










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSAMJ: South African Medical Journal
versão On-line ISSN 2078-5135
versão impressa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.103 no.5 Pretoria Mai. 2013
RESEARCH
Risk of nevirapine-associated Stevens-Johnson syndrome among HIV-infected pregnant women: The Medunsa National Pharmacovigilance Centre, 2007 - 2012
N DubeI, II; E AdewusiIV; R Summers,V, III
IBSc (Microbiology and Biochemistry)MSc, MPH. Medunsa National Pharmacovigilance Centre, Medunsa Campus, University of Limpopo, Ga-Rankuwa, Gauteng, South Africa
IIBSc (Microbiology and Biochemistry)MSc, MPH. AIDS Unit, National Institute for Communicable Diseases, National Health Laboratory Services, Pretoria, South Africa
IIIBSc (Pharmacy), MSc, PhD, Department of Pharmacy, Faculty of Health Sciences, Medunsa Campus, University of Limpopo, Ga-Rankuwa, Gauteng, South Africa
IVBPharm, MSc, PhD Medunsa National Pharmacovigilance Centre, Medunsa Campus, University of Limpopo, Ga-Rankuwa, Gauteng, South Africa
VBSc (Pharmacy), MSc, PhD. Medunsa National Pharmacovigilance Centre, Medunsa Campus, University of Limpopo, Ga-Rankuwa, Gauteng, South Africa
ABSTRACT
BACKGROUND: Stevens-Johnson syndrome (SJS) is an acute life-threatening condition often elicited by drugs. The government's indecisiveness in deciding to stop the use of nevirapine (NVP) in HIV-infected pregnant women owing to the increase of SJS among this population group in South Africa prompted this investigation.
OBJECTIVES: To investigate if pregnancy is a risk factor for SJS among HIV-infected women taking NVP-containing regimens and registered within the Medunsa National Pharmacovigilance Centre database.
METHODS: A matched case-control study with 5:1 matching was conducted. Women with SJS (cases) taking NVP-containing regimens were matched with women without SJS (controls) taking NVP-containing regimens. Controls were randomly selected and matched to cases by hospital, age, treatment duration and CD4 count. Conditional logistic regression was used to determine if pregnancy was a risk factor forSJS.
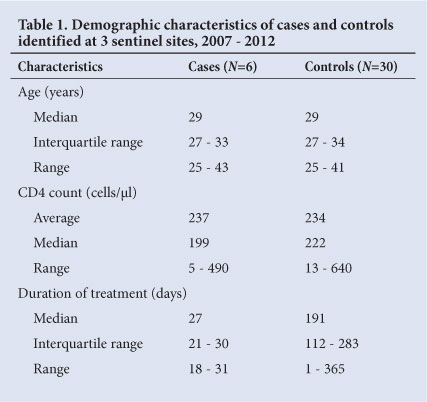
RESULTS: Six SJS cases were identified and 30 controls selected. The median age of both cases and controls was 29 years and the average CD4 counts were 237 and 234 cells/µl respectively. Subjects were on NVP treatment for 18 - 31 days before the onset of SJS. Controls did not develop SJS after treatment of between 1 and 365 days. Pregnancy increased the chances of developing SJS 14-fold (OR 14.28, p=0.006, 95% CI 1.54 - 131.82).
CONCLUSIONS: NVP-containing ARV regimens taken during pregnancy increase the risk of developing SJS. Healthcare workers are advised to offer informed consent to patients and recommend effective contraception methods if NVP treatment is considered. In the light of our findings, further studies of the association between NVP, pregnancy and SJS are necessary before general conclusions can be reached.
Toxic epidermal necrolysis (TEN) and Stevens-Johnson syndrome (SJS) are acute life-threatening conditions, most often elicited by drugs and less often by infection.[1] SJS and TEN are characterised primarily by acute skin blisters and mucous membrane erosions.[2]The main difference between the two conditions is the extent of skin detachment: <10% in SJS and >30% in TEN.[3] Cases with detachment of 10 - 30% are labelled as SJS-TEN overlap.[1] Both SJS and TEN are rare and have an incidence of approximately 2 per million population per year in Europe.[4,5]
Typically, the drug reaction develops within the first 6 weeks after the causative drug initiation.'1,6-91 Initial symptoms are cough, fever, sore throat and facial swelling. If not detected early, and the offending drug discontinued, skin rash may develop that leads to skin ulcers and skin sloughing. Death of the patient could result.[10]
Numerous drugs can cause SJS, with several antituberculosis drugs,[11] aromatic anticonvulsants (e.g. carbamazepine, phenobarbital and phenytoin), anti-inflammatory drugs (e.g. allopurinol, chlormezanone), anti-infective agents (e.g. aminopenicillins, sulphonamides, quinolones, cycline antibiotics)[7,12] and antiretroviral (ARV) medications (e.g. nevirapine (NVP), zidovudine (AZT), stavudine (d4T), indinavir, didanosine)'71 being some of the most frequent offending agents.
It is important to note that although the outcome of SJS is not significantly worsened by HIV infection, HIV-infected patients have a higher predisposition to the condition because of decreased anti-oxidant levels owing to infection.[13,14] In addition, the greater likelihood of such patients using the drugs at higher dosages than the general population, further predisposes them to SJS.'7,15]
Although the first ARV agent was licensed in 1987, South Africa (SA) only began antiretroviral therapy (ART) in 2003. At that time, ARV use was guided by the National Department of Health's Operational Plan for Comprehensive HIV and AIDS Care, Management, and Treatment; this plan was revised in 2010.'16-181 The revised plan states that all patients requiring ART must be initiated on first-line ARV regimens involving 3 ARVs in combination.'19,201 The recommended SA first-line regimens contain the following 3-drug combinations: d4T, AZT or tenofovir with lamivudine and efavirenz (EFV) or NVP. Of these ARVs, NVP has been implicated as the cause of SJS in HIV-infected patients.[6,7,12,21]
In 1998, Barner and Myers from Boehringer Ingelheim Pharmaceuticals Inc. publicly acknowledged that NVP might cause SJS in some patients.'81 This adverse drug reaction is described in the labelling of NVP produced by this company, as well as that produced by other pharmaceutical companies, such as Cipla. A prominent warning to reduce the risk of rash of any severity (including SJS) is also specified on NVP package inserts, whereby a 2-week lead-in dose (200 mg once daily) is recommended. Furthermore, it is specified that the NVP dose should not be increased during the lead-in period until any rash that develops, has resolved. Reported risk factors for SJS include female sex, history of drug allergy, low body weight, high NVP plasma level and CD4 counts >250 cells/ul in women and >400 cells/µl in men. [6,22] The revised SA plan on the use of ARVs recommends the use of NVP, even at a CD4 count >250 cells/ul in pregnant women,[19,20] in line with the World Health Organization (WHO)'s contention that benefits outweigh risks of using the drug at a high CD4 count.
Recently, we became aware of a possible increase in risk of SJS among HIV-infected pregnant women taking NVP-containing ARV regimens in KwaZulu-Natal Province. This is a new observation, as pregnancy has not been specified by pharmaceutical companies as a risk factor for skin reactions. This increase in SJS incidence led to the release of a directive by the SA National Department of Health on 6 April 2012 (later retracted owing to lack of sufficient evidence) stating the following: (i) When initiating non-pregnant HIV-positive women of reproductive age on highly active ART (HAART), use EFV; (ii) when initiating treatment on HIV-positive pregnant women, use EFV if commencing treatment during the second trimester; (iii) delay initiation of treatment until the second trimester even in those women who need HAART and present during their first trimester; (iv) for HIV-positive pregnant women already on EFV as part of a HAART regimen, continue with EFV.
We investigated whether pregnancy was a risk factor for SJS among HIV-infected women monitored by the Medunsa National Pharmacovigilance Centre and taking NVP-containing regimens.
Methods
Study setting and study design
A matched case-control study with 5:1 matching was conducted at 3 sentinel sites in the SA public health sector, located in Gauteng, Mpumalanga and Limpopo provinces. The study population comprised HIV-infected women >15 years old who had been taking NVP-containing ARV regimens and whose details were available on the Medunsa Pharmacovigilance Centre database. Excluded from the study population were women on the Prevention of Mother To Child Transmission (PMTCT) programme and women not taking NVP-containing regimens.
Cases were those women who developed SJS within a period of 3 - 46 days (6 weeks) after HAART initiation and were diagnosed as having SJS by the attending physician as stated on the case report form (CRF) or adverse drug reaction (ADR) form.
Controls were the population of reports not selected as cases and reported over a 5-year period where the subject was a woman on NVP-containing regimens and not diagnosed as having SJS. Controls were matched for age (within 5 years of the case), CD4 count (<250 cells/ml or >250 cells/ml), and duration of NVP treatment (within one year of case). As there were no controls available with a closer match for duration of NVP treatment to that of cases (i.e. 3 - 46 days), a maximum of one year of treatment duration was used for controls.
Pregnancy status during NVP treatment was recorded for both the cases and the controls.
Data collection
All female patients taking NVP-containing regimens as part of HAART were selected from the database. All patients with 'Stevens-Johnson syndrome' stated in the adverse drug reaction column were selected as cases. To ensure that no SJS cases were missed, ADR forms were simultaneously reviewed, and additional cases found that met the inclusion criteria were classified as cases.
Controls were selected among the female patients taking NVP-containing regimens as part of HAART who had not been selected as cases. The selection of controls was based on the assumption that women taking NVP-containing regimens who were reported for an adverse event other than SJS were representative of all women taking NVP who had not been reported for SJS. For each case, the following procedure was performed in selecting appropriate controls: The age group, CD4 count and duration of treatment of the case were identified and a subset of potential controls was selected such that all elements had the same age group (within ±5 years of the case), CD4 count (<250 cells/ml or >250 cells/ml) and duration of treatment (within ±1 year of the case) characteristics of the case. This process was carried out using Stata's 'Keep' command for each of the cases. One file resulted for each case and its controls. Stata's random sampling function was then used to select a random sample of 5 controls from each of the case files, in turn.
Data management and analysis
An algorithm for implicating a drug as the cause of an adverse drug reaction, described by Roujeau and Stern, was used to implicate NVP as the cause for SJS in this study:'11
1. Alternative causes (e.g. concomitant medication) were excluded.
2. The interval between the introduction of a drug and the onset of a reaction was examined (for drug-induced SJS, 3 - 46 days was applied).
3. Any improvement after drug withdrawal was noted.
4. Any reaction if the drug were re-administered was noted. Conditional logistic regression analysis was performed on STATA version 12 (StataCorp LP, College Station, TX, USA). Odds ratios, chi-square and 95% confidence intervals (CIs) were also computed. A p-value <0.05 was considered statistically significant.
Ethical approval
The project proposal, which includes the work described in this paper, was approved by the Medunsa Research and Ethics Committee of the University of Limpopo in 2006.
Results
Of the 2 664 patients enrolled from the 3 facilities during the study period, 10.4% (278/2 664) of female patients were taking NVP-containing regimens. Of these patients, 6 SJS cases (6/278 (2.2%)) were identified from the database and ADR forms. Three cases were from Hospital A, 2 from Hospital B and 1 from Hospital C. The demographic characteristics of these 6 cases and 30 controls are shown in Table 1. Controls were selected to be as similar as possible to the cases; however, the cases were on treatment for between 3 and 46 days before developing SJS.
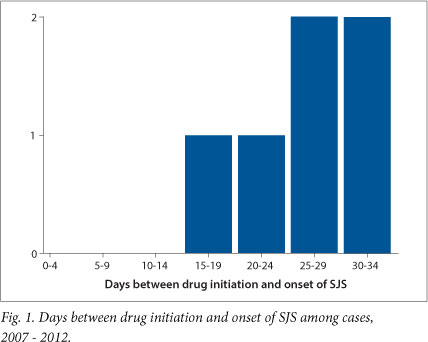
Onset of SJS ranged from 18 to 31 days after initiation of NVP, with the highest frequency of patients experiencing SJS signs and symptoms after 24 days of drug administration (Fig. 1). For all cases, NVP was stopped and an alternative drug substituted, following which all SJS signs and symptoms subsided.
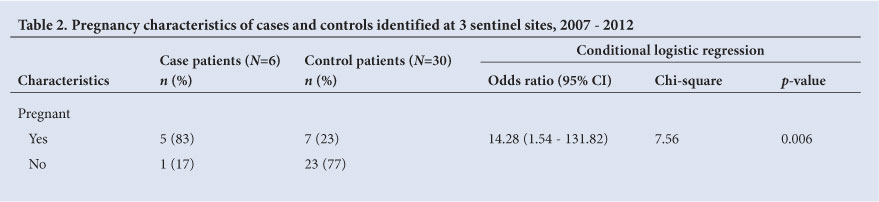
The characteristics of cases and controls with respect to pregnancy are shown in Table 2. Pregnancy increased the chances of developing SJS 14-fold (OR 14.28). This association was highly significant (p=0.006) despite the CI being wide owing to the small sample size (95% CI 1.54 - 131.82).
Discussion
Drug causality of SJS is easy to postulate but difficult to prove, particularly in HIV-infected patients on combination therapy and other concomitant medicines. The toxicity of NVP during pregnancy has not been measured in large cohorts and, for those who have measured it, results are contradictory. Our results were based on attending physician diagnoses as logged in our CRF and ADR forms as well as a causality algorithm described by Roujeau and Stern.
Our findings show that the chance of developing SJS increases with pregnancy. This finding contradicts results found by Marazzi et al. (2006)[23] that NVP-containing regimens in pregnant women appear to be safe in African settings. In SA, most HIV-infected patients are initiated on an EFV-containing regimen and continue on that course unless they exhibit an adverse reaction. Patients who are pregnant, HIV-infected and in need of ARVs for their own health, are fast-tracked and initiated on an NVP-containing regimen. The standard prescribing practice is to switch patients from an EFV- to a NVP-containing regimen when they become pregnant, owing to possible teratogenicity that is attributed to EFV. This practice of prescribing NVP to pregnant women may account for the fact that these women are at a higher risk of developing SJS than the general population of women.
A weakness of this study was the small sample size which limited our study power. In addition, there were no controls available with a closer match for duration of NVP treatment to that of cases; consequently, a longer treatment duration for controls was used. In view of these weaknesses and our findings, further studies of this important matter are necessary before general conclusions can be reached. In addition to studying the association between SJS, NVP and pregnancy, the teratogenic effects of EFV should be thoroughly investigated to allow the SA National Department of Health to make an informed decision regarding safety of NVP in pregnancy.
Conclusion
The present analysis was performed to confirm or disprove suspicions of increased SJS among pregnant women taking NVP-containing regimens. Our investigation confirms this suspicion. Healthcare workers must therefore be advised to offer informed consent to the patient and recommend effective appropriate contraception methods if NVP treatment is considered. All other patients on NVP-containing regimens must be equally closely monitored and NVP discontinued immediately if side-effects are experienced. Further studies are needed before the SA National Department of Health will be able to reach conclusions regarding NVP safety in pregnancy.
Acknowledgements. We acknowledge support from the SA National Department of Health. The Foundation for Professional Development contributed to the development of the database. Professor Mojakgomo H Motswaledi assisted with obtaining patient files of SJS cases. Professor Brendan V Girdler-Brown assisted with advice on the statistical analysis of the results. Dr Theresa Rossouw assisted with the review of this manuscript. The contents of this manuscript are solely the responsibility of the authors.
Authors' contributions. N Dube and R Summers conceived this study. N Dube and E Adewusi reviewed ADR forms and CRFs and undertook data extraction. N Dube was involved in the statistical analysis and the interpretation of the results. All authors participated in the preparation and revision of this study.
References
1. Kumar PNS, Thomas B, Kumar K, Kumar S. Stevens-Johnson syndrome - toxic epidermal necrolysis (SJS-TEN) overlap associated with carbamazepine use. Indian J Psychiatry 2005;47(2):121-123. [http://dx.doi.org/10.4103/0019-5545.55961] [ Links ]
2. Chen KT, Twu SJ, Chang HJ, Lin RS. Outbreak of Stevens-Johnson syndrome/toxic epidermal necrolysis associated with mebendazole and metronidazole use among Filipino laborers in Taiwan. Am J Public Health 2003;93(3):489-492. [http://dx.doi.org/10.2105/AJPH.93.3.489] [ Links ]
3. Fagot JP, Mockenhaupt M, Bouwes-Bavinck JN, Naldi L, Viboud C, Roujeau JC. Nevirapine and the risk of Stevens-Johnson syndrome or toxic epidermal necrolysis. AIDS 2001;15(14):1843-1848. [http://dx.doi.org/10.1097/00002030-200109280-00014] [ Links ]
4. Pereira F, Mudgil A, Rosmarin D. Toxic epidermal necrolysis. J Am Acad Dermatol 2007;56:181-200. [http://dx.doi.org/10.1016/j.jaad.2006.04.048] [ Links ]
5. Bastuji-Garin S, Zahedi M, Guillaume JC, Roujeau JC. Toxic epidermal necrolysis (Lyell syndrome) in 77 elderly patients. Age Ageing 1993;22(6):450-456. 'http://dx.doi.org/10.1093/ageing/22.6.4501 [ Links ]
6. Metry DW, Lahart CJ, Farmer KL, Hebert AA. Stevens-Johnson syndrome caused by the antiretroviral drug nevirapine. J Am Acad Dermatol 2001;44(2):354-357. 'http://dx.doi.org/10.1067/ mjd.2001.1018851 [ Links ]
7. Rotunda A, Hirsch RJ, Scheinfeld N, et al. Severe cutaneous reactions associated with the use of human immunodeficiency virus medications. Acta Derm Venereol 2003;83(1):1-9. 'http://dx.doi.org/10.1080/000155503100026111 [ Links ]
8. Barner A, Myers M. Nevirapine and rashes. Lancet 1998;351(9109):1133. http://dx.doi.org/10.1016/ S0140-6736(05)79417-41 [ Links ]
9. Yap FBB, Wahiduzzaman M, Pubalan M. Stevens-Johnson syndrome (SJS) and Toxic epidermal necrolysis (TEN) in Sarawak: A four years' review. EDOJ 2008;4(1):13. [ Links ]
10. Ghislain PD, Roujeau JC. Treatment of severe drug reactions: Stevens-Johnson syndrome, toxic epidermal necrolysis and hypersensitivity syndrome. Dermatol Online J 2002;8(1):5. [ Links ]
11. Kannenberg SMH, Jordaan HF, Koegelenberg CFN, Von Groote-Bidlingmaier F, Visser WI. Toxic epidermal necrolysis and Stevens-Johnson syndrome in South Africa: A 3-year prospective study. Q J Med 2012;105(9):839-846. 'http://dx.doi.org/10.1093/qjmed/hcs0781 [ Links ]
12. Mockenhaupt M, Liboud C, Dunant A, et al. Stevens-Johnson syndrome and toxic epidermal necrolysis: Assessment of medication risks with emphasis on recently marketed drugs. The EuroSCAR- study. J Invest Dermatol 2008;128(1):35-44. 'http://dx.doi.org/10.1038/sj.jid.57010331 [ Links ]
13. Saiag P, Caumes E, Chosidow O, Revuz J, Roujeau JC. Drug-induced toxic epidermal necrolysis (Lyell syndrome) in patients infected with the human immunodeficiency virus. J Am Acad Dermatol 1992;26(4):567-574. 'http://dx.doi.org/10.1016/0190-9622(92)70082-Q1 [ Links ]
14. Moreno-Ancillo A, Lopez-Serrano MC. Hypersensitivity reactions to drugs in HIV-infected patients. Allergic evaluation and desensitization. Clin Exp Allergy 1998;28:57-60. [ Links ]
15. Porteous DM, Berger TG. Severe cutaneous drug reactions (Stevens-Johnson syndrome and toxic epidermal necrolysis) in human immunodeficiency virus. Arch Dermatol 1991;127(5):740-741. http://dx.doi.org/10.1001/archderm.1991.016800401520241 [ Links ]
16. World Health Organization. Rapid advice: Antiretroviral therapy for HIV infection in adults and adolescents. 2009. http://www.who.int/hiv/pub/arv/rapid_advice_art.pdf (accessed 9 December 2012). [ Links ]
17. Mahumane C, Dube NM, Mayayise G, Summers S. An Overview of the Demographic Data from the Structured Surveillance Study. Ga-Rankuwa: Medunsa National Pharmacovigilance Centre, 2011. [ Links ]
18. National Department of Health. South African National Antiretroviral Treatment Guidelines (2010). Pretoria: National Department of Health, 2010. http://www.uj.ac.za/EN/CorporateServices/ioha/ Documentation/Documents/ART%20Guideline.pdf (accessed 9 May 2012). [ Links ]
19. National Department of Health. Clinical Guidelines for the Management of HIV & AIDS in Adults and Adolescents. Pretoria: Department of Health, 2010. http://www.fidssa.co.za/Guidelines/2010_Adult_ ART_Guidelines.pdf (accessed 9 December 2012). [ Links ]
20. World Health Organization. Antiretroviral Drugs for Treating Pregnant Women and Preventing HIV Infection in Infants: Towards Universal Access. Geneva: World Health Organization, 2010. http:// whqlibdoc.who.int/publications/2010/9789241599818_eng.pdf (accessed 9 December 2012). [ Links ]
21. Namayanja GK, Nankya JM, Byamugisha JK, et al. Stevens-Johnson syndrome due to nevirapine. Afr Health Sci 2005;5(4):338-340. [ Links ]
22. Manosuthi W, Sungkanuparph S, Tansuphaswadikul S, et al. Incidence and risk factors of nevirapine-associated skin rashes among HIV-infected patients with CD4 cell counts <250 cells/microL. Int J STD AIDS 2007;18(11):782-786. 'http://dx.doi.org/10.1258/0956462077822122891 [ Links ]
23. Marazzi MC, Germano P, Liotta G, et al. Safety of nevirapine-containing antiretroviral triple therapy regimens to prevent vertical transmission in an African cohort of HIV-1-infected pregnant women. HIV Med 2006;7(5):338-344. [http://dx.doi.org/10.1111/j.1468-1293.2006.00386.x+] [ Links ]
Accepted 21 January 2013.
 Correspondence: N Dube (nmgumede@yahoo.com)
Correspondence: N Dube (nmgumede@yahoo.com)


{kind=link}