










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSAMJ: South African Medical Journal
versión On-line ISSN 2078-5135
versión impresa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.103 no.9 Pretoria ene. 2013
EDITOR'S CHOICE
Trauma: South Africa's other epidemic
Damian Clarke, the guest editor for this issue of the SAMJ, is a young surgeon on the staff of the Pietermaritzburg complex of hospitals, whose current research concerns the strategies required to improve quality of care of injured patients admitted to the emergency centres in our regional and peripheral hospitals.
In SA, injury-related mortality rates are six times, and road traffic injuries double, the global rate.[1]
Traumatic brain injury (TBI), featured in an editorial by Naidoo,[2] is the leading cause of mortality in young people. Primary brain injury occurs at impact and is currently believed to be irreversible.
South Africa (SA) has one of the highest motor vehicle accident (MVA) rates in the world, a study from the Red Cross War Memorial Children's Hospital (RCWMCH)[3] confirms MVAs as one of the major reasons for a high incidence of paediatric brain injury (PTBI). The peak admission age to RCWMCH was 6 years, more boys than girls suffered TBI, most injuries occurred on weekends and the major mechanism of PTBI was pedestrian road traffic accidents.
Unique to SA is that pedestrians account for more than half of all road traffic fatalities. A paper from Nadesan-Reddy and Knight[4] shows how 'traffic calming' near schools in the Durban area cut serious pedestrian-vehicle collisions by 23% and 22%, reducing child injuries and dramatically reducing fatalities by 68% and 50% in Chatsworth and KwaMashu, respectively.
Promoting road safety
An editorial by Sinclair[5] continues the theme of tramatic injuries, showing that traffic injuries are the top cause of premature death in children between the ages of 5 and 14 years and the second highest cause in children between 15 and 18 years. While the majority of deaths involve pedestrians, we dismally fail our children as passengers in our cars and taxis. The law is very clear - all adult occupants (whether front- or back-seat) are obliged to wear seatbelts if they are fitted to the vehicle; it is the driver's legal responsibility to ensure that the passengers are 'buckled up'. However, seatbelt use is not enforced and, in fact, many traffic officials themselves flaunt the law. SA legislation is less clear for children - only children older than 3 years are obliged to utilise seatbelts where there are enough present in a vehicle. Furthermore, babies and young children are commonly, and legally, held in the arms of adult passengers in the mistaken belief that in the event of a collision the child will be safely retained in the adult's arms. This is, of course, a physical impossibility given the force of any impact, when the weight and velocity of an adult body will convert into a force of potentially lethal magnitude. There is ample evidence, however, that adherence to the laws that compel use of seatbelts and child restraints has led to an average 40% - 50% reduction in traffic deaths and injuries across the globe.
Improving access to critical care interventions
The major causes of secondary brain injury associated with TBI are hypotension and hypoxia. In relation to which SA faces the unique challenges of prolonged pre-hospital times and limited access to physicians. In 2008, the Health Professions Council of SA introduced paramedic rapid sequence induction (RSI), the gold standard critical care intervention for emergency airway management.[6]
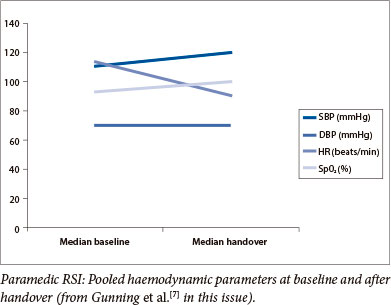
Early access to critical care interventions may improve outcomes for severely ill and injured patients. Gunning et al [7] surveyed 274 945 patients transported to hospital by a private emergency medical service (EMS) over a 2-year period, of whom 86 (0.03%) underwent RSI by paramedics. The 'good shape' in which these trauma victims were in at handover by paramedics to emergency centre personnel is shown in the figure above. Importantly, no patients who underwent RSI died. Nevertheless, the 20% adverse event rate highlights patient safety concerns, and the importance of a robust clinical governance programme to refine practice. The authors recommend that EMS implement an improved Patient Record File - with objective physiological data capture and printouts, including capnography -and a system of patient follow-up that captures patient outcomes to determine the exact role of paramedic RSI in the SA context.
Radiology is key to the early diagnosis and management of the injured. The paper by Hlongwane and Pitcher[8] highlights the deficiency of radiologists in SA, and globally, and confirms the utility of SA radiographers applying the 'red dot' system, used in the United Kingdom since the mid-1980s, for trauma triage. Experienced radiographers evaluating appendicular fractures in adults did as well as consultant radiologists. International experience has shown that radiographer reporting can reduce patient waiting times, release radiologists for other duties and improve the retention of radiographic staff and potentially improve patient care. Radiographers, if they can be shown to accurately identify trauma pathology, can potentially ease service pressures at regional and district public sector hospitals, where there is limited radiologist cover, particularly after-hours. A compelling argument is made for formal extension of the scope of practice of SA radiographers.
Bernon et al.[9] signal 'a worrying reality' in regard to endotracheal tube cuff pressures, which, in the trauma unit and emergency setting, are often unacceptably high. Many patients are hypotensive and particularly susceptible to tracheal mucosal ischaemia, and, potentially, to the life-threatening complication of tracheal stenosis. Such stenosis may present weeks to months after intubation, often as an airway emergency, and is difficult and costly to treat.
In a prospective study conducted over a year in the Northern Cape Province, Bezuidenhout et al.[10] succeeded in developing an accurate, unifying clinical guideline - the Kimberley Hospital Rule (KHR) -that optimises the utilisation of CT scanning of the brain (CTB) in a resource-limited environment. This is applicable to management of any patient over the age of 16 years presenting to hospital with intracranial symptoms, regardless of aetiology. The KHR was shown to be 100% sensitive in the trauma cohort, making it potentially universally applicable in both well-resourced and resource-limited settings. Sensitivity for the non-trauma group was less than that for the trauma group, but as stated by Benatar et al.,[11] 'resource-limited tertiary-care institutions must try to provide the best possible results, both for individual patients and for society as a whole, with their shrinking resources'.
The prevalence of helminth infections
Two case reports[12] highlight a potential endemic focus of human fascioliasis in the Eden district of the Western Cape. Both patients ingested watercress bought from local markets. The perception that fascioliasis is rare or non-existent in SA is likely to result in a delay to diagnosis, and morbidity and mortality. The accompanying editorial[13] asks 'How many cases of fascioliasis are we missing?'
Building life-rafts with one finger in the dyke?
With 1 000 extra Cuban-trained South African medical students added annually to the sixth-year complements of what will hopefully be nine local medical campuses from 2018, medical deans have their work cut out to belatedly begin catering for our healthcare needs. Faced with an unprecedented doctor shortage crisis, the government is putting huge pressure on schools to expand overall output capacity, and the 'Cuban solution,' a temporary measure to win them preparation time. Drawing comparisons with the Eskom capacity debacle, Professor Dan Ncayiyana, Editor Emeritus of this magazine and chief chaperone of the incipient Limpopo medical campus, asks testily, 'Why do we continue to believe that colonial-era institutions will produce milk and honey until kingdom come?'
Too few, inappropriately-trained and very late, the Cuban-trainees, over 300 of whom have graduated so far, are de facto the only game left in town, due to the training incapacity of all South African Development Community medical schools, reports Izindaba[14] in a thorough in-depth look at the controversial programme. Government thinking seems to be that the Cuban-training dovetails neatly with the preventative, primary healthcare approach underpinning our budding National Health Insurance - but our hugely skewed public/ private healthcare system will need to be put to rights first.
Janet Saggie
1. Norman R, Matzopoulos R, Groenewald P, Bradshaw D. The high burden of injuries in South Africa. Bull World Health Organ 2007;85(9):695-702. [http://dx.doi.org/10.2471/BLT.06.037184; [ Links ]
2. Naidoo D. Traumatic brain injury: The South African landscape. S Afr Med J 2013;103(9):613-614. [http://dx.doi.org/10.7196/SAMJ.7325] [ Links ]
3. Schrieff LE, Thomas KGF, Dollman AK, Rohlwink UK, Figaji AA. Demographic profile of severe traumatic brain injury admissions to Red Cross War Memorial Children's Hospital, 2006 - 2011. S Afr Med J 2013;103(9):616-620. [http://dx.doi.org/10.7196/SAMJ.7137] [ Links ]
4. Nadesan-Reddy N, Knight S. The effect of traffic calming on pedestrian injuries and motor vehicle collisions in two areas of the eThekwini Municipality: A before-and-after study. S Afr Med J 2013;103(9):621-625. [http://dx.doi.org/10.7196/SAMJ.7024] [ Links ]
5. Sinclair M. The promotion of road safety by healthcare professionals in South Africa. S Afr Med J 2013;103(9):614-615. [http://dx.doi.org/10.7196/SAMJ.7335] [ Links ]
6. Stein C, Botha M, Kramer E, et al. Position statement: Pre-hospital rapid sequence intubation. S Afr Med J 2011;101(3):163. [ Links ]
7. Gunning M, Perkins Z, Crilly J, von Rahden R. Paramedic rapid sequence induction (RSI) in a South African emergency medical service: A retrospective observational study. S Afr Med J 2013;103(9):632-637.[http://dx.doi.org/10.7196/SAMJ.6656] [ Links ]
8. Hlongwane ST, Pitcher RD. Accuracy of after-hour 'red dot' trauma radiograph triage by radiographers in a South African regional hospital. S Afr Med J 2013;103(9):638-640. [http://dx.doi.org/10.7196/SAMJ.6267] [ Links ]
9. Bernon JK, McGuire C, Carrara H, Lubbe D. Endotracheal tube cuff pressures - the worrying reality: A comparative audit of intra-operative versus emergency intubations. S Afr Med J 2013;103(9):641-643. [http://dx.doi.org/10.7196/SAMJ.6638] [ Links ]
10. Bezuidenhout AF, Hurter D, Maydell AT, et al. The Kimberley Hospital Rule (KHR) for urgent computed tomography of the brain in a resource-limited environment. S Afr Med J 2013;103(9):646-651. [http:// dx.doi.org/10.7196/SAMJ.6876] [ Links ]
11. Benatar SR, Fleischer TE, Peter JC, et al. Treatment of head injuries in the public sector in South Africa. S Afr Med J 2000;90(8):790-793. [ Links ]
12. Black J, Ntusi N, Stead P, Mayosi B, Mendelson M. Human fascioliasis in South Africa. S Afr Med J 2013;103(9):658-659. [http://dx.doi.org/10.7196/SAMJ.7184] [ Links ]
13. Frean J, Mendelson M. We don't see that in South Africa'. S Afr Med J 2013;103(9):612. [http://dx.doi.org/10.7196/SAMJ.7334] [ Links ]
14. Bateman C. Doctor shortages; unpacking the 'Cuban solution'. S Afr Med J 2013;103(9):603-605. [http://dx.doi.org/10.7196/SAMJ.7323] [ Links ]

Damian Clarke* graduated from Wits in 1992. He is a specialist surgeon and senior lecturer at the Department of General Surgery, Nelson Mandela School of Medicine, University of KwaZulu-Natal and serves as Academic Director of the Pietermaritzburg Metropolitan Trauma Service. He is the author of 40 publications and 13 case reports in peer-reviewed journals and presents regularly at medical scientific meetings and conferences. He currently is pursuing research leading to his PhD entitled ‘A multi-faceted approach to improving trauma care in the periphery’.

Dinesh Naidoo* qualified at Wits in 1995. Having undertaken registrar training principally at Baragwanath Hospital, he obtained the Fellowship of the College of Neurosurgeons (FC Neurosurg (SA)) in 2004. He considers himself a general neurosurgeon with special interests in vascular neurosurgery, neuro-oncology and neurotrauma and is currently on the staff at Charlotte Maxeke Johannesburg Academic Hospital. He collaborates with the Department of Pharmacology in investigating advanced and novel drug delivery systems using nanotechnology (and has 4 patents pending). He has published a number of articles in international peer-reviewed journals.

