alternatives are often ignored in an endemic TB area. Clinical insight may be flawed and influenced by clinical context and resource restraints, as evidenced in autopsy studies.[6]
In this study, pleural and lymph node tuberculosis rates were similar to those reported from Hong Kong, where 42% had pleural and 37% lymph node tuberculosis.[7] In a composite of several studies of EPTB, lymph node tuberculosis (35%) and pleural tuberculosis (20%) were commonest.[1] Among Somalis in Minnesota, lymph node tuberculosis caused 50% and pleural disease 9% of cases of EPTB. In reports from the USA, TB adenopathy occurred in 40% and pleural disease in 20%, while bacteraemia was the sole proof of disease in 18%.[3,8] The presence of TB bacteraemia has been shown to be an important test in HIV-infected patients, especially those with CD4 counts <100 cells/µl[9] In a retrospective survey of unselected patients in Soweto who were investigated with mycobacterial blood culture, 19% had TB bacteraemia.[10] HIV infection has been negatively associated with a pleural site of EPTB. [11,12] The lack of documentation of HIV status for the group with pleural disease did not allow us to assess this in the study cohort. The slight male predominance found is similar to that in the USA.[8] There was, however, a marked female predominance in patients with tuberculous peritonitis. Abdominal tuberculosis generally occurs equally in both sexes, although some studies report a higher incidence in women.[13]
Limitations of the study include its retrospective nature, and the fact that resistance to anti-TB therapy and HIV status, other than in patients with meningitis and to a lesser extent bacteraemia, were not available. The results of HIV tests, among others, for the period of the study were removed from the laboratory database (and the archived discs proved unreadable). Some organ systems that rely largely on histology or clinical criteria for diagnosis would have been under-represented, including bone and joint, pericardial, gastrointestinal and genitourinary TB.
Although the data are a decade old, they do provide a baseline prior to the advent of widespread provision of antiretroviral therapy at the time of the penultimate published census for South Africa. Furthermore, the numbers of patients with EPTB were similar to those at the hospital in 2006.[10] The high incidence of EPTB, based on culture results, persists.
The importance of culture of material or tissue obtained from extrapulmonary disease sites to confirm diagnosis and ensure anti-TB drug susceptibility testing is emphasised, at least until molecular techniques are validated and widely available.[14]
Acknowledgements. I thank Mani Khoosal and Xoliswa Poswa of the National Health Laboratory Service for provision of culture results and Vanessa Quan of GERMS-SA for assistance with data.
References
1. Sharma SK, Mohan A. Extrapulmonary tuberculosis. Indian J Med Res 2004;120(4):316-353. [ Links ]
2. Fiske CT, Griffin MR, Erin H, et al. Black race, sex, and extrapulmonary tuberculosis risk: An observational study. BMC Infect Dis 2010;10:16. [http://dx.doi.org/10.1186/1471-2334-10-16] [ Links ]
3. Rock RB, Sutherland WM, Baker C, Williams DN. Extrapulmonary tuberculosis among Somalis in Minnesota. Emerg Infect Dis 2006;12(9):1434-1436. [http://dx.doi.org/10.3201/eid1209.050295] [ Links ]
4. Seiscento M, Vargas FS, Rujula MJP, Bombarda S, Uip DE, Galesi VMN. Epidemiological aspects of pleural tuberculosis in the state of Sao Paulo, Brazil (1998-2005). J Bras Pneumol 2009;35(6):548-554. [http://dx.doi.org/10.1590/S1806-37312009000600008] [ Links ]
5. Edginton ME, Wong ML, Phofa R, Mahlaba D, Hodkinson HJ. Tuberculosis at Chris Hani Baragwanath Hospital: Numbers of patients diagnosed and outcomes of referrals to district clinics. Int J Tuberc Lung Dis 2005;9(4):398-402. [ Links ]
6. Cox JA, Lukande RL, Nelson AM, et al. An autopsy study describing causes of death and comparing clinico-pathological findings among hospitalized patients in Kampala, Uganda. PLoS One 2012;7:e33685. [http://dx.doi.org/10.1371/journal.pone.0033685] [ Links ]
7. Noertjojo K, Tam CM, Chan SL, Chan-Yeung MMW Extra-pulmonary and pulmonary tuberculosis in Hong Kong. Int J Lung Dis 2002;6(10):879-886. [ Links ]
8. Peto HM, Pratt RH, Harrington TA, LeBue PA, Armstrong LR Epidemiology of extrapulmonary tuberculosis in the United States, 1993-2006. Clin Infect Dis 2009;49(9):1350-1357. [http://dx.doi.org/10.1086/605559] [ Links ]
9. Jones BE, Young SMM, Antoniskis D, Davidson PT, Kramer F, Barnes PF. Relationship of the manifestations of tuberculosis to CD4 cell counts in patients with human immunodeficiency virus infection. Am Rev Respir Dis 1993;148(5):1292-1297. [ Links ]
10. Edginton ME, Rakgokong L, Verver S, et al. Tuberculosis culture testing at a tertiary care hospital: Options for improved management and use for treatment decisions. Int J Tuberc Lung Dis 2008;12(7):786-791. [ Links ]
11. Alvarez GG, Thembela BL, Muller FJ, Clinch J, Singhal N, Cameron DW. Tuberculosis at Edendale Hospital in Pietermaritzburg, KwaZulu Natal, South Africa. Int J Tuberc Lung Dis 2004;8(12):1472-1478. [ Links ]
12. Leeds IL, Magee MJ, Kurbatova EV, et al. Site of extrapulmonary tuberculosis is associated with HIV infection. Clin Infect Dis 201255(1):75-81. [http://dx.doi.org/10.1093/cid/cis303] [ Links ]
13. Kapoor VK. Abdominal tuberculosis. Postgrad Med J 1998;74(874):459-467. [http://dx.doi.org/10.1136/pgmj.74.874.459] [ Links ]
14. Tortoli E, Russo C, Piereimoni C, et al. Clinical validation of Xpert MTB/RIF for the diagnosis of extrapulmonary tuberculosis. Eur Respir J 2012;40(2):442-447. [http://dx.doi.org/10.1183/09031936.00176311] [ Links ]
 Correspondence:
Correspondence:
A S Karstaedt
(karstaedt@mweb.co.za)
Accepted 24 April 2013


{kind=link}
{kind=link}