










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSAMJ: South African Medical Journal
versión On-line ISSN 2078-5135
versión impresa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.103 no.7 Pretoria jul. 2013
RESEARCH
Otolaryngological and head and neck manifestations in HIV-infected patients seen at Steve Biko Academic Hospital in Pretoria, South Africa
M TshifularoI, II; L GovenderIII, IV; G MonamaV, VI
IMB ChB, FCS (SA) ORL, MMed (ORL). Tertiary Referral Centre, Steve Biko Academic Hospital, Pretoria, South Africa
IIMB ChB, FCS (SA) ORL, MMed (ORL). Department of Otorhinolaryngology, Faculty of Health Sciences, University of Pretoria, South Africa
IIIMB ChB, MMed, FCORL. Tertiary Referral Centre, Steve Biko Academic Hospital, Pretoria, South Africa
IVMB ChB, MMed, FCORL. Department of Otorhinolaryngology, Faculty of Health Sciences, University of Pretoria, South Africa
VMB ChB, MMed. Tertiary Referral Centre, Steve Biko Academic Hospital, Pretoria, South Africa
VIMB ChB, MMed. Department of Otorhinolaryngology, Faculty of Health Sciences, University of Pretoria, South Africa
ABSTRACT
BACKGROUND: Sub-Saharan Africa has the highest incidence of HIV infection. According to recent census statistics, 5.6 million people in South Africa (SA) are HIV-positive, the highest number of infected individuals worldwide. Over 80% of HIV-infected individuals will present with ear, nose and throat (ENT) manifestations. Previous studies show that oral diseases seem to be the most common ENT-related manifestation, reported in about 40 - 50% of HIV-infected patients. In SA, there is lack of local information regarding the otolaryngological and head and neck manifestations in HIV-infected individuals.
OBJECTIVE: To ascertain our local trends of ENT and head and neck manifestations in HIV-infected patients seen at our specialised ENT-HIV Clinic, Steve Biko Academic Hospital, Pretoria, Gauteng Province, SA.
METHODS: A 1-year prospective study involving 153 HIV-infected patients was conducted in the clinic from January to December 2011. Patient history was taken and examinations were performed based on the World Health Organization (WHO) HIV/AIDS classification system. Data analysis was performed using Epi Info 7 software.
RESULTS: The most common manifestations were adenoid hypertrophy/hyperplasia followed by cervical lymphadenopathy, chronic suppurative otitis media, otitis media with effusion and sensory-neural hearing loss.
CONCLUSION: Patients typically presented with early manifestations during symptomatic WHO stages I and II in contrast to results reported in similar developing world studies from Iran, Nigeria and India. A possible explanation may lie in the SA government HIV Counselling and Testing campaign and the antiretroviral rollout programme, the effectiveness of which is becoming evident.
The link between ear, nose and throat (ENT) disease and HIV infection has been well established. Over 80% of HIV-infected individuals will present with ENT symptoms at some point during the course of their disease.[1]
The highest incidence of HIV infection is recorded in sub-Saharan Africa (SSA), accounting for almost two-thirds of the world's HIV-infected individuals, the majority of these cases being women.[2]-According to the 2009 census statistics, an estimated 5.6 million people were living with HIV in South Africa (SA),[3] the highest number of infected individuals worldwide, and it was estimated that 310 000 people in SA died of AIDS-related diseases. The highest prevalence was among people between the ages of 15 - 49 years, with younger adults being particularly affected.[3,4] The SA government launched the HIV Counselling and Testing (HCT) campaign in 2010 to highlight peoples' experiences and expel the myths and stigmas of HIV among people in the communities.[5,6] Strategies included increasing the availability of free testing and counselling at clinics, media exposure, door-to-door campaigns and billboard messages.
A number of studies have revealed that oral diseases seem to be the most common ENT-related manifestation, reported in about 40 - 50% of HIV-infected patients. Among these, oral candidiasis was the most prevalent. Sinusitis had the highest prevalence of the rhinological manifestations, ranging from 11 to 70% in different studies. Cervical lymphadenopathy can occur in up to 70% of HIV-infected individuals and is the primary manifestation in the head and neck category of disease. Otitis media ranges from 13 to 40%, closely followed by sensory-neural hearing loss and otitis externa.[7,8] There is lack of local information from SSA and SA regarding the otolaryngological (or ENT) and head and neck manifestations in HIV-infected individuals.
Objective
To ascertain local trends of common ENT and head and neck manifestations in HIV-infected patients seen at our specialised ENT-HIV Clinic at the Steve Biko Academic Hospital, Pretoria, Gauteng Province, SA.
Methods
A 1-year prospective study was undertaken from January 2011 to December 2011 among HIV-infected outpatients attending the ENT-HIV clinic. Some patients were established on antiretroviral (ARV) therapy at the time of presentation. A datasheet was used for collection of patient history, CD4 count, ARV therapy and results of ENT and head and neck examinations, based on the World Health Organization (WHO) HIV/AIDS classification system. Epi Info software (version 7.1.1.14) was used for analysis of trends, mean and frequencies.
This study was approved by the Medical Research Ethics Committee, University of Pretoria.
Results
A total of 153 patients were included in the study, with a male (41.18%; n=63) to female (58.82%; n=90) ratio of 1:1.4. Patients ranged in age from 1 to 76 years (mean ± standard deviation, 31.5±15.52 years). The CD4 counts ranged from 3 to 2 463 cells/mm3.
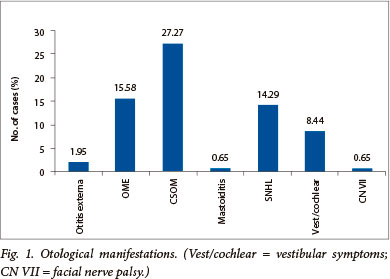
The most common otological manifestation was chronic suppurative otitis media (CSOM), which affected 27% (n=42) of patients; followed by otitis media with effusion (OME) (15.58%; n=24), sensory-neural hearing loss (SNHL) (14.29%; n=22), vestibular symptoms (vertigo) (8.44%; n=13), otitis externa (1.95%; n=2) and facial nerve palsy associated with mastoiditis (0.65%; n=1) (Fig. 1).
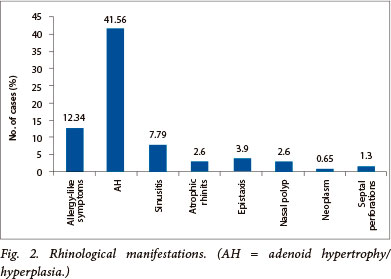
Rhinological manifestations included adenoid hypertrophy/ hyperplasia (41.56%; n=64), allergy-like symptoms (12.34%; n=19), sinusitis (7.79%; n=12), epistaxis (3.9%; n=6), atrophic rhinitis (nose bleeding) (2.6%; n=4), nasal polyposis (2.6%; n=4), septal perforations (1.3%; n=2) and nasal neoplasm (inverting papilloma) (0.65%; n=1) (Fig. 2).
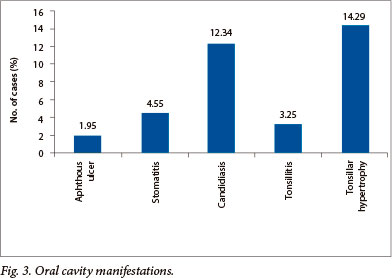
Tonsillar hypertrophy was the most common oral cavity manifestation (14.29%; n=22); followed by oral candidiasis (12.34%; n=19) - the pseudomembranous type being the most common (83% of cases) with 1 case each of angular cheilitis and the erythematous form, stomatitis (4.55%; n=7), tonsillitis (3.25%; n=5) and aphthous ulcers (1.95%; n=3) (Fig. 3).
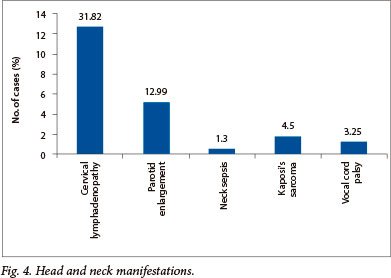
Among the head and neck manifestations (31.82%; n=49), cervical lymphadenopathy with posterior triangle nodes (39%) was the most common; followed by parotid gland cystic enlargement, primarily due to lymphoepithelial cysts (12.99%; n=20); Kaposi's sarcoma (4.5%; n=10); laryngitis (3.25%; n=5) comprising vocal cord palsies (presenting as hoarseness of the voice) and squamous cell carcinoma of the larynx and neck sepsis (cervical abscess) due to lymphadenitis (1.3%; n=2) (Fig. 4).
Discussion
Otolaryngology manifestations are recognised as common early presentations of HIV infection. Of HIV-infected patients, 80 - 100% will present to the ENT clinic with early or late manifestations.[2,7,9,10]
Previous studies have shown that oral manifestations are the most frequently presented symptoms, followed by cervical head and neck lymphadenopathy, sinusitis and otitis media.[1,2,9]
No study of this nature has been conducted in SA; however, studies encompassing 1 155 patients from 3 developing countries; namely Nigeria (n=89), Iran (n=98) and India (n=968), have been conducted.[1,2,11]
In contrast to these studies, females were in the majority in our study. There are several potential reasons for this predominance: it might reflect the SA migrant labour system where males work away from home and females are home-bound; women tend to seek medical attention earlier than men; antenatal clinics in SA are well equipped and are excellent for early HIV screening of women in pregnancy and, according to the SA statistical survey in 2012, females outnumber males in the population as a whole.[3]
In our study, the most common otological manifestation was CSOM followed by OME, SNHL and vestibular symptoms. We could not determine a pattern compared with the other studies since each study showed unique patterns of otological manifestations. The Nigerian study showed a high percentage of OME, followed by SNHL, vestibulo-cochlear symptoms (vertigo, tinnitus, and hearing loss) and low yield of CSOM, similar to the India study.[11]
The most common and earliest rhinological manifestation was adenoid hypertrophy/hyperplasia, which may present as nasal blockage, snoring and/or hearing loss from OME - due to eustachian tube obstruction, followed by allergy-like symptoms (rhinitis, sneeze and itchiness) and sinusitis (atrophic rhinitis, epistaxis and blockage).
In the other studies, sinusitis was the most prevalent, followed by allergy-like symptoms and epistaxis.[10,12]
Tonsillar hypertrophy was the most common oral manifestation, followed by candidiasis, stomatitis and aphthous ulcers. In the other developing countries, oral candidiasis was most prevalent, followed by aphthous ulcers and stomatitis.[10,12]
All studies, including ours, showed high rates of cervical lymphadenopathy, head and neck lymph nodes being common signs of systemic disease.[10,12]
However, our study is the only one to have documented parotid gland cystic enlargement, revealing that this is an early (WHO stage I or II) manifestation, when immunity is well preserved. Moreover, parotid enlargement is known in the community to be associated with HIV; recognising it as a stigma of infection, patients are motivated to seek a diagnosis and possible cosmetic treatment.
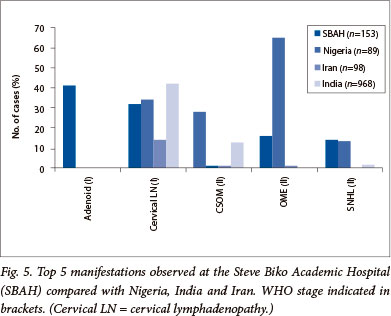
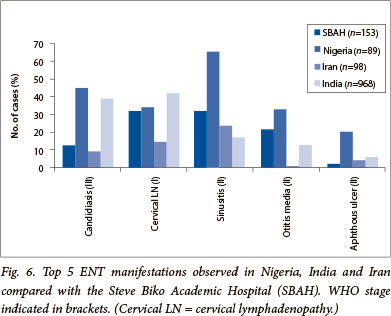
When all presenting conditions were classified according to the WHO stages I - V HIV disease classification, the top 5 manifestations in our study included adenoid hypertrophy/hyperplasia (stage I), cervical lymphadenopathy (stage I), CSOM (stage II), OME (stage II) and SNHL (stage II) (Fig. 5). In contrast, the other studies' top 5 manifestations included sinusitis (stage II), oral candidiasis (stage III/ IV), cervical lymphadenopathy (stage I), otitis media (stage II) and aphthous ulcers (stage II/III) (Fig. 6)
Why did our patients present with earlier-stage manifestations compared with the current trend? A few years ago our clinic handled mainly advanced WHO stage IV manifestations and conditions representing unusual opportunistic AIDS-related infections, which are now rarely seen. A tenable explanation would be that there is now good awareness of HIV/AIDS disease manifestations among health-conscious patients in our urban drainage area of Gauteng, with Pretoria as the tertiary referral centre. Moreover, there are large scale, efficient government HCT services and a commendable national ARV public rollout programme. As a result, changes in disease profiles are being observed. Advanced stage IV manifestations and rare AIDS-associated conditions and opportunistic infections are now seldom seen in our ENT clinic.
Limitation
This study offers information on local trends, but is limited to a single ENT tertiary referral clinic in Pretoria. A multi-centred study, involving all tertiary ENT departments and covering all provinces in SA, would yield an improved overall trend analysis.
Conclusion
This Gauteng-based study demonstrated a local trend that differs from experience in other developing countries. Our patients presented with earlier WHO stage I and II diseases compared with similar studies from Iran, Nigeria and India. This may reflect the SA HIV/AIDS strategy and effectiveness of the public ARV rollout programme.
Acknowledgements. We thank Prof. A Mulder, Mrs B Khoele, the patients and nurses of the ENT clinic of the Steve Biko Academic Hospital, Pretoria.
References
1. Jafari S, Razmpa E, Saeedinejad Z, et al. Otolaryngological manifestations in HIV infected patients, Tehran, Iran. J AIDS Clinic Res 2012;3:160. [http://di.doi.org/10.4172/2155-6113.1000160] [ Links ]
2. Prasad HK, Bhojwani KM, Shenoy V, Prasad SC. HIV manifestations in otolaryngology. Am J Otorhinolaryngol 2006;27(3):179-185. [http://dx.doi.org/10.1016/j.amjoto.2005.09.011] [ Links ]
3. Statistics South Africa. Mid-year population estimates: 2010. Pretoria: Statistics South Africa, 2010. http://www.statssa.gov.za/publications/P0302/P03022010.pdf (accessed 20 July 2010). [ Links ]
4. Joint United Nations Programme on HIV/AIDS (UNAIDS). Global report: UNAIDS Report on the Global AIDS Epidemic 2010. Geneva: UNAIDS, 2010. [ Links ]
5. SANAC Secretariat. The national HIV counselling and test campaign strategy. http://www.cabsa.org.za/sites/default/files/HCT%20Campaign%20Strategy%202_3_10%20final.pdf (accessed 1 February 2010) [ Links ]
6. Peltzer K, Matseke G, Mzolo T, Majaja M. Determinates of knowledge of HIV status in South Africa: Results from a population based HIV survey. BMC Public Health 2009;9:174. [http://dx.doi.org/10.1186/1471-2458-9-174. [ Links ]]
7. Iacovou E, Vlastarakos PV, Papacharalampous G, Kampessis G, Nikolopoulos TP. Diagnosis and treatment of HIV associated manifestations in otolaryngology. Infectious Disease Reports 2012;4(1):e9 [http://dx.doi.org/10.4081/idr.2012.e9] [ Links ]
8. Lubbe DE. HIV and ENT. CME 2004;22(5):250-253. [ Links ]
9. Herdman RCD, Foster S, Stafford ND, Pinching AJ. The recognition and management of the otolarynological manifestations of AIDS. Clin Otolaryngol Allied Sci 1989;14(4):323-332. [http://dx.doi.org/10.1111/j.1365-2273.1989.tb00380.x]
10. Viswanatha B, Krishna N. Otolaryngological manifestations of HIV infection. J Hematol Malig 2012;(2)2:33-38. [http://dx.doi.org/10.5430/jhm.v2n2p33] [ Links ]
11. Sulyman AB, Kazeem SA, Abdulrahman A, et al. Otolaryngologic manifestations among HIV/ AIDS patients in a Nigerian tertiary health institution: An update. Int Archiv Otorhinolaryngol 2010;14(4):398-403. [http://dx.doi.org/10.1590/S1809-48722010000400003] [ Links ]
12. Sanjar FA, Queiroz BE, Miziara ID. Otolaryngological manifestations in HIV - clinical aspects and treatment. Braz J Otorhinolaryngol 2011;77(3):391-400. [http://dx.doi.org/10.1590/S1808-86942011000300020] [ Links ]
Accepted 11 April 2013
 Correspondence: M Tshifularo (mashudu.tshifularo@up.ac.za)
Correspondence: M Tshifularo (mashudu.tshifularo@up.ac.za)

