










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSAMJ: South African Medical Journal
On-line version ISSN 2078-5135
Print version ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.103 n.11 Pretoria Jan. 2013
EDITOR'S CHOICE
Janet SeggieI; Bridget FarhamII
IEditor-in-Chief
IIDeputy Editor
This issue of the SAMJ deals comprehensively with our 'bad habits' whether smoking, making poor dietary choices or abusing alcohol and other substances, and their downstream health effects.
Somewhat unusually, this issue starts with two guest editorials, one from Leonie Joubert,[1] a well-known science writer who has recently turned her attention to the question of food security in southern Africa. This, paradoxically, fits well into the theme of 'bad habits' as her research shows that the poorest of the poor suffer specifically through their relatively easy access to cheap sources of refined carbohydrates and sugars, with consequent poor micro- and, in many cases, macronutrient intake. This is not so much a 'bad habit' as poor and inadequate diet caused by a combination of poverty, poor city planning and the vested interests of major food retailers and industries. Characteristically, Joubert does not simply report - she suggests practical approaches to relieving this situation.
Smoking and tobacco control
Cigarettes kill over 6 million people each year - almost twice the number that die from HIV and tuberculosis combined. Smoking is strongly associated with the five leading causes of global mortality - ischaemic heart disease, stroke, chronic obstructive pulmonary disease, lower respiratory tract infection and lung cancer. It is estimated that without tobacco, one-third of all cancer deaths would be avoided.
We feature an editorial from Dr Nkosazana Dhlamini Zuma,[2] who, as Minister of Health in the first democratic government, steered through legislation banning the advertising of tobacco products, classifying nicotine as an addictive drug, restricting smoking in public places, and increasing excise duties on cigarettes; as well as interventions at the individual level such as school health education, e.g. changes in the national school curriculum declaring nicotine a drug of addiction, and improving health literacy.
This has escalated into a pan-African view on tobacco control, aimed at protecting Africa's population - set to double by the middle of the 21st century to 2 billion - from being recruited to smoking by the tobacco industry. More than half of this population will be the young people (especially young women) being targeted by the industry.
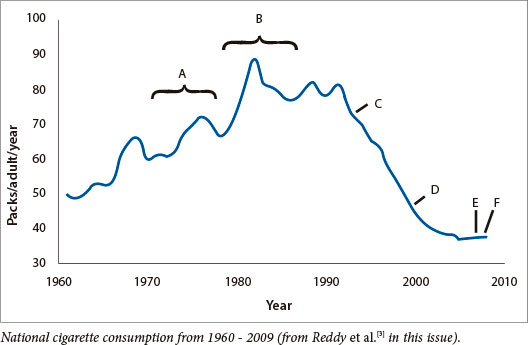
Reddy et al.[3] show that Dr Zuma's comprehensive health-promotion approach to tobacco control can work among school age children in Africa (see figure above). These remarkable changes occurred during a time when smoking among young people was on the rise globally.
Sub-Saharan Africa is still in the early stages of the tobacco epidemic and authorities must intervene now to prevent tobacco-related death, and disease, with the concomitant economic and environmental burden.
The e-cigarette debate
Coinciding with intensifying attempts by government and society to reduce tobacco smoking through stricter limitation on its sale, advertising and use, the popularity of electronic cigarettes (e-cigarettes), which are relatively new in South Africa, is increasing.
Two colleagues, both pulmonologists, present arguments for the potential benefit and harms of e-cigarettes, based on the currently available evidence[4,5]
Our protagonist states that without any form of counselling or incentive, quit rates at one-year were 8.7%, with a further 10.3% having a >50% reduction in smoking. Moreover, 73% of those who gave up smoking at one year had quit the use of e-cigarettes as well.
If e-cigarettes improve quit rates, surely they should be considered, if not embraced. They remain the only currently available therapy that simultaneously addresses both the physical and psychological components of tobacco addiction - assisting smokers in both quitting and cutting down, with the added benefit of avoiding 'passive smoking' by others. Thus, they are safe and effective, and based on the available evidence, the potential benefits must outweigh their risks, especially when compared with the alternative: smoking.
Our antagonist's view is, firstly, that the evidence that e-cigarettes are an effective method for smoking cessation is unconvincing and that there are scant data on efficacy as a bridge to stop smoking; secondly, that they are a means for maintaining nicotine addiction and dependence and thirdly, that they may even encourage more habitual use of nicotine, which in time may encourage a switch to cigarette smoking.
Far from being a 'healthier alternative' -e-cigarettes may induce long-term nicotine addiction, and if this tendency is present, it is so far unaddressed.
The diet-heart hypothesis and obesity
From tobacco to one of the other major consequences of our 'bad habits', obesity -which has been increasing steadily since the publication of the 1977 Dietary Goals for the United States written for the US Select Committee on Nutrition by Nick Mottern, a vegan with no scientific training. The developed, and much of the developing world, has over the past three decades seen an inexorable rise in obesity and all its related diseases while largely adhering to the so-called 'prudent diet' - low in saturated fats and high in carbohydrates. In this issue of the SAMJ, Tim Noakes, no stranger to controversy, has presented a series of reports from people who, suffering from obesity and related diseases, have rejected the conventional approach to diet and weight loss and opted to try what has become known as the 'Noakes diet', with apparant success.[6]
Noakes also provides an insightful critique on the Women's Health Initiative Randomized Controlled Dietary Modification Trial, which looked at the role of diet in the development of major health issues in postmenopausal women, including cardiovascular disease. Noakes suggests that this study challenges the diet-heart hypothesis - that a diet high in saturated fat and cholesterol increases the risks of cardiovascular disease.[7]
The costs of alcohol consumption
No round up of 'bad habits' is complete without mention of alcohol. Sturm et al.[8] discuss the effects of obesity, smoking and excessive alcohol intake on healthcare expenditure in a South African medical scheme. Not surprising, excess alcohol intake, along with smoking, significantly increases healthcare expenditure - obesity doubling these costs.
Harker Burnhams et al.[9] tackle the extent of alcohol and other drug use in the workplace, noting that their use in this setting, although known to have a major impact on the health and productivity of the workforce globally, is under-researched in South Africa. What they found is instructive: employed men misuse alcohol, while the women misuse drugs. Most referrals to Employee Assistance Programmes come from the public, financial and industrial sectors and alcoholand drug-related problems have a major effect on work performance. More research into effective intervention and prevention is needed in this area.
Tilting at windmills in the Eastern Cape
Something remains rotten in our Eastern Cape 'state,' mass-sackings of crooked healthcare officials by a single senior provincial crusader obviously making little difference to systemic dysfunction, death and dying among its people. In Izindaba this month,[9] we wring out what's behind the saturation point that civic organisations and several former African National Congress stalwarts have reached, culminating in a protest march to Bhisho and their release of a horrifying patient-centred probe. Two of the disenchanted newsmakers are former operational chiefs of healthcare delivery in the province and one is a Mandela-era national cabinet minister. National Health Minister, Dr Aaron Motsoaledi's decisive and immediate response has been welcomed, but as you'll read, the 'people's' anger cannot be effectively expressed via the ballot box because our proportional representation system dilutes responsibility to an amorphous 'party', which former Eastern Cape health chief, Dr Siva Pillay, argues merely entrenches endemic corruption-breeding patronage. However, this alone cannot be the reason healthcare delivery has imploded so spectacularly in this picturesque province. A massive contributing factor may well be a blind per-capita-based budget allocation from central government to provinces - regardless of those labouring under a homelands legacy of a backlog in human resources and infrastructure. The problems - and solutions - are political.
1. Joubert L. Food security: The optimal diet for people and the planet. S Afr Med J 2013;103(11):809-810. [http://dx.doi.org/10.7196/SAMJ.7545] [ Links ]
2. Zuma ND. A comprehensive, health promotion approach to tobacco control. S Afr Med J 2013;103(11):831. [http://dx.doi.org/10.7196/SAMJ.7305] [ Links ]
3. Reddy P, James S, Sewpaul R, et al. A decade of tobacco control: The South African case of politics, health policy, health promotion and behaviour change. S Afr Med J 2013;103(11):835-840. [http://dx.doi.org/10.7196/SAMJ.6910] [ Links ]
4. Allwood B. Electronic cigarettes: The potential benefits outweigh the risks. S Afr Med J 2013;103(11):832-833. [http://dx.doi.org/10.7196/SAMJ.7434] [ Links ]
5. van Zyl-Smit RN. Electronic cigarettes: The potential risks outweigh the benefits. S Afr Med J 2013;103(11):833. [http://dx.doi.org/10.7196/SAMJ.7435] [ Links ]
6. Noakes TD. Low-carbohydrate and high-fat intake can manage obesity and associated conditions: Occasional survey. S Afr Med J 2013;103(11):826-830. [http://dx.doi.org/10.7196/SAMJ.7302] [ Links ]
7. Noakes TD. The Women's Health Initiative Randomized Controlled Dietary Modification Trial: An inconvenient finding and the diet-heart hypothesis. S Afr Med J 2013;103(11):824-825. [http://dx.doi.org/10.7196/SAMJ.7343] [ Links ]
8. Sturm R, An R, Maroba J, et al. The effects of obesity, smoking, and excessive alcohol intake on healthcare expenditure in a comprehensive medical scheme. S Afr Med J 2013;103(11):840-844. [http://dx.doi.org/10.7196/SAMJ.7260] [ Links ]
9. Harker Burnhams N, Dada S, Linda B, et al. The extent of problematic alcohol and other drug use within selected South African workplaces. S Afr Med J 2013;103(11):845-847. [http://dx.doi.org/10.7196/SAMJ.7195] [ Links ]
10. Bateman C. Corruption-breeding political patronage an albatross; former Eastern Cape health chief. S Afr Med J 2013;103(1):816-818. [http://dx.doi.org/10.7196/SAMJ.7561] [ Links ]

