










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSAMJ: South African Medical Journal
versão On-line ISSN 2078-5135
versão impressa ISSN 0256-9574
SAMJ, S. Afr. med. j. vol.103 no.5 Pretoria Mai. 2013
RESEARCH
High uptake of Gardasil vaccine among 9 - 12-year-old schoolgirls participating in an HPV vaccination demonstration project in KwaZulu-Natal, South Africa
I MoodleyI; N TathiahI; V MubaiwaII; L DennyIII
IPhD. Department of Public Health Medicine, University of KwaZulu-Natal, Durban, South Africa
IIMB ChB, FCPHM (SA). Provincial Department of Health, Pietermaritzburg, South Africa
IIIMB ChB, MMed (OG), PhD, FCOG (SA). Department of Obstetrics and Gynaecology, Faculty of Health Sciences, University of Cape Town, South Africa
IVBSc (Hons), MB ChB, Dip HIV Man (SA), MS (Epi). Department of Public Health Medicine, University of KwaZulu-Natal, Durban, South Africa
ABSTRACT
BACKGROUND: Cervical cancer is linked to infection of the cervix by oncogenic human papillomavirus (HPV) subtypes. The quadrivalent Gardasil vaccine (against HPV types 6, 11, 16, 18), recommended in girls 9 - 12 years of age, has been shown to be safe, immunogenic and efficacious, with minimal or no side-effects.
AIM: To demonstrate the capacity of school health teams to carry out vaccinations within a school environment.
OBJECTIVES: To assess the uptake of 3 doses of the vaccine, document lessons learnt and provide recommendations for a national rollout of school-based HPV vaccination for learners.
METHODS: Female learners (age 9 - 12 years) from 31 primary schools in Nongoma and Ceza districts (KwaZulu-Natal province, South Africa) were identified for inclusion in the vaccination programme. The 3 doses of vaccine were administered by existing school health teams. Education and training sessions were held with all stakeholders: provincial departments of health and education; school health teams; primary healthcare nurses; hospital doctors and nurses; private practitioners; school principals, teachers and governing bodies; parents; and community and traditional leaders.
RESULTS: The overall uptake of the vaccine was found to be high: 99.7%, 97.9% and 97.8% for the first, second and third doses respectively ( N=963). No adverse events were attributed to the HPV vaccine.
CONCLUSION: This project demonstrated the successful implementation of HPV vaccination among learners (ages 9 - 12 years) using school health teams.
Globally, cervical cancer is the secondmost common cancer among women, with an estimated 529 409 new cases and 274 883 deaths reported in 2008.[1] Approximately 86% of cases occur in developing countries, and represent 13% of all cancers affecting women.[1]
In South Africa (SA), cervical cancer is the secondmost frequent cancer among all women, with a crude incidence rate of 22.8 cases per 100 000 women.[1] Current estimates indicate that 5 743 women are diagnosed with cervical cancer annually; with 3 027 women dying from the disease annually.[1] Approximately 21% of women in the general population are estimated to harbour cervical human papillomavirus (HPV) at any time, and 62.8% of invasive cervical cancers are attributed to HPV oncogenic types 16 or 18.[1] Individuals infected with HIV are at an increased risk for HPV-related cancers.[2]
Globally, the prevalence of genital warts is high, especially in people living with HIV.[3] Though there is little information on incidence, genital warts are common among sexually active people and usually first occur in adolescence.[3] Genital warts are highly infectious, with a transmission rate of 65% within sexual partnerships; despite treatment, they can recur in up to 75% of cases[4] HPV types 6 and 11 are linked to genital warts, with 20 - 50% of lesions also co-infected with high-risk HPV types.[4]
The development of the bivalent vaccine Cervarix (GlaxoSmithKline) (against HPV types 16 and 18),[5] and the quadrivalent vaccine Gardasil (MSD) (against HPV types 6, 11, 16 and 18)[6] represents a major breakthrough in the options available for the prevention of cervical cancer. Both vaccines have been shown to be safe, immunogenic and efficacious.[3,5,6] Although licensed for use in both the public and private healthcare sectors in SA, they are currently only available in the private sector.[1]
The quadrivalent Gardasil vaccine (used in the HPV demonstration project) is indicated in females (aged 9 - 26 years) for the prevention of cervical, vulvar, vaginal and anal cancers, as well as genital warts, and in males (aged 9 - 26 years) for the prevention of anal cancers and genital warts.[6]
Modelling studies estimate that vaccination of 70% of girls aged 9 - 12 years against HPV types 16 and 18, will result in a 43% reduction in the lifetime risk of cervical cancer.[7] Furthermore, the implementation of a strategy combining vaccination of young girls with screening programmes for women over 30 years, could lead to a 53 - 70% reduction in the lifetime risk of cancer, assuming 70% coverage for both.[7] At 100% coverage with vaccination alone, the reduction in the lifetime risk of cancer will be 61%; with the combination of vaccination and screening, this will increase to 75%.[8]
The World Health Organization has recommended that routine HPV vaccination be included in national immunisation programmes.3 Goldie et al. [8] have suggested that focusing existing resources on vaccinating girls, rather than dividing resources between girls and boys, is the most cost-effective way of reducing the lifetime risk of cancer in resource-constrained environments. In SA, the Extended Programme on Immunization (EPI), established in 1995, provides free vaccination of children against childhood diseases.[9] The service, which is available at public health facilities, targets mainly the under-6-year age group, however.[9]
For school-going children older than 6 years, the newly revised National School Health Policy and Implementation Guidelines intends to provide a comprehensive, integrated school health programme, as part of the primary healthcare package.[10] School health teams, comprising qualified nursing personnel, deliver interventions to learners in schools, and ensure that all learners have completed their vaccination schedules.[10]
The aim of our project was to demonstrate capacity to carry out vaccinations against HPV of female learners within the primary school environment, using the existing staff and infrastructure resources of the school health teams.
The objectives were to assess the uptake of 3 doses of the vaccine and to document lessons learnt, thus to provide recommendations for the establishment of HPV vaccination in schools.
Methods
Ethics and consent
Ethics approval for the HPV demonstration project was obtained from the institutional Human Research Ethics Committee at the University of Cape Town (UCT). Approval to conduct the project in the districts of Nongoma and Ceza was given by the KwaZulu-Natal (KZN) Provincial Department of Health (DoH). Written informed consent was obtained from parents/caregivers of the learners prior to starting vaccination.
Setting
The project was undertaken in the Zululand district of KZN. The district has an area of 14 810 km2 and a population of 964 005 people living in small isolated rural settlements or one of the 6 urban areas.[11] The district is characterised by widespread poverty, high HIV incidence, and poor access to basic services and facilities.
In consultation with the KZN DoH and Department of Education (DoE), it was determined that 1 000 female learners (aged 9 - 12, in grades 4 - 5) from 31 schools in the Nongoma and Ceza areas (18 in Nongoma and 13 in Ceza) would be vaccinated. The schools were chosen based on the number of learners in the schools and the proximity of schools to clinics. The vaccination schedule was administered at 0, 1 and 6 months, as per the recommended time intervals required between doses.
Stakeholder participation
The establishment of the HPV Vaccination Demonstration Project Working Group ensured the representation and participation of key stakeholders from UKZN, provincial and district Departments of Health and Education, and MSD.
The DoE provided the list of schools and the number of learners from each school who would participate in the vaccination programme. Meetings were held with the department to discuss the content of the communication materials for the learners to ensure that it was at the appropriate age, maturity and knowledge levels of the learners. Once confirmed and approved, information leaflets were translated into isiZulu, the local language. The material was also available in English.
Key stakeholders in Nongoma and Ceza were identified during visits to the sites prior to commencing vaccination. Information sessions were held with principals, teachers, school governing bodies, parents, community and religious leaders, traditional leaders, traditional healers, school health teams, hospital nurses and doctors, and private practitioners. Acceptance of the vaccination programme by these key stakeholders was considered necessary before the programme could be implemented. The training, educational and awareness material was tailored specifically towards the needs of these different groups of stakeholders.
Inclusion and exclusion criteria
The following were inclusion criteria for vaccination:
• signed informed consent from parent/caregiver
• learner to be in 9 - 12-year age group, or in grade 4 or 5 at time of vaccination
• learner to be afebrile and clinically well
• learner willing to return for further doses. The following were exclusion criteria:
• no signed informed consent from parent/caregiver available
• learners younger than 9 years of age, and older than 12, at the time of vaccination
• learner febrile and/or clinically unwell
• learner unable or unwilling to return for further doses.
Project implementation
Vaccination was performed by the school health teams comprising 4 staff members: a nursing sister, a registered nurse, and 2 enrolled nurses. The role of the nursing sister was to ensure that written informed consent from parents/caregivers was in place, as well as to perform a general clinical appraisal of the learner (measuring temperature, height, weight and mid-arm circumference). The registered nurse recorded the data on data collection forms. A follow-up card containing details of the vaccine, the schedule and date of the next dose was given to each learner.
If any learner reported any symptoms of ill-health, no vaccination was administered, and the learner was then referred to the nearest clinic or hospital. Follow-up measures were established for those learners who missed doses who needed to be vaccinated in the subsequent 2-week period.
The cold chain for the vaccination programme was reviewed and shortcomings identified and managed well in advance of the implementation. In this regard, refrigerators and freezers were purchased by MSD and donated to the district hospitals in Nongoma and Ceza. The vaccination distribution plan was matched to the schools list and the number of participating learners. The vaccines in cooler boxes with accompanying ice-packs were prepared by the pharmacy at the hospital and collected by the school health teams on the day of the vaccinations. Included in the first vaccine distribution packs were bags containing information leaflets on cervical cancer and screening. The quantities of vaccine and bags were recorded and reconciled at the end of each day by pharmacy staff.
Training and education
Training was provided for all healthcare personnel from the Nongoma and Ceza districts, and included the school health teams, primary healthcare nurses, hospital nurses (outpatients and paediatric), doctors and community health workers.
Awareness, information and education sessions on cervical cancer, screening and the HPV demonstration project were conducted with school principals, governing bodies and teachers. Thereafter, teachers set up meetings with the grade 4 and 5 learners to explain the project, and to obtain informed consent from parents, who received information leaflets, well in advance of the vaccination date.
Data collection and reporting of adverse events
Multi-level data collection tools for reporting of adverse events were developed and reviewed by the project team and relevant stakeholders, comprising:
• observation for 15 minutes post vaccination by school health nurses in designated observation areas
• observation by teachers in classroom post vaccination
• follow-up regarding any adverse events, with school health teams visiting schools a few days post vaccination
• follow-up of vaccinated learners with school health teams carrying out community visits, where feasible
• a telephone number was provided so that MSD could be notified immediately regarding any adverse event
• the DoH EPI adverse event reporting protocol, already in existence, was also used
• doctors who consulted in the private sector in Nongoma and Ceza were notified of the vaccination project, and were asked to alert the DoH if called upon to treat any learner experiencing side-effects post vaccination.
Linkage to the provincial cervical cancer screening programme
The HPV vaccine demonstration project is seen as part of a comprehensive cervical cancer prevention and treatment programme being planned in KZN. Linkage to the cervical cancer screening programme was planned in the following manner: parents and learners were provided with educational material about cervical cancer, screening and prevention; and female members of the community were encouraged to have Pap smears at their local clinics.
Results
Vaccination commenced on 7 March 2011, followed by the second dose on 4 May 2011 and the third dose on 17 October 2011. Of the initial selection of 1 000 learners, a final total of 963 participated (423 from Ceza and 540 from Nongoma). Their ages ranged from 7 to 14 years. For this analysis, data for 959 learners were analysed (4 had missing data on age). The mean age was 9.88 years, median 10 years and mode 9 years. The youngest learner was 7 years old and the oldest was 14 years. Most of the learners were in the age categories 9, 10, 11 and 12 years. Most (94%) of the learners were from grades 4 (69.5%) and 5 (24.4%). There were 17 missing values (1.8% of the total). However, 49 learners (5.1%), who were ineligible owing to age (<9 years or >12 years) were also vaccinated, and included in the analysis.
Table 1 shows the number of learners who received their first, second and third doses of vaccine in each district. A total of 960 learners (99.7%) received their first dose of vaccine (99.4% in Nongoma;100% in Ceza). A total of 943 learners (97.9%) received their second dose of vaccine (97.6% in Nongoma; 98.4% in Ceza).
A total of 938 learners (97.8%) received their third dose of vaccine (97.6% in Nongoma 98.1% in Ceza).
Two adverse events were reported. On investigation by the DoH, the 2 cases were diagnosed as chicken pox and an abdominal abscess respectively; following evaluation, neither was found to be related to the HPV vaccine.
Although the initial target was 1 000 learners, 963 learners were finally vaccinated as there were challenges in tracking the exact numbers of learners in particular ages and grades. Even after commencement of the school year, there was still movement of learners between schools in the two districts. There was a wide range of age categories (7 - 14 years) and grades (2 - 9), despite the strict inclusion and exclusion criteria. The vaccination of 49 learners, despite being ineligible due to age, was attributed to administrative oversights during the enrolment process.
Anthropometric data, not shown in this article, will be reported in a separate publication.
Discussion
A total of 963 female learners from 31 schools in Nongoma and Ceza participated in the HPV demonstration project. Overall, the uptake of the vaccine was high for all 3 doses (99.7%, 97.9% and 97.8% respectively). The high uptake of vaccine in this project is comparable with the results from other studies worldwide. A 2008 HPV vaccination study in Bolivia, which vaccinated 3 900 girls, showed 99.7%, 99.2% and 97.1% uptake for doses 1, 2 and 3 respectively.[12] In Uganda, the results of the HPV vaccination project held in 2008 - 2009 also showed a high uptake; in 2008, 99.6% of 3 459 girls received the first dose; and 87.8% completed all 3 doses; while in 2009, 93.2% of 2 385 girls received their first dose, and 86.3% completed all 3 doses.[13] Vaccination coverage in school-based programmes was 82.6% in Peru, 88.9% in 2009 in Uganda, and 96.1% in 2009 in Vietnam.[14] In India, a campaign approach achieved 77.2 - 87.8% coverage, whereas monthly delivery achieved 68.4 - 83.3% coverage.[14]
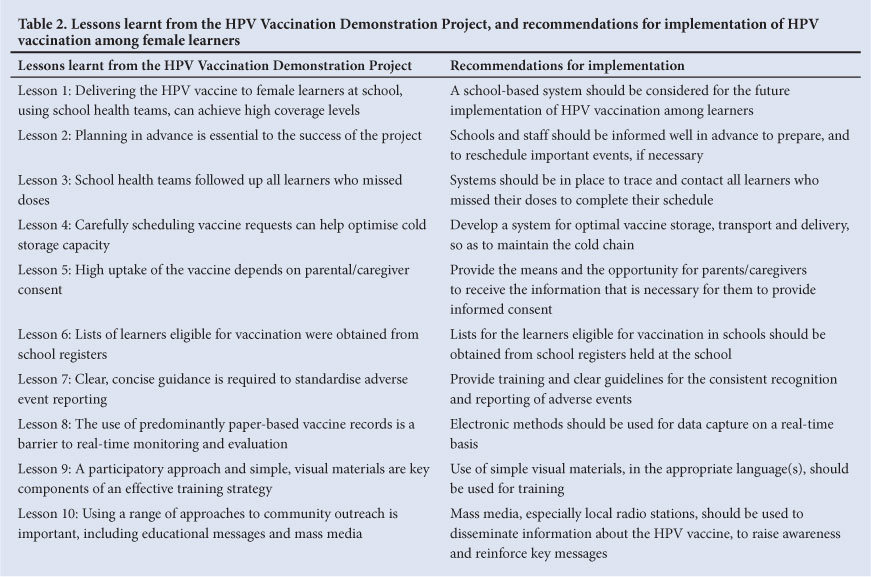
Table 2 lists the lessons learnt during the HPV Vaccination Demonstration Project, and specific recommendations for the future implementation of HPV vaccination among female learners.
Conclusion
The HPV Demonstration Project has shown a high uptake of the vaccine, using the delivery model of school health teams undertaking the vaccination of learners in schools. The lessons and the recommendations from this demonstration project are relevant to the plan for a national rollout of school-based HPV vaccination, as part of the integrated DoH primary healthcare and school health programmes.
Acknowledgements. The authors thank the following members of the HPV Vaccination Demonstration Project Working Group for their technical contributions: Janet Dalton, Thabisile Dlomo, John Friggens, Zanele Hadebe, Lynette Julius, Masothole Langa, Rani Manickum, Mavis Nkosi, Oliver Pillay, Lenore Spies, Bawinile Tembe and Thandie Vilakazi (Department of Health); and E Minlah and M Mdlalose (Department of Education). We also thank MSD (South Africa) for the donation of 3 000 doses of Gardasil vaccine, for fridges for vaccine storage, and travel and subsistence costs related to the HPV Vaccination Demonstration Project; and we thank the school health teams, learners and their parents/caregivers, and community members for their participation in this project.
References
1. WHO/ICO Information Centre on HPV and Cervical Cancer (HPV Information Centre). Human Papillomavirus and Related Cancers in South Africa. Summary Report. Geneva: World Health Organization, 2010. http://www.who.int/hpvcentre (accessed 11 October 2010). [ Links ] South African HPV Advisory Board. Prophylactic HPV vaccination against cervical cancer: a summarised resource for clinicians. S Afr J Gynaecol Oncol 2011;3(1):39-42. [ Links ]
2. WHO. Human papillomavirus vaccines: World Health Organization position paper. Geneva: World Health Organization, 2009. http://www.who.int/wer/2009/wer8415.pdf (accessed 17 August 2012). [ Links ]
3. Denny L. Human papillomavirus infections: Epidemiology, clinical aspects and vaccines. The Open Infectious Diseases Journal 2009;3:135-142. [ Links ]
4. GlaxoSmithKline. Prescribing Information - Cervarix. 2011. http://www.cervarix.com (accessed 17 August 2012). [ Links ]
5. Merck & Co. Prescribing Information - GardasiL 2011. http://www.gardasil.com (accessed 17 August 2012). [ Links ]
6. Sinanovic E, Moodley J, Barone MA, Mall S, Cleary S, Harries J. The potential cost-effectiveness of adding a human papillomavirus vaccine to the cervical cancer screening programme in South Africa. Vaccine 200937(44):6196-6202. [http://dx.doi.org/10.1016/j.vaccine.2009.08.004; [ Links ]
7. Goldie SJ, Kohli M, Grima D, et al. Projected clinical benefits and cost-effectiveness of a human papillomavirus 16/18 vaccine. J Natl Cancer Inst 2004;96(8):604-615. [http://dx.doi.org/10.1093/jnci/ djh104] [ Links ]
8. National Department of Health. Vaccinators Manual 2005. Pretoria: National Department of Health, 2005. [ Links ]
9. National Department of Health. National School Health Policy and Implementation Guidelines 2011. Pretoria: National Department of Health, 2011. [ Links ]
10. Zululand District Municipality. Draft Integrated Development Plan: 2012 - 2016. http://www.zululand.org.za/media/3109/ZDM%20Draft%20IDP%202012-2013_1.pdf (accessed 11 October 2012). [ Links ]
11. CIES. Developing a Management Model for Cervical Cancer Vaccination. 2010. http://www. cervicalcanceraction.org/newsletters/2010-07/HPVvac_demoproj_Bolivia_Jan2010.pdf (accessed 11 October 2012). [ Links ]
12. PATH and UNEPI. HPV Vaccination Demonstration Project in Uganda: Results, Lessons Learnt and Recommendations. 2010 http://www.chdc.mak.ac.ug/publications/HPV%20Vaccine%20 Demonstration%20Project%20in%20Uganda.pdf (accessed 11 October 2012). [ Links ]
13. LaMontagne DS, Barge S, Le NT, et al. Human papillomavirus vaccine delivery strategies that achieved high coverage in low- and middle-income countries. Bull World Health Organ 2011;89:821-830B. http://dx.doi.org/10.2471/BLT.11.08986] [ Links ]
Accepted 23 October 2012.
 Correspondence: I Moodley (moodleyi15@ukzn.ac.za)
Correspondence: I Moodley (moodleyi15@ukzn.ac.za)


{kind=link}
{kind=link}